Hypersensitivity reactions define, pathogenesis classify, type 1,2,3,4 5 hypersensitivity reactions explain pathogenesis characteristics examples in details with diagram refer robbins 2 mbbs pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the content I need from Robbins for a comprehensive answer. Let me compile the full detailed response.
Hypersensitivity Reactions - Complete Notes (Robbins Pathology)
Source: Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
DEFINITION
Hypersensitivity refers to injurious, excessive, or inappropriate immune reactions that damage the host's own tissues. The term originates from the concept that a previously exposed ("sensitized") individual mounts a pathologically exaggerated response upon re-exposure to the same antigen. These reactions use the same effector mechanisms as protective immunity - antibodies, T lymphocytes, complement, and phagocytes - but the response is poorly controlled, misdirected, or excessive.
"Immune responses that normally are protective are also capable of causing tissue injury. Injurious immune reactions are grouped under hypersensitivity." - Robbins Basic Pathology
CAUSES OF HYPERSENSITIVITY
Hypersensitivity can be directed against:
- Self antigens (Autoimmunity) - failure of self-tolerance; e.g., SLE, rheumatoid arthritis
- Microbial antigens - excessive/persistent responses to microbes; e.g., post-streptococcal glomerulonephritis, TB granulomas
- Environmental antigens (Allergy) - reactions to pollens, dust mites, animal dander, drugs; ~20% of the population in high-income countries
Once a hypersensitivity reaction starts, it is difficult to control because the immune system has intrinsic positive feedback loops. These diseases therefore tend to be chronic and debilitating.
CLASSIFICATION OF HYPERSENSITIVITY REACTIONS
Hypersensitivity reactions are classified into 4 types (Gell and Coombs classification), with a fifth type sometimes added:
| Type | Name | Mechanism | Antibody | Time to Onset |
|---|---|---|---|---|
| I | Immediate / Anaphylactic | IgE + Mast cells | IgE | Minutes |
| II | Antibody-mediated (Cytotoxic) | IgG/IgM vs cell surface antigens | IgG, IgM | Minutes to hours |
| III | Immune complex-mediated | Ag-Ab complex deposition | IgG, IgM | Hours (6-12 h) |
| IV | Cell-mediated (Delayed-type) | T lymphocytes | None (T cell) | 24-72 hours |
| V | Stimulatory (some add) | Antibody stimulates receptor | IgG | Variable |
TYPE I HYPERSENSITIVITY (IMMEDIATE / ANAPHYLACTIC)
Definition
A rapid immunologic reaction occurring in a previously sensitized individual, triggered by the binding of antigen to IgE antibody on the surface of mast cells. Also called allergy or atopy.
Pathogenesis - Sequence of Events
PHASE 1: SENSITIZATION (First exposure)
- Allergen enters the body and is processed by dendritic cells
- Dendritic cells present antigen to naive CD4+ T cells in lymph nodes
- Epithelial cells release IL-25, IL-33, and TSLP in response to allergen injury
- These cytokines drive naive T cells to differentiate into Th2 cells
- Th2 cells secrete IL-4, IL-5, and IL-13:
- IL-4 + IL-13 → stimulate B cells to undergo class switching to IgE
- IL-5 → activates eosinophils
- IL-13 → stimulates mucus secretion from epithelium
- IgE antibodies are produced and bind to high-affinity FcεRI receptors on mast cells and basophils → Sensitized mast cells
PHASE 2: ACTIVATION (Re-exposure)
- On re-exposure, allergen cross-links adjacent IgE molecules on mast cell surface
- Cross-linking of IgE-FcεRI triggers intracellular signal transduction
- Results in mast cell activation and release of mediators
Mediators Released by Mast Cells
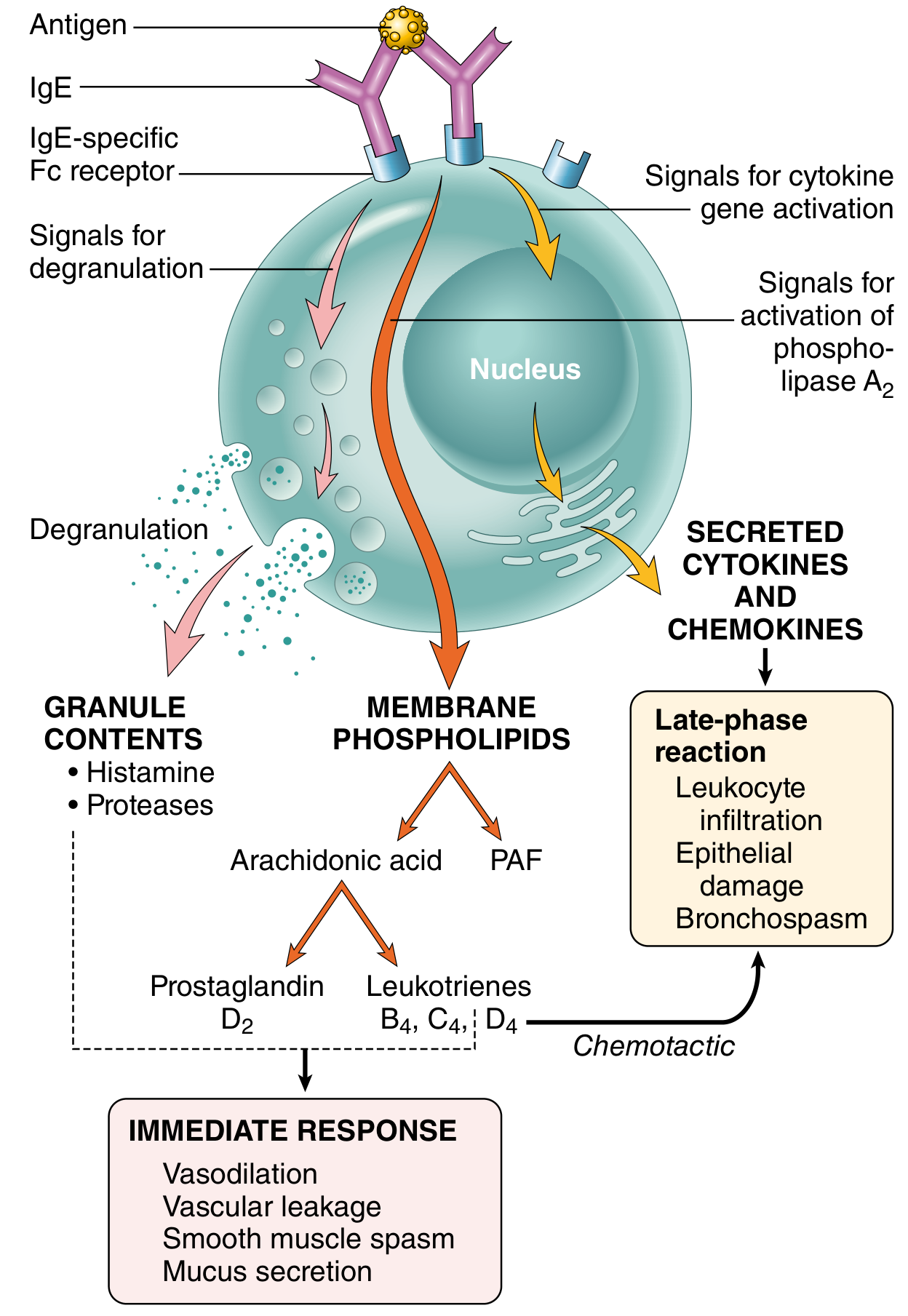
A. Preformed (Granule) Mediators - Released within MINUTES:
- Histamine - most important; causes smooth muscle contraction, increases vascular permeability, stimulates mucus secretion
- Enzymes (tryptase, chymase, acid hydrolases) - cause tissue damage; generate kinins and C3a
- Proteoglycans (heparin, chondroitin sulfate) - package and store amines in granules
B. Lipid Mediators - Synthesized within minutes to hours:
- Prostaglandin D2 - intense bronchoconstriction, vasodilation
- Leukotrienes C4, D4, E4 - most potent bronchoconstricting agents known; increase vascular permeability
- Leukotriene B4 - chemotactic for neutrophils, eosinophils, monocytes
- Platelet-activating factor (PAF) - platelet aggregation, bronchoconstriction, vasodilation
C. Cytokines - Drive the late-phase reaction:
- TNF, IL-1, IL-4, IL-5, IL-13 → leukocyte recruitment
- Chemokines (eotaxin) → recruit eosinophils
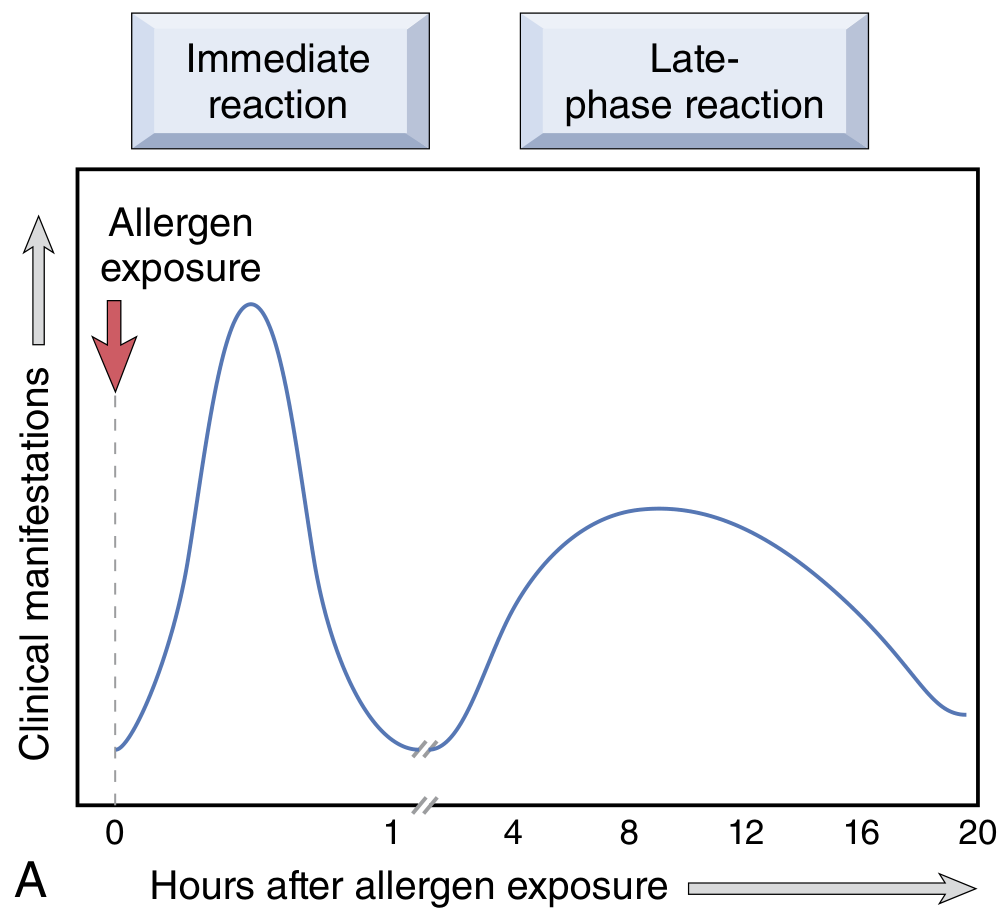
Two Phases of Type I Reaction
| Phase | Timing | Features |
|---|---|---|
| Immediate | Within minutes | Vasodilation, vascular leakage, smooth muscle spasm, mucus secretion |
| Late-phase | 2-24 hours later | Eosinophils, neutrophils, basophils, CD4+ T cells; mucosal epithelial damage; tissue destruction |
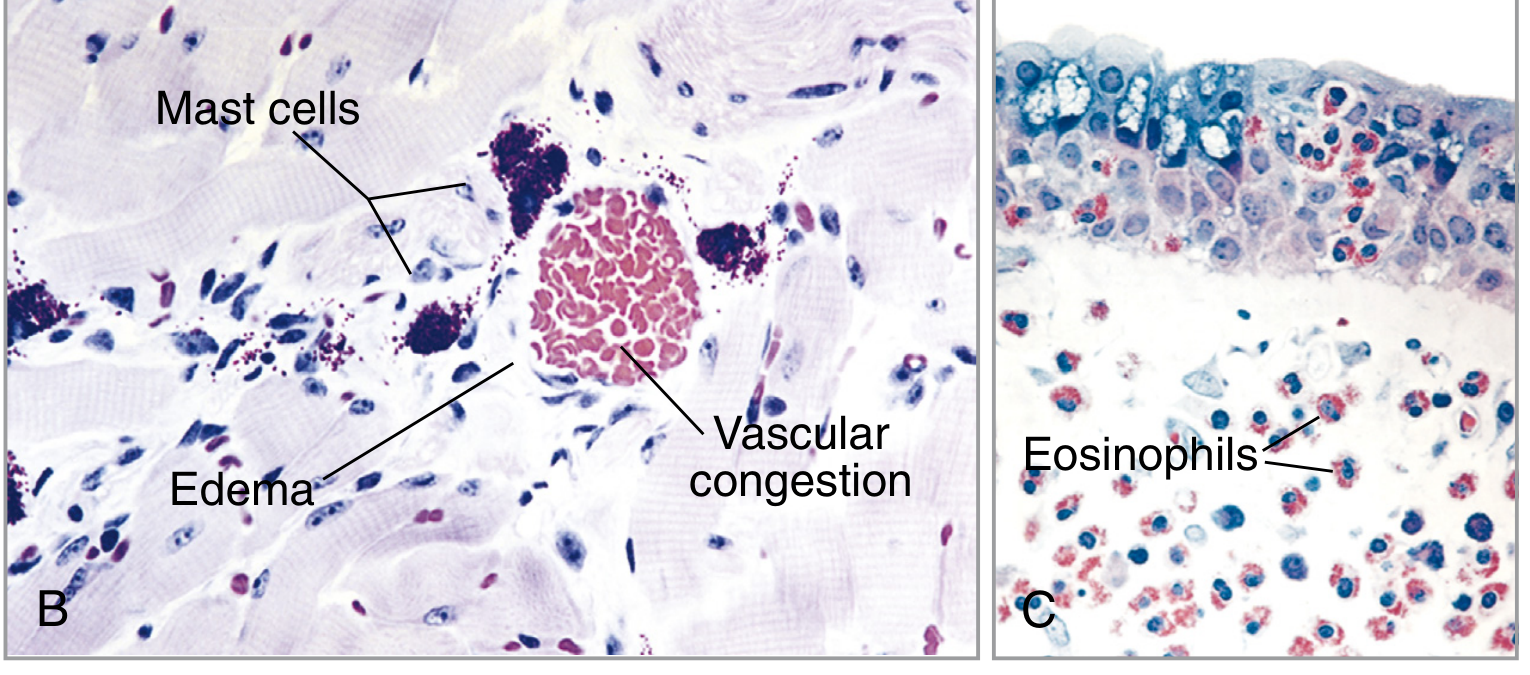
Characteristics
- Antibody: IgE
- Cells: Mast cells, basophils, eosinophils, Th2 cells
- Complement: NOT involved
- Genetic predisposition: Atopy (susceptibility to mount Th2/IgE responses)
- Transfer: Passive transfer with serum (Prausnitz-Küstner reaction)
Clinical Examples
| Local Reactions | Systemic Reaction |
|---|---|
| Allergic rhinitis (hay fever) | Anaphylaxis (bee sting, penicillin) - potentially fatal |
| Bronchial asthma (atopic) | |
| Urticaria (hives), eczema | |
| Food allergy (peanut, milk) | |
| Allergic conjunctivitis |
TYPE II HYPERSENSITIVITY (ANTIBODY-MEDIATED / CYTOTOXIC)
Definition
Disease caused by antibodies (usually IgG, rarely IgM) that react with antigens present on cell surfaces or in the extracellular matrix, destroying cells or triggering inflammation.
Pathogenesis - Three Mechanisms
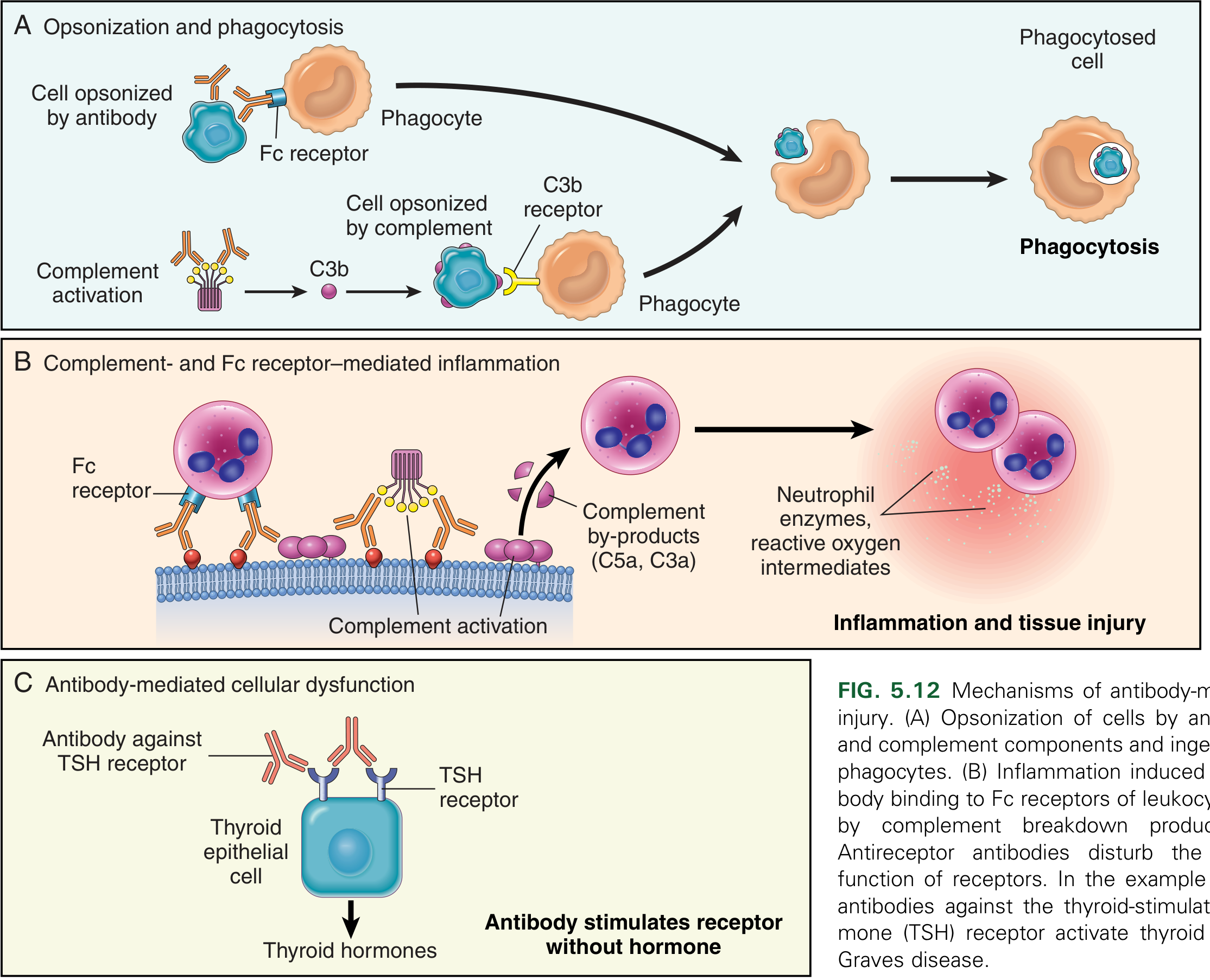
Mechanism A: Opsonization and Phagocytosis
- IgG or IgM antibodies coat (opsonize) cell surface antigens
- Phagocytes recognize IgG via Fc receptors
- Complement is activated (classical pathway) → generates C3b → recognized by C3b receptors on macrophages/neutrophils
- Result: phagocytosis and destruction of the opsonized cell
- Complement activation also forms Membrane Attack Complex (MAC) → osmotic lysis
Mechanism B: Complement- and Fc Receptor-Mediated Inflammation
- Antibody deposits on tissues (not cells) → activates complement → generates C5a, C3a (anaphylatoxins) + C5a (neutrophil chemotaxis)
- Complement fragments and Fc receptors recruit and activate neutrophils and macrophages
- Neutrophils release lysosomal enzymes and reactive oxygen species → tissue damage and fibrinoid necrosis
Mechanism C: Antibody-Mediated Cellular Dysfunction (without tissue injury)
- Antibodies against cell surface receptors impair or dysregulate function
- No complement, no inflammation - purely functional disorder
- Example: In Graves disease, anti-TSH receptor antibodies stimulate the receptor → hyperthyroidism
- Example: In Myasthenia gravis, anti-ACh receptor antibodies block receptor → muscle weakness
Also: ADCC (Antibody-Dependent Cell-Mediated Cytotoxicity)
- Cells coated with IgG are killed by NK cells and macrophages binding via Fc receptors
- No phagocytosis required
Characteristics
- Antibody: IgG (mainly), IgM
- Complement: Classical pathway activated
- Time: Minutes to hours
- Cells: Neutrophils, macrophages, NK cells
- Complement: YES (classical)
Clinical Examples
| Disease | Target Antigen | Mechanism |
|---|---|---|
| Autoimmune hemolytic anemia | RBC membrane proteins (Rh antigens) | Opsonization + phagocytosis |
| Autoimmune thrombocytopenic purpura | Platelet GpIIb/IIIa | Opsonization + phagocytosis |
| Erythroblastosis fetalis (HDN) | Rh antigen on fetal RBCs | Maternal IgG crosses placenta |
| Transfusion reactions | ABO/Rh antigens | Complement-mediated lysis |
| Goodpasture syndrome | Type IV collagen in GBM and alveoli | Complement + Fc receptor inflammation |
| Acute rheumatic fever | Cross-reactive streptococcal antigens | Complement + macrophage activation |
| Myasthenia gravis | Acetylcholine receptor | Receptor blockade (Type II - dysfunction) |
| Graves disease | TSH receptor | Receptor stimulation (Type V if classified separately) |
| Pemphigus vulgaris | Desmogleins (skin junctions) | Protease activation, acantholysis |
| Pernicious anemia | Intrinsic factor | Neutralization |
TYPE III HYPERSENSITIVITY (IMMUNE COMPLEX-MEDIATED)
Definition
Disease caused by antigen-antibody (immune) complexes that form in the circulation or in situ in tissues, deposit in vessel walls and tissues, and trigger complement activation and acute inflammation.
Pathogenesis - Three Phases
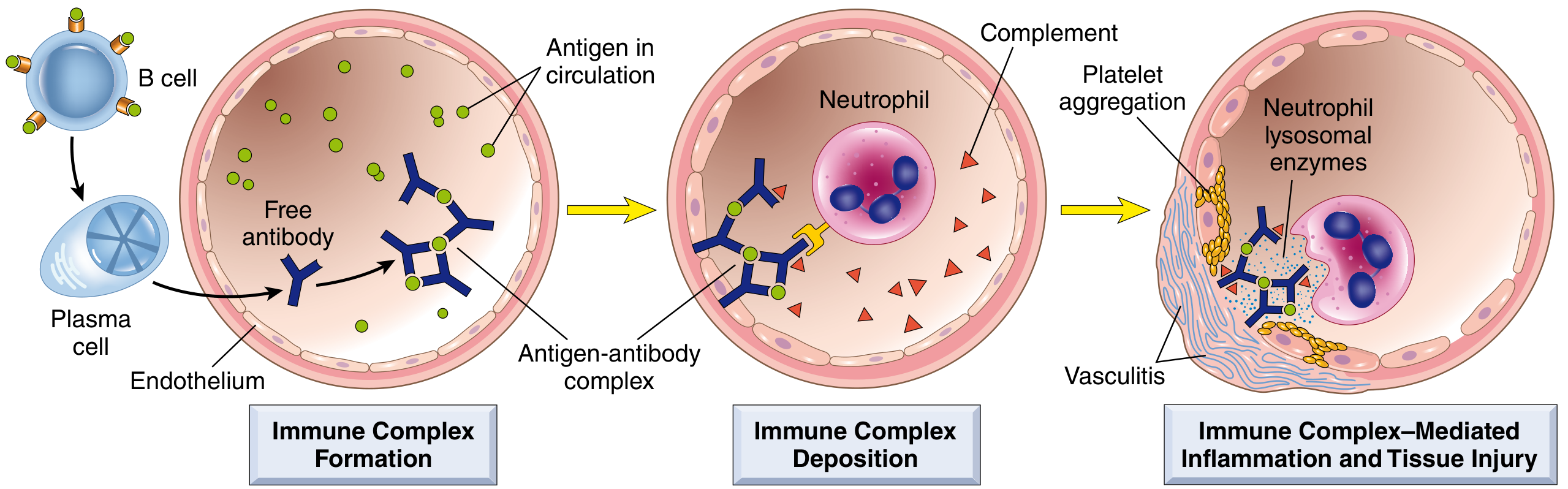
Phase 1: Immune Complex Formation
- Protein antigen enters body → immune response → antibodies produced (IgG/IgM) ~1 week later
- Antibodies react with antigen still in circulation → form antigen-antibody complexes
- Most pathogenic: complexes of intermediate size formed under slight antigen excess (not too large to be cleared, not too small to deposit)
Phase 2: Immune Complex Deposition
- Complexes circulate in blood and deposit in tissues
- Preferential sites: kidney (glomeruli), joints (synovium), skin, small blood vessels
- Why these sites? Organs where blood is filtered at high pressure (urine, synovial fluid) → complexes concentrate; also fenestrated endothelium promotes passage
- Large complexes → cleared efficiently by phagocytes in spleen/liver
- Small complexes → remain in circulation, do not deposit well
- Intermediate-sized complexes → deposit in vessel walls and cause disease
Phase 3: Inflammation and Tissue Injury
- Deposited complexes activate complement (classical pathway) → C3a, C5a (anaphylatoxins)
- C5a is chemotactic → recruits neutrophils and monocytes
- Neutrophils attempt to phagocytose complexes → frustrated phagocytosis → release lysosomal enzymes and ROS → tissue damage
- Complement consumption → ↓ serum C3 levels (useful disease marker)
- Platelet aggregation → microthrombi formation → ischemia
Morphology
Principal lesion: Acute vasculitis with fibrinoid necrosis - a smudgy eosinophilic area of tissue destruction. On immunofluorescence: granular deposits of immunoglobulin and complement. On EM: electron-dense deposits along glomerular basement membrane.
Types
- Systemic immune complex disease (Serum sickness): single large antigen exposure → complexes form → deposit systemically → fever, urticaria, joint pain, proteinuria at ~10 days
- Local immune complex disease (Arthus reaction): intracutaneous antigen injection in immunized individual with circulating antibodies → large complexes form locally → fibrinoid necrosis of vessel wall + thrombosis
Characteristics
- Antibody: IgG (primarily), IgM
- Complement: YES (classical pathway) - C3 levels fall
- Key feature: Granular (lumpy-bumpy) immunofluorescence (vs. linear in Goodpasture)
- Time: 6-12 hours (or ~10 days for serum sickness)
- Sites: Kidney, joints, skin, blood vessels
Clinical Examples
| Disease | Antigen |
|---|---|
| Systemic lupus erythematosus (SLE) | Nuclear antigens (dsDNA, histones) |
| Post-streptococcal glomerulonephritis | Streptococcal antigens |
| Membranous glomerulonephritis | Hepatitis B antigens, self antigens |
| Serum sickness | Foreign serum proteins, drugs |
| Henoch-Schönlein purpura | IgA complexes |
| Rheumatoid arthritis | IgG Fc (rheumatoid factor) |
| Polyarteritis nodosa | Hepatitis B surface antigen |
| Arthus reaction (local) | Subcutaneous antigen + Ab |
TYPE IV HYPERSENSITIVITY (CELL-MEDIATED / DELAYED-TYPE)
Definition
Tissue injury caused by T lymphocytes - specifically CD4+ Th1 and Th17 cells (causing cytokine-mediated inflammation) and CD8+ cytotoxic T lymphocytes (CTLs). No antibody is involved. Called "delayed" because it peaks 24-72 hours after antigen challenge (unlike immediate type I).
Pathogenesis - Two Mechanisms
Mechanism A: CD4+ T Cell-Mediated (Delayed-Type Hypersensitivity - DTH)
Step 1: Sensitization (First exposure)
- APC (dendritic cell) presents antigen via MHC class II to naive CD4+ T cells
- If APC produces IL-12 → T cells differentiate into Th1 cells
- If APC produces IL-1, IL-6, IL-23 → T cells differentiate into Th17 cells
- These effector T cells enter circulation as memory cells
Step 2: Elicitation (Re-exposure, 24-72 hours)
- Re-exposure to antigen → Th1 cells release IFN-γ (key cytokine)
- IFN-γ activates macrophages ("classical activation") → macrophages:
- Enhanced phagocytosis and killing ability
- Express more MHC class II → amplify antigen presentation
- Secrete TNF, IL-1, chemokines → promote inflammation
- Produce more IL-12 → amplify Th1 response (positive feedback loop)
- Th17 cells secrete IL-17, IL-22 → recruit neutrophils and monocytes
- Result: Perivascular mononuclear infiltrate (lymphocytes + macrophages)
Step 3: Chronic persistence
- With persistent or nondegradable antigens (e.g., M. tuberculosis), macrophages transform into epithelioid cells → aggregate into granulomas surrounded by lymphocytes
- This is granulomatous inflammation, driven by Th1 + IFN-γ
Mechanism B: CD8+ CTL-Mediated Cytotoxicity
- CD8+ CTLs recognize antigen presented via MHC class I on target cells
- Kill target cells directly by perforin-granzyme pathway
- Also secrete IFN-γ
- Important in: viral infections, graft rejection, type 1 diabetes (destruction of islet cells)
Histology of DTH Reaction
Classic Test: Tuberculin (Mantoux) Reaction
- Intracutaneous injection of PPD (purified protein derivative of M. tuberculosis)
- In previously sensitized individual: redness and induration appear at 8-12 hours, peak at 24-72 hours
- Morphology: accumulation of CD4+ T cells and macrophages around venules ("perivascular cuffing"), marked endothelial hypertrophy
Characteristics
- No antibody involved (purely cellular)
- Key cells: CD4+ Th1 and Th17 cells, CD8+ CTLs, macrophages
- Key cytokines: IFN-γ (most important), IL-17, TNF, IL-12
- Time: 24-72 hours (hence "delayed")
- Complement: NOT involved
- Cannot be transferred with serum (only with T cells)
Clinical Examples
| Disease | Antigen | Principal Mechanism |
|---|---|---|
| Contact dermatitis (poison ivy, nickel) | Urushiol, haptens | Th1/Th17 cytokines → epidermal necrosis |
| Tuberculin skin test (PPD) | Mycobacterial proteins | Classic DTH |
| Tuberculosis granuloma | M. tuberculosis | Granulomatous inflammation (Th1) |
| Type 1 diabetes mellitus | Islet β cell antigens | CTL destruction of islet cells |
| Multiple sclerosis | Myelin basic protein | Th1/Th17 → demyelination |
| Rheumatoid arthritis | Collagen, citrullinated proteins | Th17 cytokines → joint destruction |
| Celiac disease | Gluten-derived gliadin | Th1 + CTLs → intestinal damage |
| Graft rejection (chronic) | Alloantigens | CD4+ and CD8+ T cells |
TYPE V HYPERSENSITIVITY (STIMULATORY)
Some classifications add a 5th type where antibodies against cell surface receptors stimulate (rather than block or destroy) the receptor, causing overactivity without tissue destruction.
Characteristics
- Antibody: IgG
- Mechanism: Antibody mimics the natural ligand → constitutive receptor activation
- No complement activation, no cell destruction
- Sometimes classified within Type II (antibody-mediated cellular dysfunction)
Prototypic Example: Graves Disease (Hyperthyroidism)
- Antibodies against TSH receptor on thyroid cells
- Antibody binds and continuously stimulates TSH receptor (acts like TSH)
- → Continuous production of thyroid hormones → hyperthyroidism
- Clinically: weight loss, tachycardia, exophthalmos, goiter
Other Examples
- Myasthenia gravis (traditionally Type II - receptor blockade, but sometimes listed here)
SUMMARY COMPARISON TABLE
| Feature | Type I | Type II | Type III | Type IV | Type V |
|---|---|---|---|---|---|
| Mechanism | IgE → mast cell | IgG/IgM vs cell Ag | IgG/IgM immune complexes | T lymphocytes | IgG stimulates receptor |
| Antibody | IgE | IgG, IgM | IgG, IgM | None | IgG |
| Cells | Mast cells, eosinophils | Neutrophils, macrophages, NK | Neutrophils | CD4+ (Th1/Th17), CD8+ CTL | - |
| Complement | No | Yes (classical) | Yes (classical) | No | No |
| Transfer | Serum (IgE) | Serum | Serum | T cells only | Serum |
| Onset | Minutes (< 30 min) | Minutes-hours | 6-12 hours | 24-72 hours | Variable |
| Key mediators | Histamine, leukotrienes, PGD2 | C3b, MAC, Fc receptors | C3a, C5a, neutrophil enzymes | IFN-γ, IL-17, TNF | Receptor stimulation |
| Key examples | Anaphylaxis, asthma, allergy | AIHA, Goodpasture, MG | SLE, serum sickness, PSGN | TB, contact dermatitis, T1DM | Graves disease |
| Histology | Vasodilation, edema, eosinophils (late) | Phagocytosis, necrosis | Fibrinoid necrosis, vasculitis | Perivascular mononuclear "cuffing", granulomas | Normal/hyperplastic |
KEY MNEMONICS FOR EXAM
- Type I - "IMMEDIATE" ANAPHYLAXIS: IgE, Instant, mast cell Irritation → histamine
- Type II - "CYTOTOXIC": antibodIes kIll Cells (the letter "II" reminds you of two direct targets: complement + Fc receptor)
- Type III - "IMMUNE COMPLEX": Complex disease, III = Triple trouble (form, deposit, inflame)
- Type IV - "DELAYED" (D = Days; DTH): T-cell mediated, no antibody, needs 24-72h
- Type V - "STIMULATORY": antibody mimics Stimulant → receptor overactivation
All content referenced from: Robbins & Kumar Basic Pathology (ISBN 9780323790185) and Robbins, Cotran & Kumar Pathologic Basis of Disease (ISBN 9780443264528), Chapters 5-6, Immunologically Mediated Tissue Injury.
This is a shared conversation. Sign in to Orris to start your own chat.