Sistrunk operation
Sistrunk operation thyroglossal duct cyst procedure steps
Sistrunk Operation
Background
Why It Is Needed - Embryological Basis
- At 3 weeks of embryonic life, the thyroid gland originates as a diverticulum from the floor of the pharynx (future foramen cecum)
- It descends through the neck, passing anterior to, through, or posterior to the hyoid bone
- The tract's development is intimately linked with hyoid bone formation
- Any residual thyroid tissue or duct remnant along this path can form a cyst
Clinical Features
| Feature | Detail |
|---|---|
| Location | Midline neck, at or below hyoid (thyrohyoidal region 66%, suprahyoidal 26%) |
| Movement | Moves up on swallowing AND on tongue protrusion |
| Appearance | Smooth, soft, fluctuant, painless midline swelling |
| Complications | Infection (abscess), rupture forming a thyroglossal fistula/sinus |
| Malignant potential | Rare; suspect if rapid growth, complex on US, or calcification |
Pre-operative Assessment
- Ultrasound - first-line: confirms diagnosis, identifies normal thyroid, shows anechoic/pseudosolid well-circumscribed lesion with posterior enhancement; no internal Doppler flow
- CT/MRI - reserved for atypical cases, recurrence, or suspected malignancy
- Thyroid nuclear scan - if ultrasound cannot confirm a normal thyroid
- Routine FNA - not recommended; can be performed US-guided if diagnosis is ambiguous
- Thyroid function tests are not routinely required in a clinically euthyroid patient
Operative Steps
- Transverse (Langer's line) skin incision in the lower neck over the cyst
- Cyst dissection - careful dissection of the cyst, keeping it intact to avoid spillage (ruptured or infected cysts increase recurrence risk)
- Identification and exposure of the hyoid bone
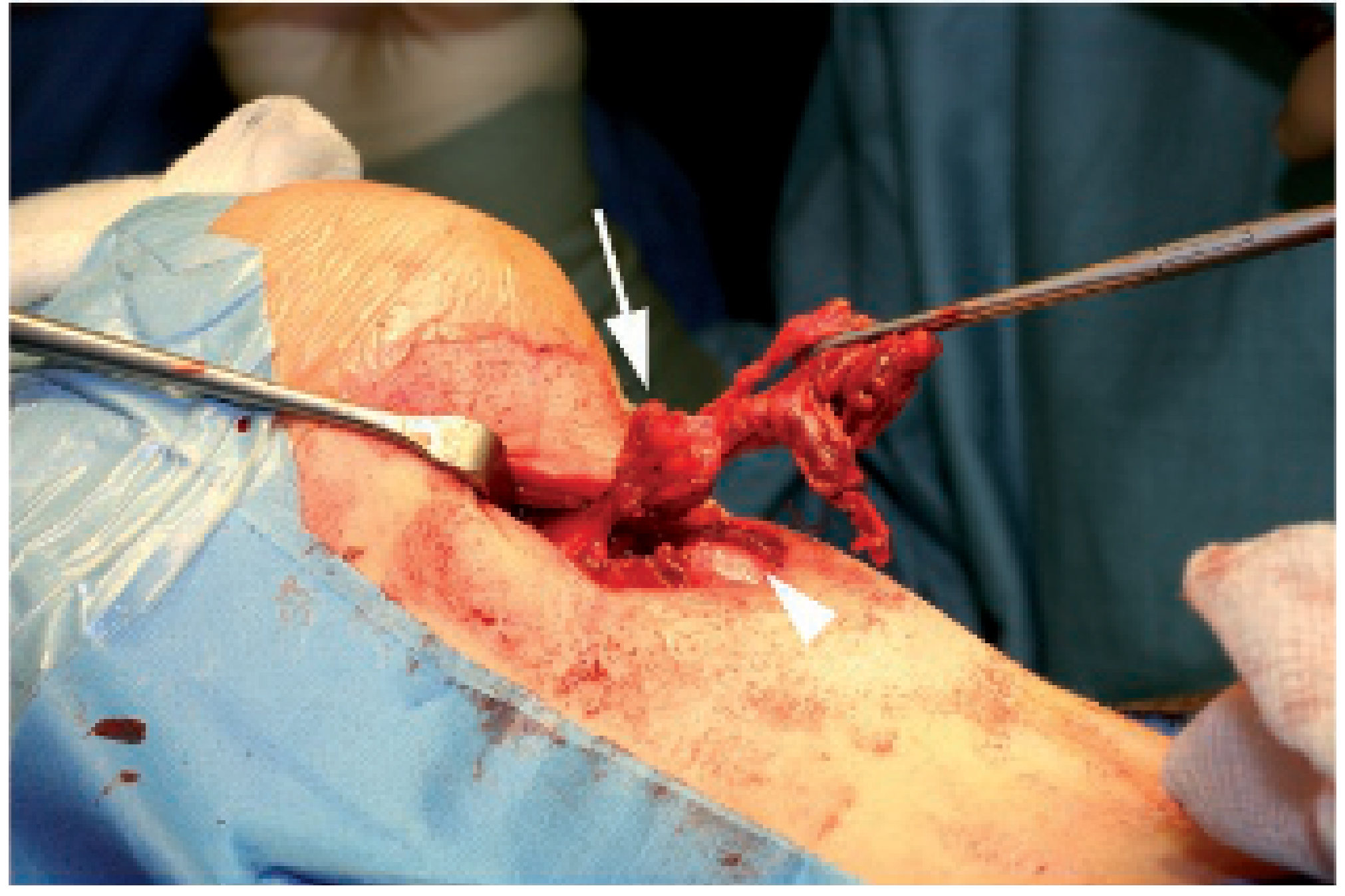
- Resection of the central (body) portion of the hyoid bone - the duct passes through or above the bone and is intimately related to it; this step is mandatory
- Dissection of the suprahyoid tract superiorly through the tongue base musculature, including a portion of the mylohyoid raphe, and a core of each genioglossus muscle
- Ligation at or near the foramen cecum - the tract is traced to the base of the tongue and ligated as high as possible at the foramen cecum
- En-bloc removal of the cyst + central hyoid + suprahyoid tract + cuff of tongue base musculature
- Copious irrigation and haemostasis (expanding haematoma can compromise airway)
- Wound closure ± drain placement (at surgeon's discretion)
The Extended / Modified Sistrunk Procedure
- Infrahyoid region extending to the thyroid isthmus
- Wider soft tissue margins including the medial strap muscles
Why the Hyoid Bone Must Be Removed
Outcomes and Recurrence Rates
| Operation Type | Recurrence Rate |
|---|---|
| Full Sistrunk operation | <5% |
| Incomplete excision (no hyoid) | ~27% |
| Sistrunk overall (all-comers) | ~5-10% |
- More than two infections prior to surgery
- Age under 2 years
- Inadequate initial operation (most common cause)
- Prior incision and drainage
Complications
| Complication | Notes |
|---|---|
| Haematoma | Can be life-threatening (airway compromise) - requires prompt drainage |
| Seroma | Common; usually resolves conservatively |
| Wound infection / stitch abscess | Common; usually managed conservatively |
| Salivary fistula | From disruption of minor salivary glands near tongue base musculature |
| Cyst recurrence | Most common serious complication; ~1-10% |
| Hypoglossal nerve injury | Rare; due to proximity during suprahyoid dissection |
Special Situation: Infected TGDC
- During an acute suppurative infection, complete excision should be deferred - distorted tissue planes greatly increase recurrence risk
- Manage with incision and drainage (or needle aspiration) + antibiotics first
- Perform the Sistrunk operation only after complete resolution of infection
- Prior infection is itself a risk factor for recurrence post-surgery
Key Points to Remember
- Sistrunk operation = excision of cyst + central body of hyoid bone + suprahyoid tract + cuff of tongue base up to foramen cecum
- Described at Mayo Clinic, 1920
- Curative in >90% of cases when performed correctly
- Removing the hyoid body is the single most important step that distinguishes it from simple cystectomy and prevents recurrence
- Always confirm normal thyroid in situ pre-operatively
- Extended Sistrunk (wider block dissection) is now the minimum recommended by some centres

Explain this in easy way in flowchart
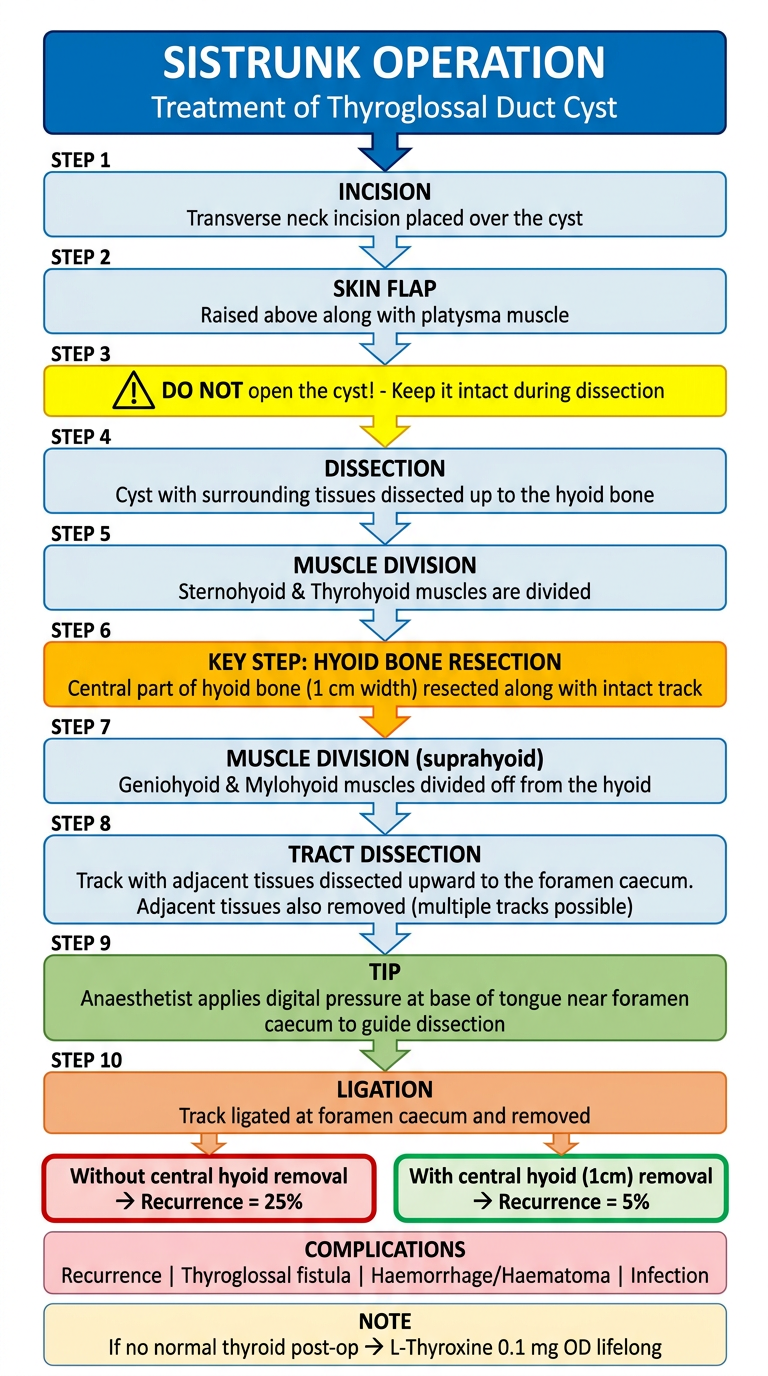
A clean, easy-to-read vertical medical flowchart titled "Sistrunk Operation - Step by Step" explaining the surgical technique for thyroglossal duct cyst removal. Use colored boxes with arrows flowing downward. Include these steps in order: TOP: Title box - "SISTRUNK OPERATION" (bold, blue header) with subtitle "Treatment of Thyroglossal Duct Cyst" STEP 1 (light blue box): "INCISION - Transverse neck incision placed over the cyst" STEP 2 (light blue box): "SKIN FLAP - Raised above along with platysma muscle" STEP 3 (yellow warning box): "⚠ DO NOT open the cyst! - Keep it intact during dissection" STEP 4 (light blue box): "DISSECTION - Cyst with surrounding tissues dissected up to the hyoid bone" STEP 5 (light blue box): "MUSCLE DIVISION - Sternohyoid & Thyrohyoid muscles are divided" STEP 6 (orange box): "KEY STEP: HYOID BONE RESECTION - Central part of hyoid bone (1 cm width) resected along with intact track" STEP 7 (light blue box): "MUSCLE DIVISION (suprahyoid) - Geniohyoid & Mylohyoid muscles divided off from the hyoid" STEP 8 (light blue box): "TRACT DISSECTION - Track with adjacent tissues dissected upward to the foramen caecum. Adjacent tissues also removed (multiple tracks possible)" STEP 9 (green box): "TIP: Anaesthetist applies digital pressure at base of tongue near foramen caecum to guide dissection" STEP 10 (orange box): "LIGATION - Track ligated at foramen caecum and removed" BOTTOM: Two result boxes side by side: - Red box: "Without central hyoid removal → Recurrence = 25%" - Green box: "With central hyoid (1cm) removal → Recurrence = 5%" COMPLICATIONS box (pink): "Recurrence | Thyroglossal fistula | Haemorrhage/Haematoma | Infection" NOTE box (light yellow): "If no normal thyroid post-op → L-Thyroxine 0.1 mg OD lifelong" Use medical illustration style, clear readable font, colorful arrows between each step, professional clean white background.
Sistrunk Operation - Easy Summary
Cut the skin (transverse neck incision) → Raise the skin flap with platysma → Do NOT open the cyst
Dissect the cyst + surrounding tissue upward → Divide Sternohyoid and Thyrohyoid muscles → Reach the hyoid bone
Resect the central 1 cm of hyoid bone with the tract inside it → Divide Geniohyoid and Mylohyoid muscles off the hyoid → Anaesthetist presses from inside the mouth (foramen caecum) to guide dissection
Dissect the tract all the way up to foramen caecum → Remove adjacent tissues too (multiple invisible side tracks can cause recurrence) → Ligate and remove
| Technique | Recurrence |
|---|---|
| Track removed WITHOUT hyoid | 25% |
| Track + central hyoid (1 cm) removed | 5% |