Fatty liver
Reading File
Finding Sources
Searching PubMed
"nonalcoholic fatty liver disease" OR "metabolic associated fatty liver"
Searching the Web
fatty liver disease MASLD NAFLD 2025 guidelines pathophysiology treatment
Reading File
Reading File
Loading Image
Reading File
I now have rich content from two authoritative textbooks plus current guidelines and PubMed data. Let me compile a comprehensive answer.
Fatty Liver Disease (MASLD/NAFLD)
What Is It?
Fatty liver disease refers to the accumulation of fat (predominantly triglycerides as macrovesicular steatosis) in hepatocytes, affecting ≥5% of liver cells, in the absence of significant alcohol use. The condition now carries updated nomenclature:
- NAFLD (Nonalcoholic Fatty Liver Disease) - older term, still widely used
- MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease) - the current preferred term adopted in 2023, emphasizing the metabolic driver
- MASH (Metabolic Dysfunction-Associated Steatohepatitis) - replaces NASH
Global prevalence is approximately 25%, making it the most common chronic liver disease worldwide.
Spectrum of Disease
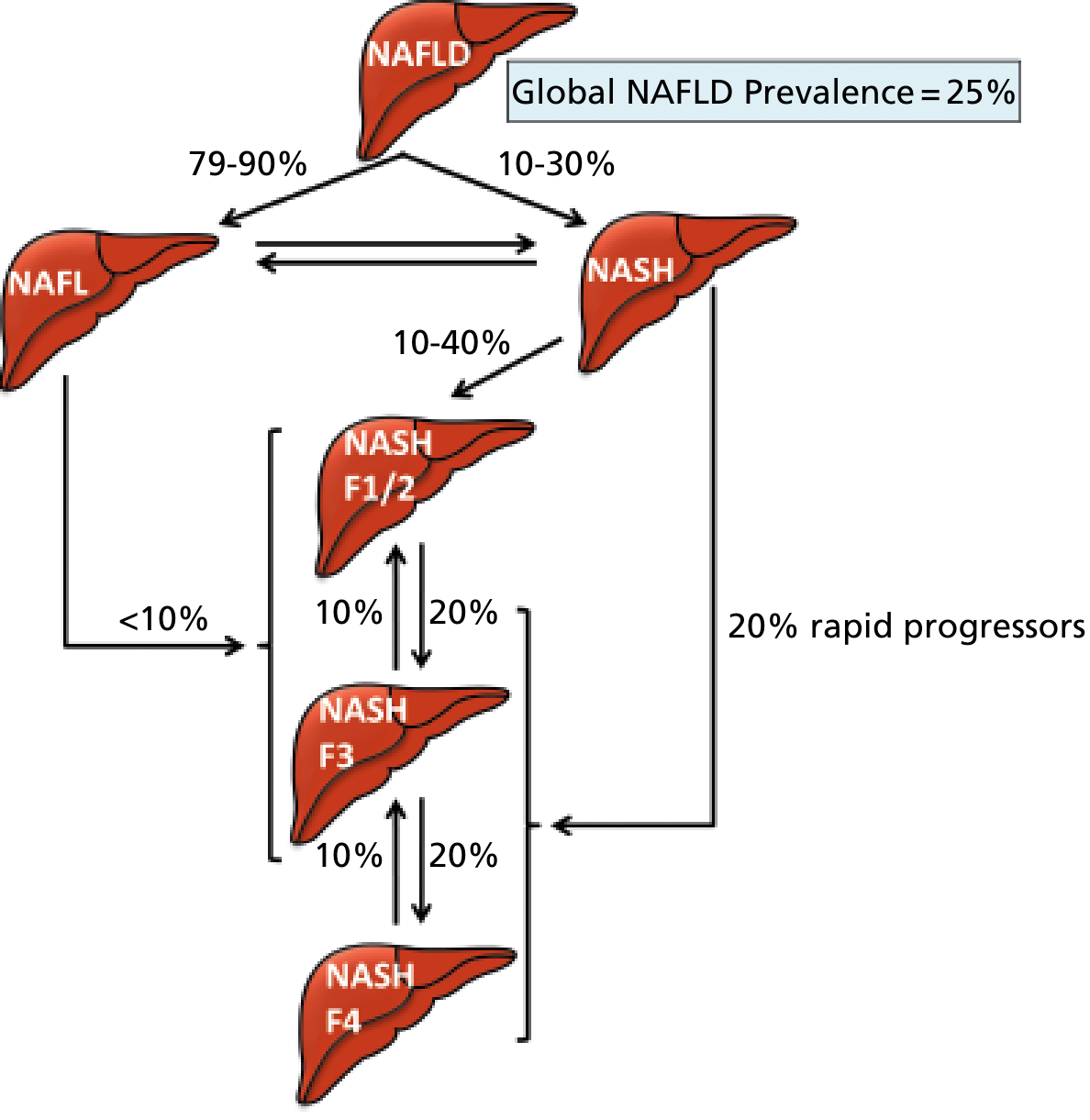
The disease spans a continuum:
| Stage | Features | Notes |
|---|---|---|
| NAFL / Simple Steatosis | Fat deposition, no significant inflammation | 79-90% of NAFLD; bidirectional with NASH |
| NASH / MASH | Steatosis + hepatocyte ballooning + inflammation ± fibrosis | 10-30% of NAFLD; liver-related mortality rises |
| Fibrosis (F1-F4) | Progressive scarring (F1 perisinusoidal → F4 cirrhosis) | Fibrosis stage is the #1 predictor of outcomes |
| Cirrhosis | End-stage scarring, portal hypertension | Risk of HCC even without cirrhosis in NAFLD |
- Progression is non-linear - some patients cycle between NAFL and NASH
- ~20% of NASH patients are rapid progressors to advanced fibrosis
- Fibrosis regression is possible with treatment
Risk Factors / Associated Conditions
- Obesity (especially central/visceral adiposity)
- Type 2 diabetes mellitus or insulin resistance
- Dyslipidemia (hypertriglyceridemia, low HDL, high LDL)
- Hypertension
- Metabolic syndrome (all of the above)
MASLD diagnosis requires hepatic steatosis plus at least one cardiometabolic risk factor (per current 2023 criteria).
Pathogenesis
The "multiple-hit" model has replaced the older "two-hit" model:
-
Insulin resistance - the central driver. It increases adipose tissue lipolysis, flooding the liver with free fatty acids (FFAs). Reduced adiponectin further impairs FFA oxidation in skeletal muscle and increases hepatocyte FFA uptake.
-
Hepatic lipotoxicity - accumulated lipids (especially saturated FFAs like palmitate and lysophosphatidylcholine) directly injure hepatocytes via:
- Endoplasmic reticulum (ER) stress
- Mitochondrial dysfunction
- Lysosomal dysfunction
- Reactive oxygen species (ROS) production
- Inflammasome activation → IL-1 release
-
Hepatocyte ballooning - ballooned hepatocytes produce sonic hedgehog, which activates hepatic stellate cells (HSCs) in a paracrine fashion → collagen deposition → fibrosis
-
Innate immune activation - gut-derived endotoxins (via dysbiosis and increased gut permeability) activate Kupffer cells and inflammatory signaling
-
Genetic factors - the PNPLA3 rs738409 variant (C>G polymorphism) is the strongest genetic risk factor for both disease severity and HCC risk
-
Gut microbiome dysbiosis - independently contributes to inflammation and bile acid signaling changes
Clinical Features
- Most patients are asymptomatic - often an incidental finding
- Symptoms, when present: fatigue, malaise, right upper quadrant discomfort
- Labs: elevated ALT and AST, with AST:ALT ratio typically <1 (key differentiator from alcoholic liver disease, where AST:ALT >2)
- Hepatomegaly may be present on examination
- Advanced disease shows signs of chronic liver disease/cirrhosis
Diagnosis
Non-invasive methods (first line):
- Ultrasound - most common screening tool; detects steatosis >20-33% of hepatocytes
- FIB-4 score (using age, AST, ALT, platelets) - initial fibrosis risk stratification
- Transient elastography (FibroScan) with CAP (controlled attenuation parameter)
- MRI-PDFF (proton density fat fraction) - most accurate quantification of steatosis
- MR elastography - most accurate non-invasive fibrosis assessment
Liver biopsy - still the gold standard for:
- Diagnosing NASH/MASH (distinguishing from simple steatosis)
- Staging fibrosis accurately
- Graded by the NAFLD Activity Score (NAS): steatosis (0-3) + lobular inflammation (0-3) + ballooning (0-2); NAS ≥5 = NASH
Complications / Outcomes
Top causes of mortality in NAFLD patients (in order):
- Cardiovascular disease (most common overall cause of death)
- Cirrhosis
- Non-liver malignancy
- Hepatocellular carcinoma (HCC)
- Diabetes mellitus
Key points:
- In NASH specifically, liver-related mortality surpasses cardiovascular mortality
- NAFLD-related HCC is growing 9% annually in the US
- NAFLD is a major contributor to "cryptogenic" cirrhosis
- Shares risk factors with coronary artery disease
Treatment
Lifestyle (cornerstone)
- ≥5% body weight loss - improves steatosis, ballooning, and inflammation
- ≥7-10% weight loss - improves fibrosis; 10%+ achieves greatest fibrosis resolution
- Mediterranean-style diet (reduced refined carbs, saturated fat)
- Aerobic exercise (even without weight loss, reduces hepatic fat)
- Avoid sugar-sweetened beverages and fructose
Bariatric/Metabolic Surgery
- Proven to improve NASH histology and induce fibrosis regression
- Considered in obese patients with BMI ≥35 with metabolic comorbidities
Pharmacological
Approved agents (as of 2024-2025):
- Resmetirom (Rezdiffra) - thyroid hormone receptor-beta (THR-β) agonist; first-ever FDA-approved drug specifically for MASH with fibrosis (approved March 2024)
- Semaglutide (Ozempic/Wegovy) - GLP-1 receptor agonist; AASLD updated guidance in November 2025 supports use for MASH; meta-analysis confirms efficacy (PMID 40489581)
Used off-label / under investigation:
- SGLT2 inhibitors (empagliflozin, dapagliflozin)
- Pioglitazone (in patients with T2DM, improves steatohepatitis)
- Vitamin E (in non-diabetic adults with NASH)
- FGF19/FGF21 analogs, PPAR agonists (phase 3 trials)
Cardiovascular Risk Management
- Statins are safe in NAFLD and should be used for dyslipidemia management
- Control of hypertension, diabetes, and hyperlipidemia is integral to care
Pediatric NAFLD
- Growing problem paralleling pediatric obesity epidemic
- Distinct histology: inflammation and scarring are more prominent in portal tracts/periportal regions (vs. centrilobular in adults), with mononuclear (not neutrophilic) infiltrates predominating
Key Differentials
- Alcoholic fatty liver - AST:ALT >2, history of alcohol use, GGT often elevated
- Drug-induced steatosis - amiodarone, methotrexate, tamoxifen, valproate, corticosteroids
- Acute fatty liver of pregnancy (AFLP) - obstetric emergency
- Lipodystrophy, hypothyroidism, celiac disease
Sources:
- Robbins & Kumar Basic Pathology, 10th ed.
- Yamada's Textbook of Gastroenterology, 7th ed.
- AASLD Practice Guidance on MASLD (updated 2023-2025), aasld.org
- GLP-1 therapies for MASH meta-analysis (Wang et al., 2025) - PMID 40489581
- Global epidemiology in T2DM meta-analysis (Younossi et al., 2024) - PMID 38521116
Cervical radiculopathy
Reading File
Finding Sources
Searching PubMed
"cervical radiculopathy" AND treatment
Searching the Web
cervical radiculopathy diagnosis management guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Bradley and Daroff's Neurology textbook, plus imaging, PubMed data, and recent guidelines. Here is the full answer:
Cervical Radiculopathy
Definition
Cervical radiculopathy is a clinical syndrome caused by compression or irritation of a cervical nerve root, producing pain, sensory disturbance, motor weakness, and/or reflex changes in a dermatomal/myotomal distribution corresponding to the affected root. It is one of the most common causes of neck and arm pain.
Etiology and Pathophysiology
Two main mechanisms account for the vast majority of cases:
1. Disc Herniation (younger patients, <45 years)
- Nucleus pulposus extrudes through the annulus fibrosus and compresses the adjacent nerve root
- More likely to present acutely
- Biochemical irritation from inflammatory mediators (phospholipase A2, cytokines) also contributes - not purely mechanical compression
2. Foraminal Stenosis from Degenerative Changes (older patients, >45 years)
- Uncovertebral joint osteophytes (posterolateral) and facet joint osteophytes narrow the intervertebral foramen
- Cervical spondylosis - degenerative disc disease with disc height loss, osteophyte formation, ligamentum flavum hypertrophy
- Becomes more prevalent with increasing age; the more common cause overall
Levels most often affected: C5-C6 (C6 root) and C6-C7 (C7 root) - these are the levels of greatest cervical mobility where disc degeneration is greatest. C4-C5 (C5 root) is the next most common.
Nerve Root Level Localization
This table is the clinical core of cervical radiculopathy:
| Root | Disc Level | Pain / Sensory Area | Weakness | Reflex Lost |
|---|---|---|---|---|
| C5 | C4-C5 | Shoulder, lateral arm | Deltoid, biceps, brachioradialis | Biceps, supinator |
| C6 | C5-C6 | Lateral forearm, thumb & index finger | Brachioradialis, wrist extensors | Biceps, brachioradialis |
| C7 | C6-C7 | Index, middle, ± ring finger; subscapular | Triceps, wrist flexors, pronators | Triceps |
| C8 | C7-T1 | Ring & little finger, medial forearm | Hand intrinsics, finger flexors | None reliable |
| T1 | T1-T2 | Medial arm/elbow | Hand intrinsics | None reliable |
Key pearls:
- C8/T1 clinically evident compression is less common
- Subscapular/interscapular pain is characteristic of lower cervical roots (C7 especially, also C6, C8, T1)
- Radicular pain is worsened by Valsalva/coughing (increased intradiscal pressure)
Clinical Presentation
Symptoms often appear suddenly, though most lack an identifiable traumatic trigger. The classic presentation is:
- Neck pain radiating down the arm in a dermatomal pattern
- Paresthesias, dysesthesias, numbness in the corresponding dermatome
- Weakness of muscles innervated by the affected root (myotome)
- Reflex diminution or loss (lower motor neuron at the level of the lesion)
Important: The absence of objective neurologic deficits does not exclude radiculopathy - isolated root demyelination without axonal loss can cause full radicular symptoms with a normal EMG.
Physical Examination
Key Provocative Tests
Spurling's Test (Spurling Maneuver)
- Neck extension + lateral rotation toward the symptomatic side + downward axial compression
- Reproduces or worsens radicular arm pain
- A 2025 systematic review and meta-analysis (PMID 39938056) confirms good specificity for subacute/chronic cervical radiculopathy; best used to confirm, not exclude
Shoulder Abduction Relief Sign
- Placing the hand on top of the head relieves radicular pain (reduces nerve root tension)
- Highly specific for cervical radiculopathy
Neck Distraction Test
- Manual axial traction of the head by the examiner relieves arm pain
- Positive when it reduces radicular symptoms
Upper Limb Tension Test (ULTT)
- Neurodynamic test analogous to the straight-leg raise for lumbar radiculopathy
- A 2025 meta-analysis (PMID 40156954) evaluated diagnostic accuracy of neurodynamic tests for upper-limb entrapment/radicular pathology
Warning Signs of Myelopathy (not radiculopathy alone)
If any of these are present, suspect concurrent cervical spondylotic myelopathy:
- Spread of biceps reflex to finger flexors (inverted biceps reflex)
- Paradoxical biceps reflex (absent biceps + reflex contraction of finger flexors/triceps)
- Increased triceps reflex with absent biceps reflex
- Hoffman's sign, clonus, Babinski sign
- Gait disturbance, leg spasticity
Diagnostic Testing
Imaging
MRI (preferred first-line imaging)
- Identifies nerve root compression, disc herniation, foraminal stenosis, and spinal cord changes
- Must be interpreted cautiously - degenerative abnormalities are extremely common in the asymptomatic spine
- Indicated when: symptoms persist >4-6 weeks without improvement, progressive neurologic deficit, red flags present, or surgery/injection being considered
CT Myelography (alternative)
- More sensitive than MRI in some cases
- Better at distinguishing osteophyte/calcified disc from soft disc herniation
- Preferred when: MRI contraindicated (pacemaker, spinal cord stimulator), prior hardware from cervical fusion (causes MRI artifact), severe claustrophobia
- Limitation: Cannot visualize lateral disc herniation beyond the subarachnoid space
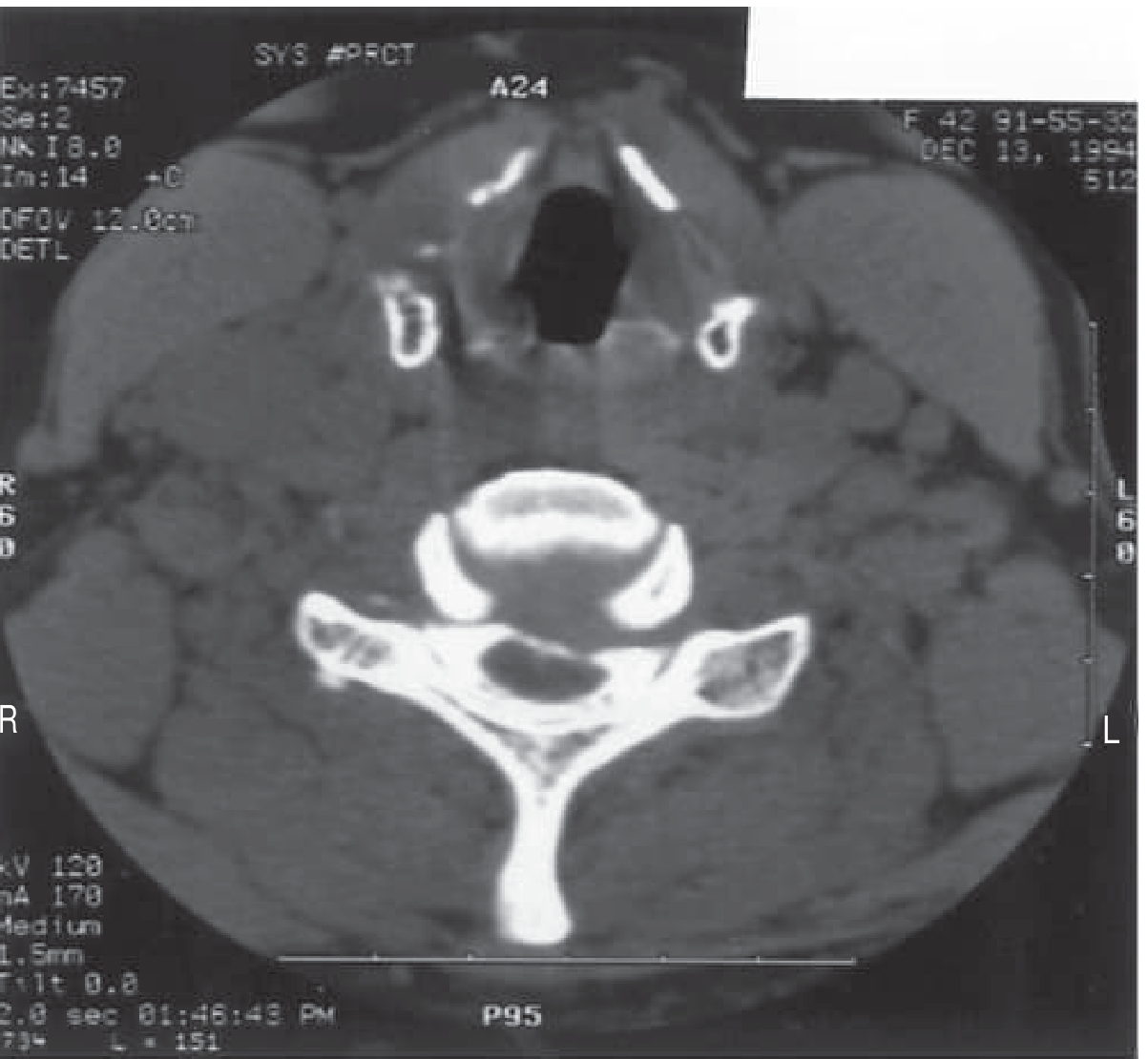
CT with intrathecal contrast showing a herniated cervical disc distorting the spinal cord and thecal sac (Bradley and Daroff's Neurology)
Plain X-rays - of little diagnostic value for radiculopathy, but may be used to screen for instability, fracture, or alignment.
ACR Appropriateness Criteria (2024 update) supports MRI as usually appropriate for suspected cervical radiculopathy, with CT myelography as an alternative when MRI is unavailable or contraindicated.
Electrodiagnostic Studies (EMG/NCS)
Key pattern of cervical radiculopathy on NCS:
- Reduced CMAP amplitude (motor) - affected
- Preserved SNAP amplitude (sensory) - preserved despite sensory symptoms
This apparent paradox occurs because the dorsal root ganglion (DRG) lies outside the spinal canal. Compression is proximal to the DRG, so the peripheral sensory axon remains intact from the DRG distally - hence the SNAP is preserved even with sensory symptoms (preganglionic lesion).
Needle EMG: Moderate sensitivity (50-71%). Must wait 5-6 days after injury for motor fiber changes and 8-9 days for sensory fiber changes (Wallerian degeneration).
Role: Most useful in diagnostically uncertain cases, to distinguish radiculopathy from brachial plexopathy or peripheral neuropathy (e.g., carpal tunnel, cubital tunnel).
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Shoulder pathology (rotator cuff, impingement) | Pain localized to shoulder, normal neck exam, worsened by shoulder movements |
| Brachial neuritis (Parsonage-Turner) | Acute severe shoulder/arm pain, then rapid weakness; no disc pathology; patchy neurologic signs |
| Thoracic outlet syndrome | Vague shoulder pain + numbness of 4th/5th digits; positional |
| Carpal tunnel syndrome | Nocturnal symptoms, thenar wasting, positive Tinel/Phalen at wrist |
| Cubital tunnel syndrome | Ulnar distribution (4th/5th digits), positive Tinel at elbow |
| Cervical myelopathy | Bilateral symptoms, spasticity, hyperreflexia below lesion, gait disorder |
| Pancoast tumor | C8-T1 distribution, Horner's syndrome, constitutional symptoms |
Treatment
Natural History
The prognosis for cervical radiculopathy is generally favorable. Most cases improve significantly over 4-8 weeks regardless of specific treatment - a key point when counseling patients.
Conservative (Non-operative) Management - First Line
Medications:
- NSAIDs - analgesic and anti-inflammatory; first-choice oral agent
- Short-course oral corticosteroids - may provide faster initial pain relief
- Neuropathic agents - gabapentin, pregabalin for neuropathic/radicular pain component
- Muscle relaxants - for associated cervical muscle spasm (short-term)
- Opioids - generally avoided unless severe, refractory, short-term
Physical Therapy:
- Cervical traction (mechanical or manual) - decompresses neural foramen
- Therapeutic exercise, postural training
- Manual therapy / mobilization - supported by a 2025 umbrella review (PMID 39607420) for neck disorders
- Soft cervical collar - temporary/situational use only; prolonged use leads to deconditioning
Cervical Epidural Steroid Injections (CESI):
- Can provide significant short-term pain relief and facilitate rehabilitation
- Interlaminar or transforaminal approach
- Best evidence for acute-to-subacute radiculopathy with significant pain
- Bridging therapy while awaiting natural resolution or surgery
Surgical Management
Indications for surgery:
- Absolute: Rapidly progressive or severe motor weakness, myelopathy
- Relative: Intractable pain not responding to ≥6-12 weeks of conservative care; significant neurologic deficit persisting
Surgical options:
| Approach | Procedure | Best For |
|---|---|---|
| Anterior | ACDF (Anterior Cervical Discectomy and Fusion) | Anterior pathology (disc herniation, osteophyte), multiple levels, kyphosis |
| Anterior | Total Disc Arthroplasty (TDA/ADR) | Single/two-level disc herniation, preserved motion segment, no instability |
| Posterior | Cervical Laminoforaminotomy | Foraminal stenosis, posterior/lateral pathology, lordosis preserved |
All three techniques have demonstrated good outcomes. Choice depends on sagittal alignment (kyphosis vs. lordosis), site of pathology (ventral vs. dorsal), number of levels, and surgeon experience.
Red Flags - Urgent Assessment Required
- Myelopathy signs: Gait instability, bilateral arm/leg symptoms, hyperreflexia, bladder/bowel dysfunction
- Trauma history with neurologic deficit
- Cancer history (metastatic cord compression)
- Fever + neck pain (epidural abscess, discitis)
- Progressive rapid weakness (surgical emergency)
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, 8th ed.
- Firestein & Kelley's Textbook of Rheumatology
- Spurling's test diagnostic accuracy meta-analysis (Lin et al., 2025) - PMID 39938056
- Manual therapy for neck disorders umbrella review (Reynolds et al., 2025) - PMID 39607420
- Neurodynamic tests meta-analysis (Albert-Lucena et al., 2025) - PMID 40156954
- ACR Appropriateness Criteria: Cervical Pain/Radiculopathy 2024
Staging of fatty liver diagnostic criteria how to think nafld what to keep in mind during history taking and examining the pt
Finding Sources
Finding Sources
Searching PubMed
"NAFLD" AND "fibrosis staging" AND "diagnosis"
Searching the Web
MASLD NAFLD staging diagnostic criteria FIB-4 NAS score history examination 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, deep content from Sleisenger & Fordtran and Yamada's covering clinical features, diagnosis, staging, scoring, and non-invasive tests. Let me compile the complete answer.
NAFLD/MASLD: Staging, Diagnostic Criteria, Clinical Thinking, History & Examination
1. The Diagnostic Framework - How to Think About It
The diagnostic process has three parallel goals running simultaneously:
- Confirm the presence of steatosis (imaging or biopsy)
- Exclude other causes of liver disease (alcohol, drugs, other)
- Stage the disease - is it simple steatosis, steatohepatitis, or fibrosis?
The modern MASLD diagnostic criteria require:
- Hepatic steatosis (on imaging: ≥5% of hepatocytes; on biopsy: macrovesicular fat affecting ≥5% of cells)
- Plus at least 1 cardiometabolic risk factor (obesity, T2DM, dyslipidemia, or hypertension) - this is what defines MASLD vs. other forms of steatotic liver disease
2. History Taking - What to Ask and Why
A. The First Question: Is It Really Non-Alcoholic?
This is non-negotiable. You cannot diagnose NAFLD/MASLD without actively excluding significant alcohol use.
- Ask about quantity, frequency, and pattern of alcohol use - using validated tools (AUDIT-C questionnaire)
- NAFLD is considered only when alcohol use is <20 g/day in women, <30 g/day in men (some guidelines use <20-40 g/day as the cutoff)
- Be tactful but direct - patients often underreport. Ask about weekends separately, ask about binge episodes, ask family members if needed
- If significant alcohol AND metabolic risk factors are both present, you cannot determine the dominant cause - both are assumed
B. Metabolic Risk Factors (Core History)
These are both risk factors and criteria for the diagnosis:
| Ask About | Why |
|---|---|
| BMI, weight gain history, waist circumference | Central obesity is the #1 driver; ask about weight trajectory |
| Type 2 diabetes / prediabetes | Highest risk for advanced fibrosis; ~30-40% of T2DM patients have significant fibrosis |
| Dyslipidemia | Hypertriglyceridemia, low HDL - ask about fasting lipid profiles |
| Hypertension | Part of metabolic syndrome; adds to fibrosis risk |
| Family history of T2DM, metabolic syndrome | Genetic susceptibility |
C. Drug History - Secondary Causes to Exclude
Ask specifically about:
| Drug Type | Examples |
|---|---|
| Antiarrhythmics | Amiodarone (causes macrovesicular steatosis/steatohepatitis) |
| Chemotherapy | Methotrexate, tamoxifen |
| Hormones | Corticosteroids (chronic use) |
| Antiretrovirals | HAART (nucleoside analogues especially) |
| Anticonvulsants | Valproate (causes microvesicular steatosis) |
| Others | Tetracyclines, diltiazem |
D. Surgical / GI History
- Prior bariatric surgery (jejunoileal bypass, biliopancreatic diversion - can cause NASH from SIBO and rapid weight loss)
- Extensive small bowel resection
- Total parenteral nutrition history
E. Symptoms - Most Patients Have None
- Most patients are asymptomatic (48-100% in series)
- Ask about: fatigue, malaise, vague right upper quadrant discomfort
- Absence of symptoms does not exclude NASH or even cirrhosis
- Ask about symptoms of portal hypertension in suspected advanced disease: abdominal distension (ascites), hematemesis, confusion (encephalopathy), edema
F. Risk Stratification Questions in History
Ask about features that predict advanced fibrosis:
"Red flag" features in history suggesting likely advanced disease:
- Age >50
- Obesity (especially BMI >35)
- Diabetes mellitus
- Hispanic ethnicity
- Hypertension
- Elevated ferritin (from labs)
- Known PNPLA3 risk allele (if genetic testing done)
G. Other Causes to Think About During History
- Viral hepatitis (HBV, HCV - particularly genotype 3 HCV itself can cause steatosis)
- Wilson's disease (young patient with liver disease - ask about neuropsychiatric symptoms)
- Celiac disease (associated with fatty liver)
- Hypothyroidism
- Lipodystrophy (partial or total)
- Glycogen storage diseases, abetalipoproteinemia (in appropriate clinical context)
3. Physical Examination - What to Look For
A. General Inspection
| Finding | Significance |
|---|---|
| Central obesity (waist circumference >94 cm men, >80 cm women) | Primary metabolic risk factor; visceral fat is the driver |
| BMI >25-30 | Presence and severity of metabolic risk |
| Acanthosis nigricans | Insulin resistance |
| Skin tags | Associated with insulin resistance/metabolic syndrome |
B. Abdominal Examination
- Hepatomegaly - the most common physical sign; often smooth, non-tender enlargement
- Important caveat: difficult to appreciate in obese patients due to body habitus - don't be falsely reassured by inability to palpate the liver
- Splenomegaly - suggests portal hypertension from advanced disease/cirrhosis
C. Signs of Chronic Liver Disease (Late/Advanced Disease Only)
These are present only in NASH-cirrhosis:
| Sign | Significance |
|---|---|
| Spider telangiectasias | Established cirrhosis |
| Palmar erythema | Established cirrhosis |
| Gynecomastia | Established cirrhosis |
| Leukonychia / Terry's nails | Hypoalbuminemia |
| Dupuytren's contracture | (more alcohol-related but may overlap) |
| Parotid enlargement | More specific for alcoholic liver disease |
| Asterixis | Hepatic encephalopathy |
| Ascites (fluid thrill, shifting dullness) | Portal hypertension |
| Caput medusae | Severe portal hypertension |
| Jaundice | Late decompensated disease |
D. Cardiovascular Examination
- Blood pressure measurement - hypertension is a risk factor and associated condition
- Signs of metabolic syndrome (central obesity, BP)
- NAFLD patients have increased cardiovascular mortality - cardiovascular disease is the #1 killer in NAFLD overall, exceeding liver-related mortality (liver-related mortality overtakes CV only in NASH cirrhosis)
4. Staging Systems - The Details
A. Histological Activity: The NAFLD Activity Score (NAS)
The NAS is the standard research tool from the NASH Clinical Research Network (NASH-CRN). It is not a diagnostic tool - it measures activity/severity on biopsy.
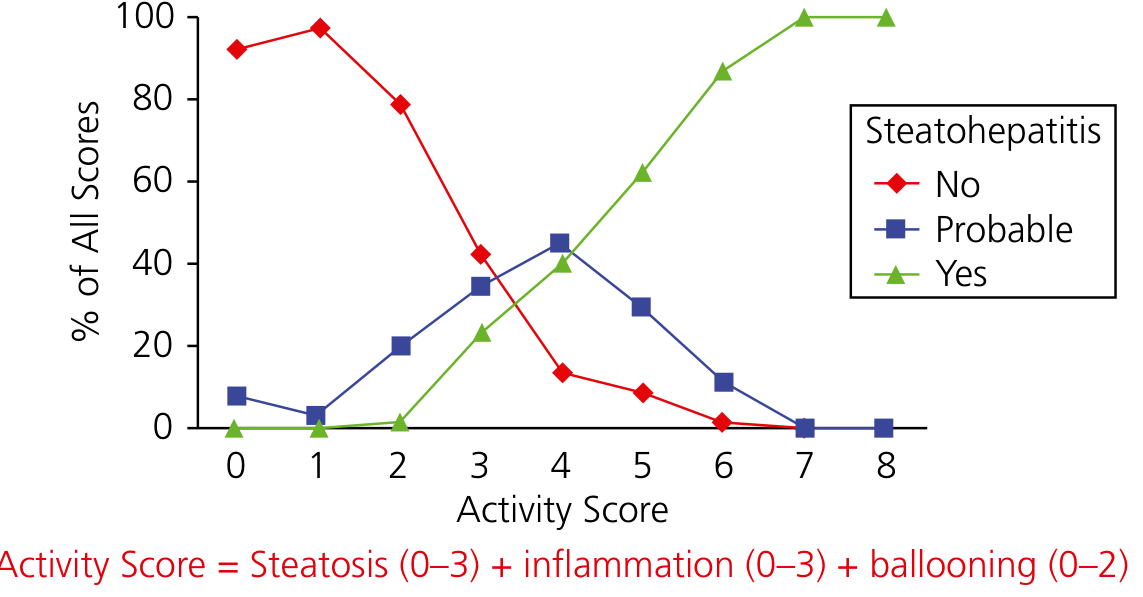
NAS = Steatosis (0-3) + Lobular Inflammation (0-3) + Hepatocyte Ballooning (0-2)
| Component | Criteria | Score |
|---|---|---|
| Steatosis | <5% hepatocytes | 0 |
| 5-33% | 1 | |
| 33-66% | 2 | |
| >66% | 3 | |
| Lobular Inflammation | No foci | 0 |
| <2 foci per 20x HPF | 1 | |
| 2-4 foci per 20x HPF | 2 | |
| >4 foci per 20x HPF | 3 | |
| Hepatocyte Ballooning | None | 0 |
| Few ballooned cells | 1 | |
| Many ballooned cells | 2 |
Interpretation:
| NAS Total | Interpretation |
|---|---|
| 0-2 | Likely NOT NASH |
| 3-4 | Indeterminate / Borderline |
| 5-8 | Likely NASH |
Critical caveat: NAS ≥5 has sensitivity 75% and specificity 83% for NASH. Only 75% of biopsies with NAS ≥5 have definite steatohepatitis; 29% of biopsies with NAS ≤4 still have steatohepatitis. NASH is a histological pattern, not just a score.
B. SAF Score (Steatosis-Activity-Fibrosis)
An alternative European system (used in clinical practice more than NAS):
- Scores steatosis (S0-S3), activity (A0-A4, combining lobular inflammation + ballooning), and fibrosis (F0-F4) separately rather than adding them together
- This allows more granularity and is considered more reliable in routine clinical practice
- NASH-CRN system remains the regulatory gold standard for clinical trials
C. Fibrosis Staging - the Most Important Prognostic Factor
Fibrosis stage is the single strongest predictor of clinical outcomes, mortality, and disease progression.
| Stage | Histological Description | Pattern |
|---|---|---|
| F0 | No fibrosis | Normal |
| F1a | Mild perisinusoidal (zone 3) | Delicate perisinusoidal collagen |
| F1b | Moderate perisinusoidal (zone 3) | Denser perisinusoidal collagen |
| F1c | Portal/periportal only | Without perisinusoidal component |
| F2 | Perisinusoidal AND periportal/portal | Both zones involved |
| F3 | Bridging fibrosis | Connects portal tracts; high risk for progression to cirrhosis |
| F4 | Cirrhosis | Regenerative nodules, distorted architecture |
Key histological note: Unlike viral hepatitis where bridging extends from portal-to-portal, in NASH bridging fibrosis often results from extension of perisinusoidal fibrosis with hepatocytes trapped within the fibrotic network - a distinctive pattern. Also notably, as fibrosis advances, steatosis, inflammation, and ballooning paradoxically decrease (the fat "burns out").
5. Non-Invasive Staging - How to Stratify Without Biopsy
Step 1 - Initial Blood Tests (First-Line in Primary Care/Clinic)
FIB-4 Index (most recommended initial test):
FIB-4 = (Age × AST) / (Platelet count × √ALT)
| FIB-4 Value | Interpretation | Action |
|---|---|---|
| <1.30 | Low risk - advanced fibrosis excluded | Monitor, no urgent biopsy |
| 1.30 - 2.67 | Indeterminate | Proceed to elastography |
| >2.67 | High risk for advanced fibrosis (F3-F4) | Refer hepatology, consider biopsy |
Note: In patients >65 years, use adjusted cutoff >2.0 as intermediate, since FIB-4 has 20-35% false-positive rate in the elderly.
NAFLD Fibrosis Score (NFS):
NFS = -1.675 + (0.037 × age) + (0.094 × BMI) + (1.13 × IFG/diabetes [yes=1, no=0]) + (0.99 × AST/ALT ratio) - (0.013 × platelet count) - (0.66 × albumin)
| NFS | Interpretation |
|---|---|
| < -1.455 | F0-F2 (advanced fibrosis excluded; NPV 88-93%) |
| -1.455 to 0.676 | Indeterminate (~25% of patients - need biopsy) |
| >0.676 | F3-F4 likely (PPV 82-90%) |
Step 2 - Elastography (If FIB-4 Indeterminate)
Transient Elastography (FibroScan/VCTE):
- Non-invasive, office-based, measures liver stiffness in kPa
- AUROC ~0.93 for advanced fibrosis (cutoff ~9.9 kPa)
- Use XL probe in obese patients
- Also measures CAP (controlled attenuation parameter) for steatosis quantification simultaneously
MR Elastography (MRE):
- Most accurate non-invasive fibrosis assessment (superior to VCTE)
- Combined with MRI-PDFF for simultaneous steatosis quantification
- Disadvantage: higher cost, limited availability
Step 3 - Liver Biopsy (When Needed)
Indications:
- FIB-4/NFS indeterminate AND elastography inconclusive
- Prior to starting pharmacological therapy
- Suspected competing or coexisting diagnosis
- High clinical suspicion of advanced disease with discordant non-invasive tests
- Before bariatric surgery if advanced liver disease suspected
6. Lab Work-Up - What to Order and Why
| Test | What It Tells You |
|---|---|
| ALT, AST | ALT > AST in NAFLD (AST/ALT <1); both mild-to-moderate elevation (1.5-4x ULN); can be normal even in NASH/cirrhosis |
| ALP, GGT | May be mildly elevated (~1/3 of patients) |
| Bilirubin, albumin, INR | Normal in uncomplicated NAFLD; abnormal in cirrhosis |
| Fasting glucose / HbA1c | Assesses diabetes/insulin resistance |
| Fasting lipid panel | Dyslipidemia assessment |
| Platelet count | Thrombocytopenia suggests portal hypertension/cirrhosis |
| Ferritin | Elevated in 20-50% of NAFLD; >1.5x ULN associated with higher NAS; does NOT mean hemochromatosis (secondary Kupffer cell iron overload) |
| ANA | Low-titer ANA (<1:320) in up to 25% - does not change management |
| TSH | Exclude hypothyroidism (secondary cause) |
| Hepatitis B/C serology | Exclude viral hepatitis (HCV genotype 3 itself causes steatosis) |
| Ceruloplasmin | Exclude Wilson's disease in younger patients |
| Anti-tissue transglutaminase (anti-tTG) | Exclude celiac disease |
| Serum iron, TIBC | If clinical suspicion for hemochromatosis |
7. Imaging - What Each Modality Does
| Modality | Detects Steatosis | Detects Fibrosis | Notes |
|---|---|---|---|
| Ultrasound | Good (>20% fat; "bright liver" with increased echogenicity) | No | First-line, cheap, available; misses <20% fat |
| CT (non-contrast) | Good (liver less dense than spleen) | No | AUROC >0.90; radiation concern |
| MRI (T1) | Excellent (fat appears bright) | Poor | |
| MRI-PDFF | Best (most accurate fat quantification) | No | Gold standard for steatosis |
| VCTE (FibroScan) | Yes (CAP) | Yes | Best combined tool for both |
| MR Elastography | Yes (MRI-PDFF simultaneously) | Best available | Limited by cost/access |
Critical point: Standard cross-sectional imaging (US, CT, MRI) cannot confirm NASH or grade fibrosis - they detect fat only.
8. The Diagnostic Algorithm (Practical Flow)
Patient presents with:
- Incidental elevated ALT/AST, OR
- Steatosis on imaging, OR
- Metabolic syndrome evaluation
↓
Step 1: EXCLUDE ALCOHOL (>20-30g/day excludes NAFLD/MASLD)
↓
Step 2: EXCLUDE SECONDARY CAUSES
(drugs, hepatitis B/C, Wilson's, hypothyroid, celiac)
↓
Step 3: CONFIRM STEATOSIS
Ultrasound → if equivocal → MRI-PDFF
↓
Step 4: CONFIRM MASLD
Steatosis + ≥1 cardiometabolic risk factor = MASLD
↓
Step 5: RISK-STRATIFY FIBROSIS (non-invasively first)
FIB-4 → If low (<1.30): low risk, monitor
→ If indeterminate (1.30-2.67): FibroScan/MRE
→ If high (>2.67): refer hepatology
↓
Step 6: LIVER BIOPSY (selective)
When non-invasive tests are indeterminate, conflicting,
or biopsy will change management
9. Key Pearls to Keep in Mind
- Normal liver enzymes do NOT exclude NASH or cirrhosis - the entire histologic spectrum including cirrhosis can be present with normal ALT/AST
- Absence of symptoms doesn't help - most patients with advanced disease are asymptomatic
- Fibrosis stage predicts mortality, not NAS - a patient with NAS 6 but F0 has better prognosis than NAS 3 with F3
- AST > ALT should make you suspect alcohol - in NAFLD it is consistently ALT > AST
- Ferritin elevated ≠ hemochromatosis in NAFLD - it's secondary iron in Kupffer cells
- ANA positivity (<1:320) in 25% of NAFLD - does not mean autoimmune hepatitis
- PNPLA3 gene variant is the most important genetic risk factor for severity and HCC risk
- As fibrosis progresses, steatosis decreases - a "burnt-out" NASH cirrhosis may have minimal fat on biopsy, making it appear cryptogenic
- Cardiovascular disease kills more NAFLD patients than liver disease - always assess and manage CV risk
- Hispanic ethnicity is independently associated with higher risk of advanced NAFLD
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, 11th ed.
- Yamada's Textbook of Gastroenterology, 7th ed.
- EASL-EASD-EASO Clinical Practice Guidelines on MASLD, Journal of Hepatology 2024
- ACR Appropriateness Criteria: Cervical Radiculopathy 2024
This is a shared conversation. Sign in to Orris to start your own chat.