Hi
Hi there! How can I help you today?
Can u explan me about skin grafting
Reading File
Finding Sources
Searching PubMed
skin grafting techniques outcomes
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Here is a thorough explanation of skin grafting based on authoritative surgical textbooks:
Skin Grafting
What Is a Skin Graft?
A skin graft is a piece of skin surgically removed from one area of the body (the donor site) and transplanted to cover a damaged, missing, or deficient area (the recipient site). Grafts are used for:
-
Burns (especially full-thickness burns)
-
Traumatic wounds
-
Surgical excision defects (e.g., after tumor removal)
-
Chronic non-healing ulcers
-
Areas where primary closure is not possible
-
Sabiston Textbook of Surgery
Types of Skin Grafts
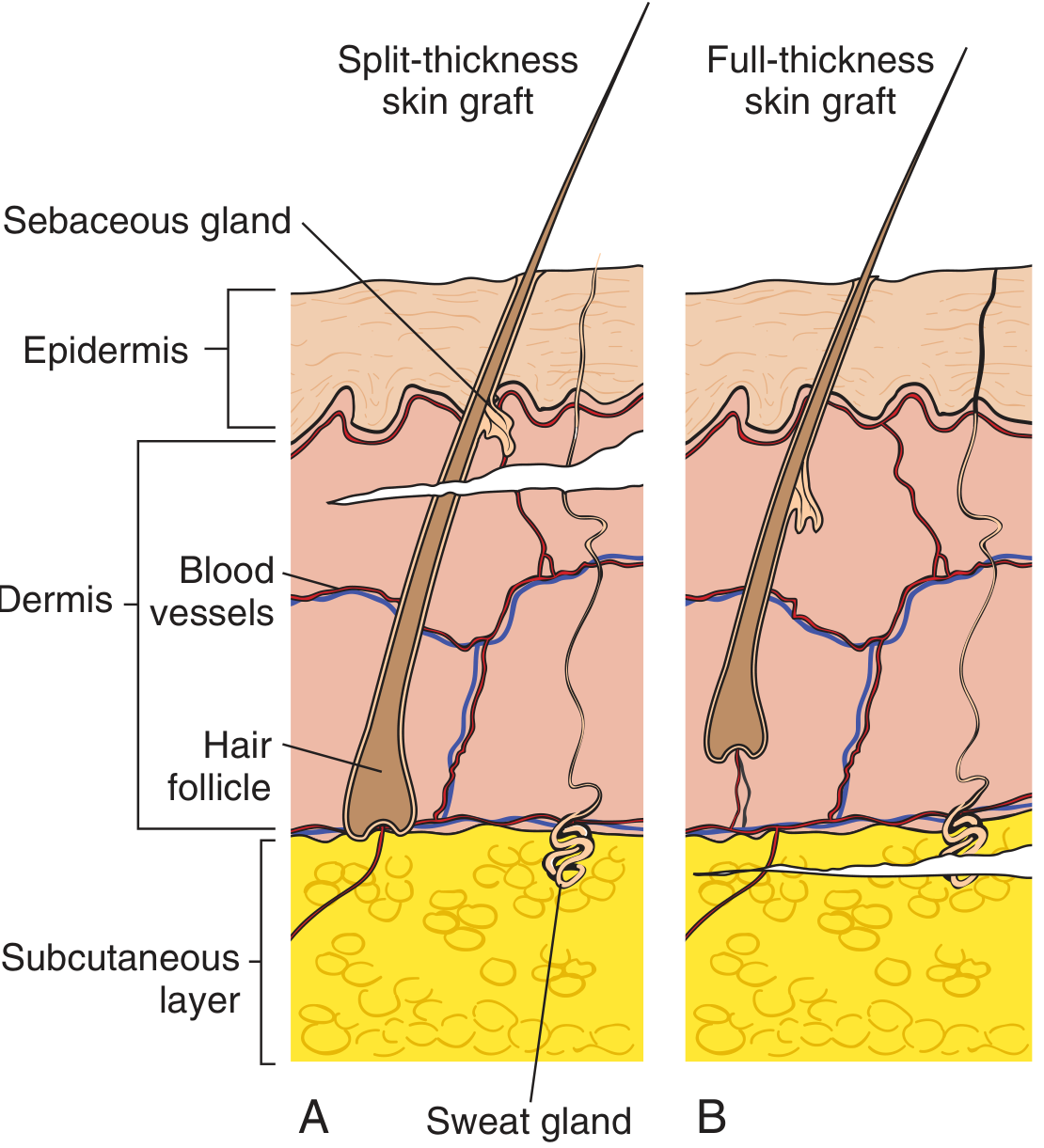
1. Split-Thickness Skin Graft (STSG)
- Contains the epidermis + part of the dermis (leaving behind deeper dermis to regenerate)
- Thickness grades:
- Thin: 0.005 - 0.010 inch
- Medium
- Thick: up to 0.015 inch
- Harvested using an electric or mechanical dermatome (set at 0.014-0.016 inch, angled 45-60 degrees)
- Can be meshed (small slits cut) to cover large areas - expansion ratios of 1:1.5, 1:2, 1:3, even up to 1:6 or 1:9
- Donor site heals on its own since part of the dermis remains
Advantages:
- Can cover large areas when meshed
- Less blood supply needed to survive
- Donor site heals faster
- Good for poor vascular beds
Disadvantages:
- More secondary contraction (scar shrinkage)
- Abnormal pigmentation
- More susceptible to trauma
- Poor sensory recovery
- No hair follicles (hairless graft)
2. Full-Thickness Skin Graft (FTSG)
- Contains epidermis + entire dermis
- Harvested by sharp scalpel dissection
- Donor site must be closed directly (sutured) or itself grafted
- Used for smaller defects in cosmetically important areas (face, nose, temple)
Advantages:
- Less secondary contraction (better cosmetic result)
- Better color and texture match
- More durable, resists trauma
- Better sensory recovery (more neurilemmal sheaths in dermis)
- Contains hair follicles
Disadvantages:
- Requires better vascular bed to survive
- More primary contraction (elastic recoil after harvest)
- Limited by donor site size
3. Composite Grafts
-
Contain two or more tissue types (e.g., skin + cartilage from the ear, or septal mucosa + cartilage)
-
Used for reconstructing composite defects such as the alar rim, ear, or eyelid
-
Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Pfenninger and Fowler's Procedures for Primary Care
Skin Graft Healing ("Take")
Once harvested, a graft is temporarily detached from its blood supply. The process of re-establishing blood flow is called graft take, which occurs in four stages:
| Stage | Timing | Mechanism |
|---|---|---|
| Graft Adherence | Immediate | Fibrin layer forms between graft and recipient bed |
| Serum Imbibition | Up to 48 hours | Graft survives by absorbing nutrients from plasma leaking from recipient capillaries; graft swells and gains weight |
| Revascularization | 48 hrs - 3 weeks | 1) Inosculation: cut vessel ends join up; 2) Revascularization: ingrowth of new vessels; 3) Neovascularization: vessels grow down basement membrane |
| Remodelling | 3 weeks - 1 year | Collagen reorganization and graft maturation |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Requirements for Successful Graft Take
For the graft to survive, close contact between the graft and the recipient bed is essential. This is ensured by:
- Wound bolsters
- Negative-pressure dressings (VAC therapy)
- Fixation with staples, surgical glue (thrombin or cyanoacrylate), or sutures
Conditions that impair graft survival:
- Exposed bone, irradiated tissue, cartilage, or tendon (limited vascularity)
- Hematoma or seroma under the graft (breaks contact)
- Infection
- Movement at the graft site
Systemic factors that reduce take:
- Diabetes mellitus
- Smoking
- Previous radiotherapy or chemotherapy
- Poor nutritional status
Graft Application Technique (STSG)
- Measure the defect and mark the donor site (often inner upper thigh or scalp)
- Harvest with a dermatome at 0.014-0.016 inch thickness
- Mesh the graft if needed to cover larger areas
- Apply with dermis side down on the wound bed
- Fix with staples or sutures; use low-adherent dressings (e.g., adaptic)
- Donor site is dressed separately
- Fischer's Mastery of Surgery, 8th ed.
STSG vs. FTSG - Quick Comparison
| Factor | STSG | FTSG |
|---|---|---|
| Dermis included | Partial | All |
| Donor site healing | Heals on own | Must be sutured |
| Vascularity required | Less | More |
| Primary contraction | Less | More |
| Secondary contraction | More | Less |
| Cosmesis | Poorer | Better |
| Hair growth | None | Present |
| Best use | Large areas, burns | Small cosmetic areas (face) |
Summary
Skin grafting is one of the most versatile reconstructive techniques in surgery. STSGs are preferred for large wounds and burns, while FTSGs are reserved for smaller, cosmetically sensitive areas. The key to success is achieving close graft-to-bed contact, adequate vascularity, and immobilization during the critical first 48-72 hours of revascularization.
This is a shared conversation. Sign in to Orris to start your own chat.