How to tell severity of aortic stenosis from signs and symptoms only
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a clinically structured answer on assessing aortic stenosis severity from signs and symptoms alone.
Severity of Aortic Stenosis: Signs & Symptoms
The Core Principle
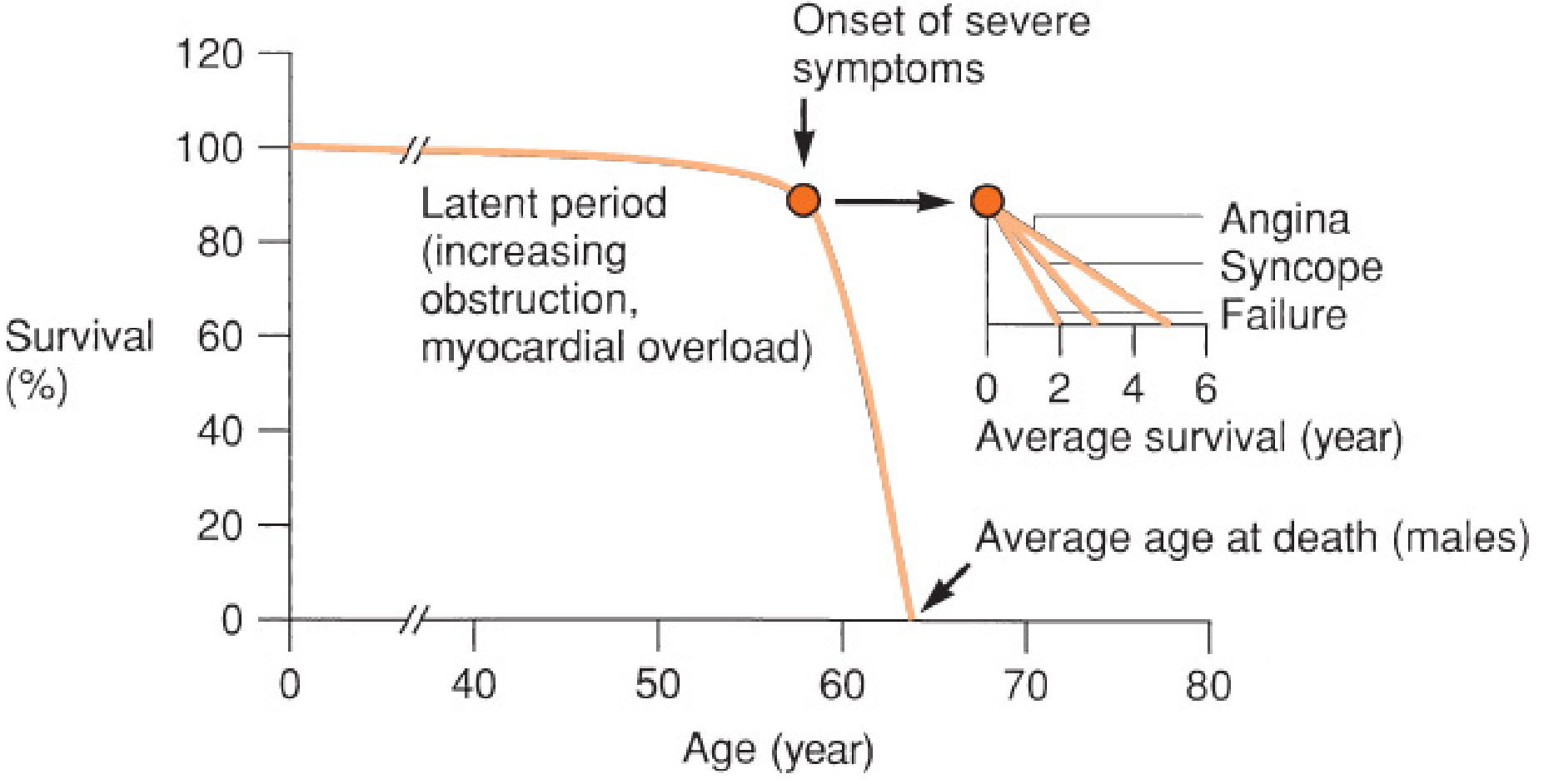
Aortic stenosis has a prolonged latent (asymptomatic) period even as obstruction worsens. Once symptoms appear, stenosis is almost always severe — and prognosis drops sharply. An elderly man with a loud aortic ejection murmur plus angina, syncope, and heart failure can be diagnosed with severe AS with high clinical certainty before any echocardiogram. — Textbook of Clinical Echocardiography
The Three Cardinal Symptoms of Severe AS
The onset of any of these symptoms signals severe disease requiring urgent evaluation and likely intervention:
| Symptom | Average survival after onset (untreated) |
|---|---|
| Angina | ~5 years |
| Syncope | ~3 years |
| Heart failure (dyspnoea, orthopnoea, PND) | ~2 years |
Patients more commonly present with exertional dyspnoea and reduced exercise tolerance before developing the classic triad. — Miller's Anesthesia; Mulholland and Greenfield's Surgery
Practical rule: No symptoms = likely mild/moderate. Any of the three cardinal symptoms = almost certainly severe.
Physical Signs and What They Suggest
| Sign | Significance |
|---|---|
| Systolic ejection murmur (best at right upper sternal border, radiating to neck) | Present in all significant AS |
| Murmur radiating to right clavicle | Supports AS; absence has a negative LR of 0.1 |
| Murmur louder, peaks later in systole (harsh, late-peaking) | More severe stenosis |
| Soft or absent A2 | Suggests severe calcific AS (reduced valve mobility) |
| Paradoxically split S2 | Severe AS with prolonged LV ejection |
| S4 gallop | Reflects LV hypertrophy and reduced compliance |
| Delayed, slow-rising carotid upstroke (pulsus parvus et tardus) | Hallmark of severe AS |
| Narrow pulse pressure | Reduced stroke volume in severe disease |
| Soft, quiet murmur in a patient with symptoms | Can indicate very severe AS with low-flow state / reduced LV function — do NOT be falsely reassured |
— Miller's Anesthesia
Putting It Together: A Clinical Severity Framework
| Clinical Picture | Likely Severity |
|---|---|
| Asymptomatic, murmur only | Mild to moderate |
| Exertional dyspnoea / decreased exercise tolerance | Moderate to severe |
| Angina on exertion | Severe |
| Exertional syncope or pre-syncope | Severe |
| Dyspnoea at rest, orthopnoea, pulmonary oedema | Severe with decompensation |
| Loud late-peaking murmur + soft A2 + delayed carotid upstroke + any of the above | Severe — refer urgently |
Key Caveats
- A soft murmur does not exclude severe AS — in low-flow/low-gradient AS (reduced LV function), murmur intensity falls even as severity is critical.
- Symptoms are the trigger for intervention — asymptomatic severe AS is generally managed conservatively, but symptomatic severe AS requires aortic valve replacement (surgical or transcatheter).
- ECG changes (LV hypertrophy with strain, LBBB, left axis deviation) support significant AS but do not grade severity.
Echocardiography remains the definitive tool for formal grading (valve area, mean gradient, jet velocity), but clinically the symptom triad is your most powerful bedside severity indicator. — Mulholland and Greenfield's Surgery; Miller's Anesthesia
This is a shared conversation. Sign in to Orris to start your own chat.