Sentinal lymphnode
Reading File
Finding Sources
Finding Sources
Searching PubMed
"sentinel lymph node" biopsy
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the Sentinel Lymph Node (SLN) concept, technique, and clinical applications.
Sentinel Lymph Node (SLN)
Definition
The sentinel lymph node is the first lymph node (or group of nodes) to receive lymphatic drainage from a primary tumor site. It acts as the initial filter, and is therefore the node most likely to harbor metastatic disease if lymphatic spread has occurred. The goal of SLN biopsy (SLNB) is to identify and remove this node in the least invasive way, so that if it is negative, a full lymph node dissection - with its significant morbidity - can be avoided.
"The first node to receive drainage from the tumor site is termed the sentinel node. This node is the node most likely to contain metastases, if metastases to that regional lymph node basin are present." - Schwartz's Principles of Surgery, 11th Ed.
History
SLNB was introduced by Dr. Donald Morton in 1992 for cutaneous melanoma. It has since become standard practice across multiple malignancies, including breast cancer, head and neck cancers, and gynecological cancers.
- Sabiston Textbook of Surgery
Concept & Rationale
- Lymphatic drainage from a tumor follows a predictable (though not always anatomically intuitive) pathway.
- The SLN is the gateway: if cancer cells have spread via lymphatics, they are captured here first.
- If the SLN is negative on histopathology, the remaining regional nodes are almost certainly negative - avoiding full node dissection.
- If the SLN is positive, the surgeon proceeds to formal regional lymph node dissection (LND).
- This avoids morbidity (lymphedema, nerve injury, seroma) in patients whose nodes are truly negative.
Tracer Agents Used
Two complementary methods are used together for the highest detection rate:
| Agent | Type | Notes |
|---|---|---|
| Technetium-99m sulfur colloid | Radioactive tracer | Injected the day before or day of surgery; detected by gamma probe |
| Isosulfan blue dye or methylene blue | Vital dye | Injected in OR; identified visually as blue-stained channels/nodes |
| Indocyanine green (ICG) | Fluorescent dye | Increasingly used; detected by near-infrared camera |
- The combination of radioactive colloid + blue dye is more accurate than either alone.
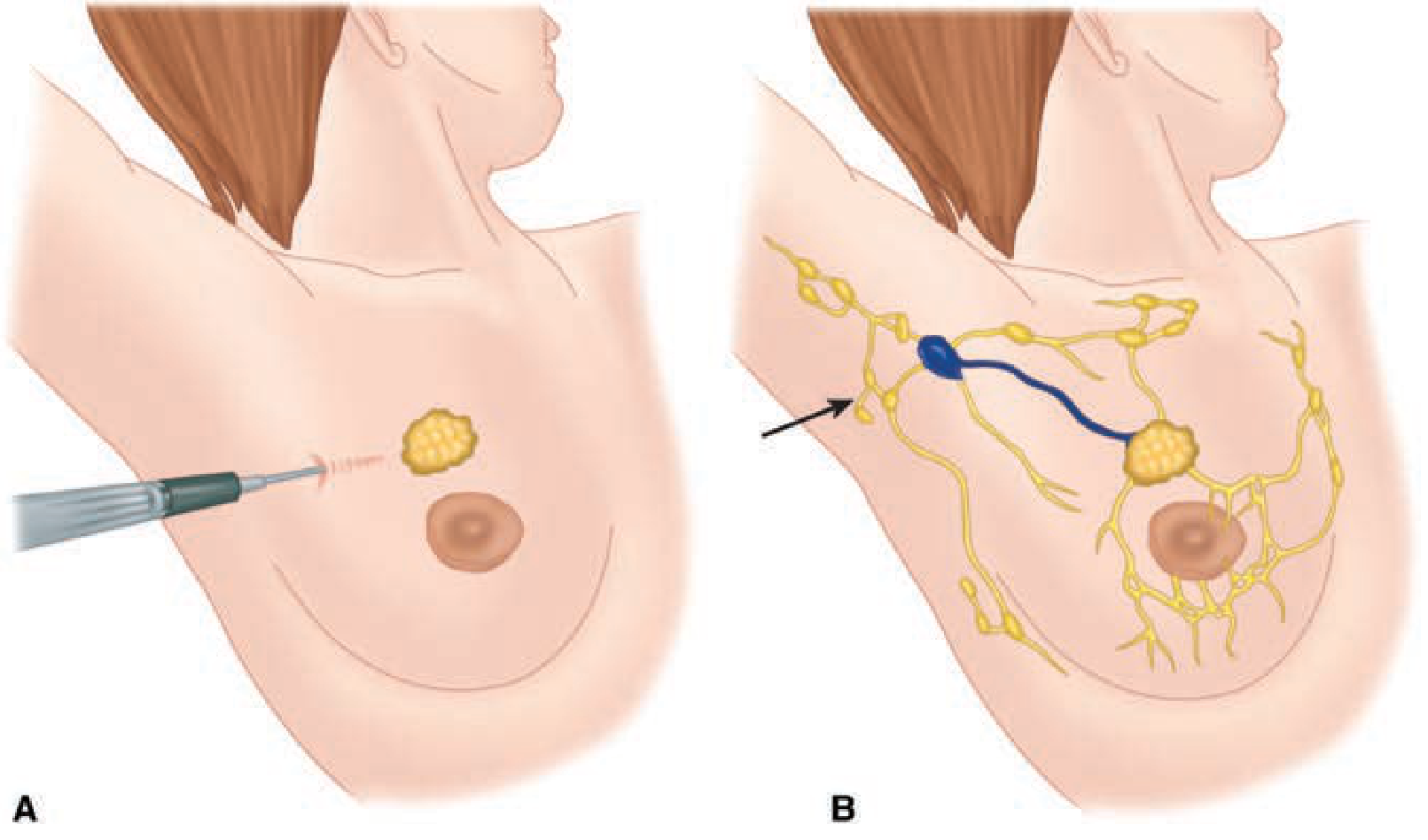
- For melanoma: tracer is injected intradermally around the lesion/biopsy scar (raising a wheal). Subcutaneous injection is a common error and will fail to identify an SLN.
- For breast cancer: tracer is injected peritumorally, subareolarly, or subdermally near the primary tumor.
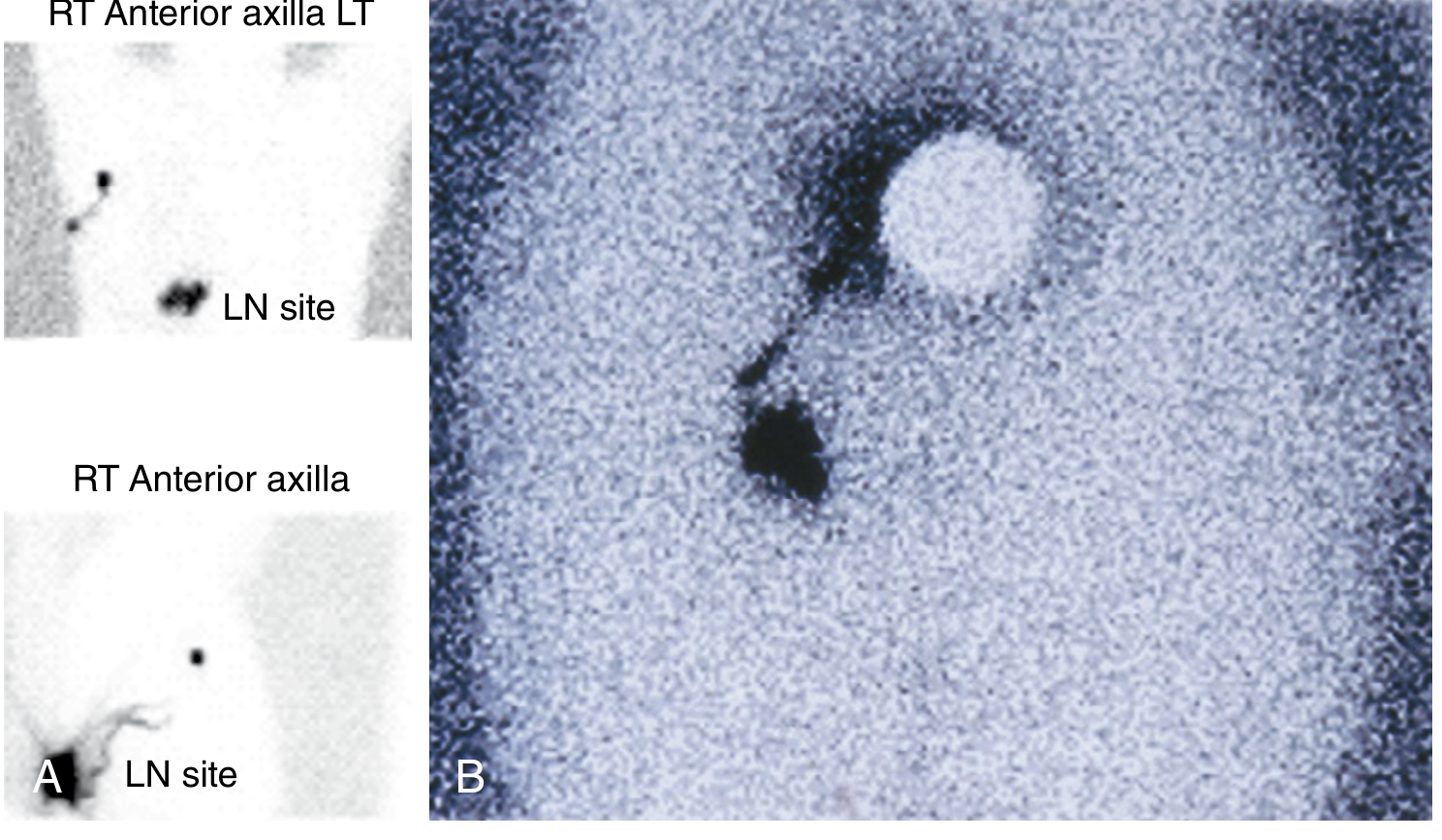
Preoperative Lymphoscintigraphy
- Performed on the day before or day of surgery.
- A gamma camera produces dynamic and static images identifying lymphatic channels and sentinel nodes.
- Especially important for melanoma on the trunk, head, or neck - where lymphatic drainage is unpredictable and may drain to more than one basin.
- Can identify interval/in-transit nodes (found between the primary and the main nodal basin), which carry the same risk of harboring metastasis and must be removed.
Surgical Technique (Breast Cancer)
- Radioactive colloid (0.5 mCi Tc-99m sulfur colloid for same-day; 2.5 mCi if injected the day before) is injected around the tumor or in the subareolar region.
- In the OR, 3-5 mL of blue dye is injected peritumorally or subareolarly.
- A hand-held gamma probe is used transcutaneously to locate the "hot" node.
- A 3-4 cm incision is made in the lower axilla; blue lymphatic channels are followed to the SLN.
- All nodes with radioactivity counts >10% of the hottest node ("10% rule") are removed.
- Careful manual palpation throughout minimizes the false-negative rate.
Histopathological Evaluation of the SLN
Removed nodes are examined with:
- Serial sectioning
- H&E staining (hematoxylin and eosin)
- Immunohistochemistry (IHC):
- S-100 protein and HMB-45 for melanoma
- Cytokeratin for breast cancer
- Molecular methods (RT-PCR) for ultrastaging are under investigation.
Nodes with isolated tumor cell deposits of <0.2 mm are classified as N0 by AJCC (6th edition) in breast cancer, though prognostic significance is debated.
Efficacy Metrics
Two criteria assess SLNB performance:
- Identification rate - proportion of patients in whom an SLN was successfully found and removed. Should be >95% with combined technique.
- False-negative rate (FNR) - proportion of patients with actual nodal metastases in whom the SLN was reported negative. Ranges 0-11% in study series; improves with surgical experience.
Meta-analysis by Tan et al. (449 cases, clinically node-negative disease): sensitivity 93%, FNR 7%, negative predictive value 94%, overall accuracy 95%.
- Schwartz's Principles of Surgery, 11th Ed.
Clinical Applications by Tumor Type
1. Breast Cancer
- Standard of care for clinically node-negative (N0) early breast cancer.
- Also accurate for larger T3N0 tumors (but ~75% of these will have nodal metastases on histology, so preoperative identification is preferred).
- Accurate for staging after neoadjuvant chemotherapy (in patients who were clinically N0 at presentation).
- Contraindications to SLNB:
- Inflammatory breast cancer
- Biopsy-proven nodal metastasis
- DCIS without mastectomy
- Prior axillary surgery
- Safe in pregnancy when performed with radioactive colloid alone (without blue dye).
2. Melanoma
- Required by AJCC for all melanomas >1.0 mm in thickness.
- SLN status is the single most important prognostic factor in melanoma without clinical nodal disease.
- Considered for T1 (thin) melanomas with high-risk features: ulceration, mitotic rate ≥1/mm², age <40 years, thickness 0.8-1.0 mm.
- Results directly guide adjuvant therapy decisions (e.g., immunotherapy, targeted therapy).
3. Merkel Cell Carcinoma (MCC)
- MCC has a much higher rate of occult nodal involvement (~30% for a 1.7 cm MCC) compared to melanoma.
- SLNB is a sensitive staging tool and is routinely recommended.
4. Head and Neck Cancer
- Used for oral cavity squamous cell carcinoma with clinically N0 neck.
- Lymphatic drainage patterns are especially unpredictable; lymphoscintigraphy is indispensable.
5. Other Cancers
- Gynecological cancers (endometrial, cervical): SLNB is increasingly used and validated.
- Penile cancer and some GI malignancies: emerging applications.
Complications
- Allergic reaction to blue dye (isosulfan blue): rare (1:10,000); can be anaphylactic. Some centers premedicate with antihistamines + steroids + H2 blocker.
- Skin tattooing or necrosis if methylene blue injected subdermally (use peritumorally instead).
- Lymphedema: significantly less than with full axillary dissection.
- Radiation exposure from Tc-99m is minimal and considered safe.
Recent Evidence (2025-2026)
- The 2025 ASCO Guideline Update on SLNB in early-stage breast cancer reviewed evidence supporting current practice (Park KU et al., J Clin Oncol, 2025) - PMID 40209128.
- A 2025 systematic review and meta-analysis found that SLNB alone (without completion axillary dissection) in patients with residual nodal disease after neoadjuvant chemotherapy has acceptable oncological outcomes - PMID 40811983.
- A 2026 Lancet Oncology meta-analysis assessed survival benefit from SLNB for melanoma, adding to the evidence that SLN status guides meaningful treatment decisions - PMID 41796592.
Summary Table
| Feature | Detail |
|---|---|
| First described | Donald Morton, 1992 (melanoma) |
| Key principle | First node in lymphatic drainage from tumor |
| Tracers | Tc-99m sulfur colloid + blue dye (combined preferred) |
| Preop imaging | Lymphoscintigraphy |
| Main uses | Breast cancer, melanoma, MCC, H&N, gynecological |
| IHC markers | Cytokeratin (breast), S-100/HMB-45 (melanoma) |
| Identification rate | >95% (combined technique) |
| False-negative rate | 0-11% |
| Key advantage | Avoids full LND morbidity when SLN is negative |
Sources: Schwartz's Principles of Surgery (11th Ed.), Sabiston Textbook of Surgery, Fitzpatrick's Dermatology (Vol. 1-2), Bailey & Love's Short Practice of Surgery (28th Ed.), Berek & Novak's Gynecology.
This is a shared conversation. Sign in to Orris to start your own chat.