BERA waves
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a complete, textbook-based overview of BERA waves:
BERA (Brainstem Evoked Response Audiometry) Waves
BERA is also called the Auditory Brainstem Response (ABR). It records far-field electrical potentials generated by synchronized neural activity along the auditory pathway in response to an acoustic stimulus (usually a 100 µs click delivered at ~75-85 dB nHL). Between 1000-3000 sweeps are averaged to extract the signal from background noise. The normal ABR contains 5-7 peaks occurring within 10 ms of stimulus onset.
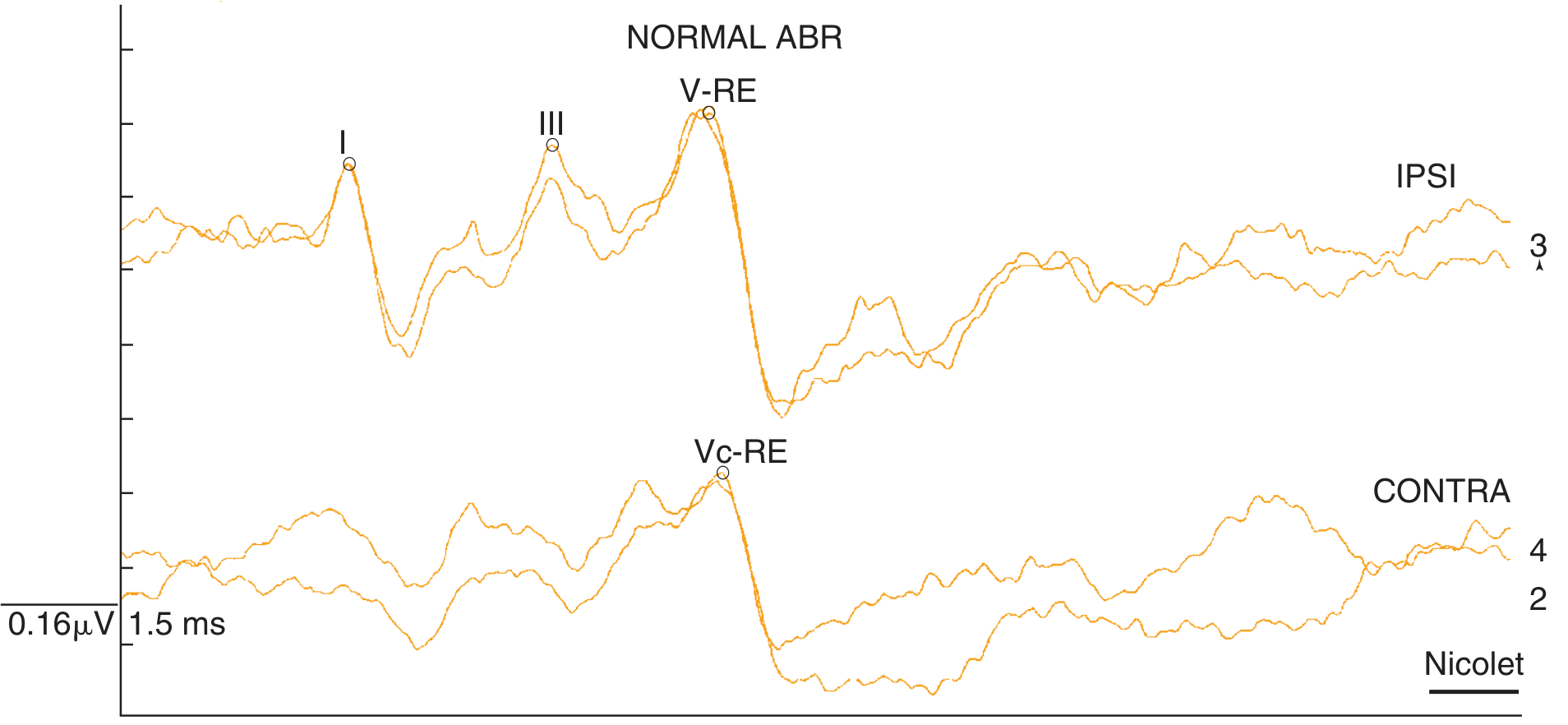
Normal two-channel ABR (ipsilateral channel shows Wave I clearly; contralateral channel separates Waves IV and V):
Wave Generators - Mnemonic: "EECOL"
| Wave | Generator Site | Approx. Latency |
|---|---|---|
| I | Distal eighth nerve (cochlear end) | ~1.7 ms |
| II | Proximal eighth nerve (near porus acusticus) | ~2.8 ms |
| III | Cochlear nucleus complex / trapezoid body | ~3.9 ms |
| IV | Superior olivary complex | ~5.0 ms |
| V | Lateral lemniscus (as it enters the inferior colliculus) | ~5.7 ms |
| VI | Inferior colliculus | >6 ms |
| VII | Inferior colliculus | >7 ms |
Note: The shift from Schwann cell (peripheral) to neuroglial cover (central) near the porus acusticus explains the distinct wave I vs wave II latency difference. Wave V is NOT generated by the inferior colliculus (as was previously thought) - it arises from the lateral lemniscus, per Moller and Jannetta's landmark study.
Waves IV and V often fuse into an IV-V complex in clinical recordings.
Normal Interpeak Latencies (IPL)
| Interval | Normal Value | Pathway Assessed |
|---|---|---|
| I - III | 2.3 ms | Cochlear nerve to cochlear nucleus (lower brainstem) |
| III - V | 2.1 ms | Cochlear nucleus to lateral lemniscus (upper brainstem) |
| I - V | 4.4 ms | Total brainstem conduction time |
Recording Technique
- Electrodes: Non-inverting at vertex/high forehead; inverting at ipsilateral earlobe; ground at mid-forehead
- Two-channel montage: Ipsilateral channel emphasizes Wave I; contralateral channel separates Waves IV and V
- Filters: High-pass 100 Hz, low-pass 1000-3000 Hz
- Stimulus: Clicks (100 µs) or tone pips at constant or alternating polarity
Wave V - The Most Important Wave
Wave V is the most robust component - it persists even with significant hearing loss and is used to:
- Estimate hearing thresholds (particularly in infants/neonates)
- Detect retrocochlear pathology
- Monitor auditory pathway integrity intraoperatively
Wave I is difficult to resolve when hearing loss exceeds 40-45 dB at high frequencies. An absent wave V in the presence of a replicated wave I or III is a definitive indicator of retrocochlear involvement.
Indicators of Retrocochlear Pathology
- Interpeak latency I-V > 4.4 ms
- Interaural latency difference of wave V > 0.2 ms (comparing left vs right ear)
- Wave V-V latency difference > 2.1 ms
- Absent or poorly formed wave V with preserved wave I/III
Key Clinical Applications
- Newborn hearing screening (UNHS programs) - ABR matures with brain development; waves I, III, V appear at ~28 weeks gestation; full maturity at ~18 months postnatal
- Acoustic neuroma/CPA tumor detection - delayed IPL or absent waves
- Neural demyelination (e.g., multiple sclerosis) - prolonged IPLs
- Intraoperative monitoring during posterior fossa or CPA surgeries
- Threshold estimation in uncooperative patients (infants, malingerers)
- Brain death evaluation - ABR unaffected by sedatives/anesthetics
Why ABR is Ideal for Objective Testing
The brainstem is relatively impervious to sedatives, anesthetics, and CNS depressants, making ABR an objective, non-volitional test. It does not require patient cooperation.
Sources: K.J. Lee's Essential Otolaryngology, p. 1211; Cummings Otolaryngology Head and Neck Surgery (Block 30); Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 689
This is a shared conversation. Sign in to Orris to start your own chat.