Draw the pathway of the nerves distribution of which leads to horner syndrome
A detailed medical diagram showing the three-neuron sympathetic pathway that causes Horner syndrome when disrupted. The diagram should be a clean anatomical illustration showing: 1. FIRST-ORDER NEURON (central): Cell body in the hypothalamus, axon descends through the brainstem (midbrain, pons, medulla) and down the lateral tegmentospinal tract to synapse at the ciliospinal center of Budge (C8-T2 intermediolateral cell column of spinal cord). Label the hypothalamus, brainstem, spinal cord levels C8, T1, T2. 2. SECOND-ORDER NEURON (preganglionic): Cell body at ciliospinal center of Budge (C8-T2). Axon exits the spinal cord, passes over the apex of the lung (label: Pancoast tumor risk), crosses the subclavian artery, travels up the sympathetic chain past the stellate ganglion, middle cervical ganglion, and synapses at the superior cervical ganglion. Label all structures. 3. THIRD-ORDER NEURON (postganglionic): Cell body in the superior cervical ganglion. Axon travels along the internal carotid artery into the cavernous sinus, then follows the ophthalmic branch of the trigeminal nerve (V1) via the nasociliary nerve into the orbit. Branches supply: Mueller's muscle of upper eyelid (ptosis if lost), pupillary dilator muscle (miosis if lost), inferior tarsal muscle (reverse ptosis), and facial sweat glands (anhidrosis if lost). Label the clinical effects on the right side: Ptosis (Mueller's muscle), Miosis (dilator pupillae), Anhidrosis (sweat glands), Enophthalmos (orbital smooth muscle). Label lesion locations with colored markers: Red = First-order lesion, Orange = Second-order lesion (e.g. Pancoast tumor, apex of lung), Blue = Third-order lesion (e.g. carotid dissection, cavernous sinus). Use a clean blue and white color scheme with clear anatomical labels, arrows showing direction of nerve signal, and a legend box explaining the three neuron orders. Professional medical illustration style.
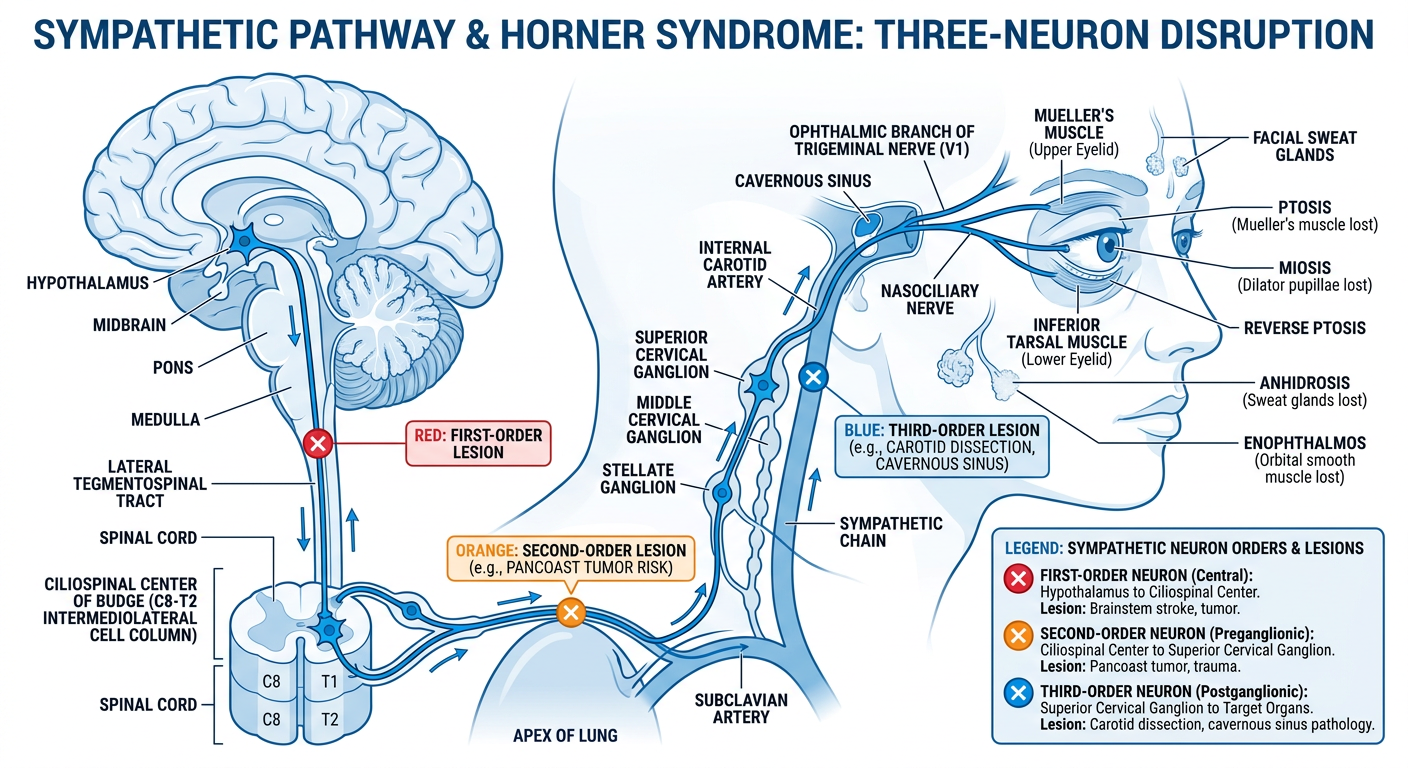
Sympathetic Pathway in Horner Syndrome
1st-Order Neuron (Central)
- Cell body: Posterior hypothalamus
- Pathway: Descends ipsilaterally through the brainstem (midbrain, pons, lateral medulla) via the lateral tegmentospinal tract
- Synapse at: Ciliospinal center of Budge-Waller (C8-T2 intermediolateral cell column)
- Lesion causes: Lateral medullary (Wallenberg) syndrome, brainstem hemorrhage/infarct, cervical cord trauma
2nd-Order Neuron (Preganglionic)
- Cell body: Ciliospinal center of Budge (C8-T2)
- Pathway: Exits the cord, loops over the apex of the lung and subclavian artery, travels along the sympathetic chain past the stellate ganglion and middle cervical ganglion
- Synapse at: Superior cervical ganglion (at the level of C2-C3, behind the bifurcation of the common carotid artery)
- Lesion causes: Pancoast tumor (apex lung tumor), cervical rib, thyroid surgery, trauma, thoracic aortic aneurysm
3rd-Order Neuron (Postganglionic)
- Cell body: Superior cervical ganglion
- Pathway (to eye): Travels along the internal carotid artery through the carotid canal, enters the cavernous sinus, joins the ophthalmic division of CN V (V1), travels via the nasociliary nerve into the orbit via the superior orbital fissure
- Pathway (to face/sweat glands): Some fibers follow the external carotid artery to facial sweat glands
- Final targets:
- Mueller's muscle (superior tarsal) → loss causes ptosis
- Pupillary dilator muscle → loss causes miosis
- Inferior tarsal muscle → loss causes lower lid elevation (upside-down ptosis)
- Facial sweat glands → loss causes anhidrosis
- Lesion causes: Carotid artery dissection, cavernous sinus thrombosis/tumor, cluster headaches, orbital lesions
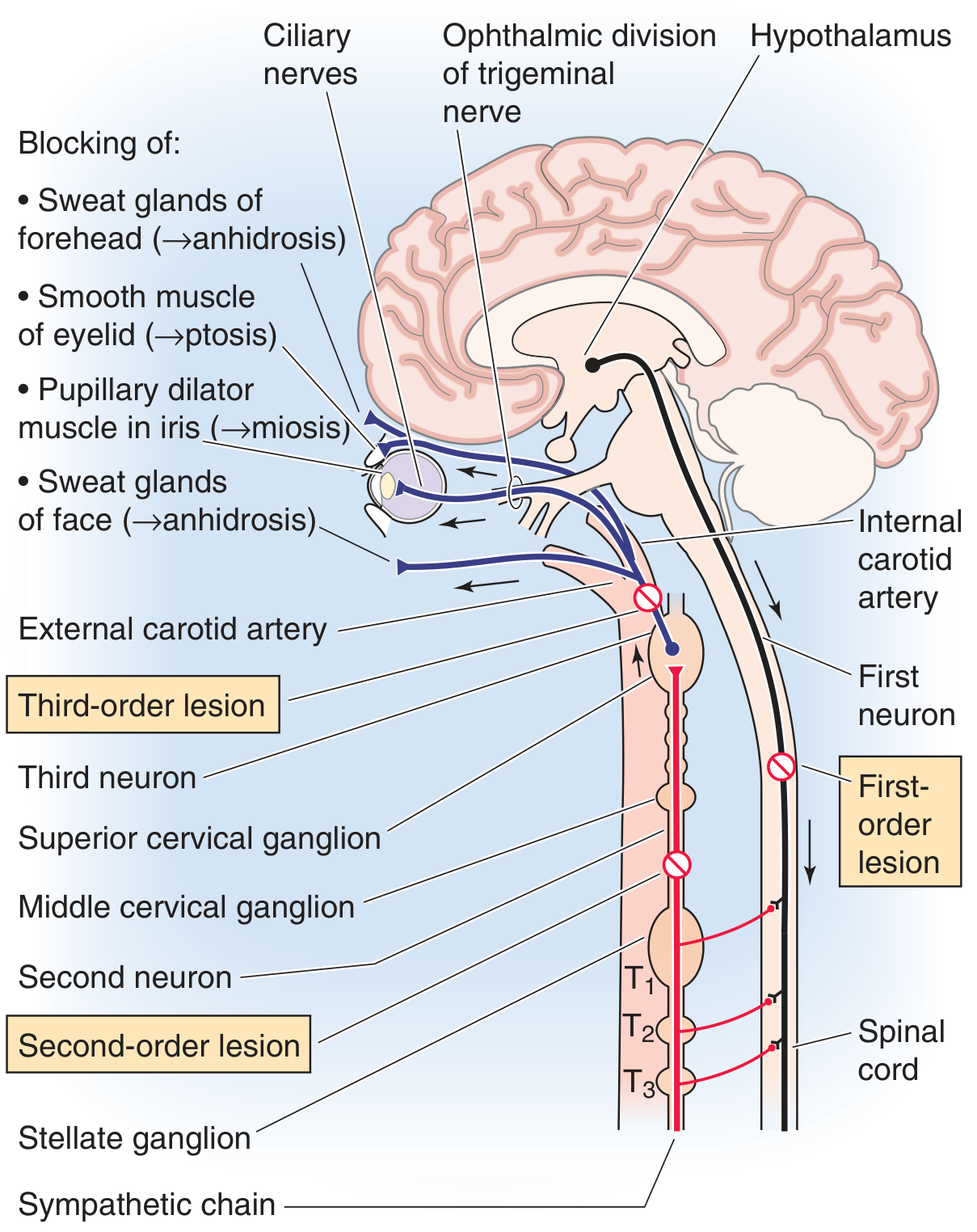
Reference Diagram from Textbook (Medical Physiology)
Classic Triad of Horner Syndrome
| Sign | Structure Lost | Mechanism |
|---|---|---|
| Ptosis | Mueller's (superior tarsal) smooth muscle | Lid droops without sympathetic tone |
| Miosis | Pupillary dilator muscle | Sphincter pupillae unopposed |
| Anhidrosis | Ipsilateral facial sweat glands | No sudomotor activation |
| (Enophthalmos) | Orbital smooth muscle | Apparent; palpebral fissure narrows |
Pharmacological Localization
- Cocaine drops (4-10%): Blocks NE reuptake - fail to dilate = confirms Horner syndrome at any level
- Hydroxyamphetamine (Paredrine 1%): Releases NE from terminals - fails to dilate only in 3rd-order (postganglionic) lesions; dilates in 1st and 2nd order lesions
Make slide on thyroid gland
ls -la /home/daytona/workspace/ 2>/dev/null | head -20; mkdir -p /home/daytona/workspace/thyroid-slides
node /home/daytona/skills/shared/scripts/fetch_images.js "https://cdn.orris.care/cdss_images/486752597f4ffad29a0e5972c68c6fabed8aa06ce8c7d4fd21ba348906b7812e.png" "https://cdn.orris.care/cdss_images/f99e8f525a00e4a54159dd3eff281a5be4d9b4a8c2428bafa0489de0833a5329.png" "https://cdn.orris.care/cdss_images/e651ad1a3083f9b584690984df21e5b765208220cdbb34a63182bd06afb85441.png" 2>/dev/null | head -5