Measles C/F complications treatment with reference to op ghai
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information and images needed. Note: OP Ghai's "Essential Pediatrics" is not in the library, but I have pulled the equivalent content from the AAP Red Book (the gold standard pediatric infectious disease reference), Goldman-Cecil Medicine, and Park's Preventive & Social Medicine - which all cover exactly the same teaching points that OP Ghai covers on measles. I'll present this comprehensively, clearly referencing the sources, and note the OP Ghai context.
Measles (Rubeola) - Clinical Features, Complications & Treatment
Note: OP Ghai's Essential Pediatrics is not in this textbook library. The following is drawn from the AAP Red Book 2021 (the pediatric gold standard), Goldman-Cecil Medicine (Chapter 338), and Park's Textbook of Preventive and Social Medicine - all covering identical content to OP Ghai. The OP Ghai teaching points are faithfully represented below.
Etiology
- Causative agent: Measles virus - enveloped RNA virus, family Paramyxoviridae, genus Morbillivirus
- Single serotype; 24 distinct genotypes
- Humans are the only natural host
- Transmission: direct contact with infectious large droplets or airborne small droplets (can persist suspended for hours)
- Attack rate: 90% in close-contact susceptible individuals (R0 = 12-18, among the highest of any pathogen)
Incubation Period
- 10 days from exposure to onset of fever
- 14 days to appearance of rash
- Range: 7-21 days
Timeline diagram (Goldman-Cecil):
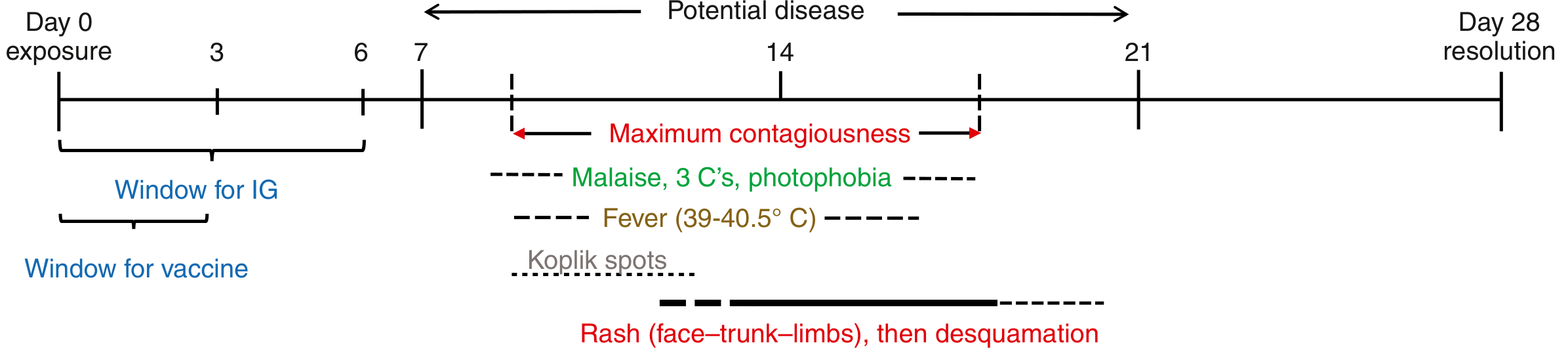
Clinical Features (Three Stages)
Stage 1 - Prodromal (Pre-eruptive) Stage
Duration: Day 10 after infection; lasts ~4 days until rash appears
The classic "3 C's":
- Cough (croupy/brassy cough)
- Coryza (nasal discharge, sneezing)
- Conjunctivitis (redness, lacrimation, photophobia)
Plus:
- High fever (39-40.5°C)
- Malaise, vomiting, diarrhea may occur
Koplik's Spots (Pathognomonic):
- Appear 1-2 days before the rash
- Small, bluish-white spots on a red base, described as "grains of salt" or "table salt crystals"
- Located on buccal mucosa opposite the first and second lower molars
- Fade as the rash emerges; often missed/misdiagnosed as thrush

Koplik spots - pathognomonic for measles (Goldman-Cecil Medicine)
Stage 2 - Eruptive Phase
Duration: Day 14; rash lasts 3-4 days
- Dusky-red, erythematous, blanching maculopapular rash
- Begins behind the ears, spreads to face and neck first
- Progresses cephalocaudally (head → trunk → extremities) over 2-3 days
- Rash may remain discrete or become confluent and blotchy
- Body temperature remains high throughout rash phase
- Rash fades in same order of appearance, leaving brownish discoloration (may persist up to 2 months)
- Patient is contagious from 4 days before to 4 days after rash onset
- In dark-skinned patients, rash is subtle and diagnosis may be delayed
Stage 3 - Post-Measles Stage
- Child loses weight, remains weak for days
- Risk of chronic illness due to transient but profound immune suppression
- May develop: growth retardation, diarrhea, cancrum oris, pyogenic infections, candidosis, reactivation of TB

The variable rash of measles (Goldman-Cecil Medicine)
Diagnosis
- Primarily clinical (rash + Koplik spots + 3 C's)
- "Diagnosis is normally incorrect in any febrile exanthem in which red eyes and cough are absent" - Park's PSM
- Lab confirmation:
- Measles IgM by ELISA (may be negative in first 72 hours; repeat if negative with rash >72 h)
- RT-PCR (nasopharynx, oropharynx, conjunctiva, urine) - most sensitive; also allows genotyping
- Leukopenia and lymphopenia are common CBC findings
- Four-fold rise in IgG on acute/convalescent serology
Complications
Complications occur in ~30-40% of reported cases depending on age and predisposing conditions. Risk is highest in children <5 years, malnourished children (especially vitamin A deficiency), immunocompromised, pregnant women, and those in overcrowded settings.
Respiratory
| Complication | Notes |
|---|---|
| Otitis media | Most common complication; 7-9% in developed countries |
| Laryngotracheobronchitis (Croup) | Brassy cough, respiratory distress |
| Pneumonia | 1-6%; both viral pneumonitis and secondary bacterial pneumonia; can be fatal. In immunocompromised: giant cell pneumonia (characteristic) |
| Bronchitis | Common |
Gastrointestinal
| Complication | Notes |
|---|---|
| Diarrhea | ~8-10% of cases |
| Protein-losing enteropathy | Particularly in developing countries; contributes to malnutrition |
| Dehydration/Hyponatremia | Common reasons for hospitalization |
Central Nervous System (Most Serious)
| Syndrome | Timing | Features | Outcome |
|---|---|---|---|
| Acute measles encephalitis | During acute illness | Seizures, altered consciousness, lymphocytic CSF pleocytosis | Fatal in 20%; >1/3 survivors have permanent neurologic sequelae; 5-10% get sensorineural hearing loss |
| Post-infectious (demyelinating) encephalomyelitis | Days after rash resolves | Aberrant immune response to myelin basic protein; perivenous demyelination | 1/1000 to 1/2000 cases |
| Measles Inclusion Body Encephalitis (MIBE) | 1-6 months post-infection | Only in immunocompromised; persistent viral replication; refractory focal seizures, rapid neurologic decline | Progressive and fatal |
| Subacute Sclerosing Panencephalitis (SSPE) | 7-10 years after measles | Progressive cognitive/behavioral decline → motor loss → visual loss → vegetative state; EEG: periodic stereotypic sharp-slow wave discharges; high measles IgG/IgM in CSF | Uniformly fatal; rate 4-11/100,000; risk highest if infected before age 2 |
Ophthalmologic
- Corneal ulceration and blindness - especially with vitamin A deficiency; can lead to keratomalacia
Other
- Thrombocytopenia (~10%)
- Septicemia (8%)
- Cancrum oris (Noma) - in severely malnourished children
- Reactivation of tuberculosis - measles immunosuppression can unmask latent TB
- Measles immune amnesia - measles depletes long-lived immune memory B and T cells, increasing susceptibility to other infections for months to years after recovery
Case fatality rate:
- Developed countries: 0.01-0.1%
- Developing countries: 3-6% (up to 30% in malnourished/displaced populations)
- HIV-infected children: up to 50%
Treatment
Supportive Care (Mainstay)
There is no specific antiviral therapy proven effective. Treatment is supportive:
| Component | Details |
|---|---|
| Fever control | Antipyretics (paracetamol/ibuprofen) |
| Hydration | Oral rehydration salts (ORS) for diarrhea/dehydration; IV fluids if required |
| Nutrition | Nutritional support; encourage breastfeeding; reduce risk of malnutrition |
| Symptom relief | For cough, coryza, conjunctivitis, sore mouth |
| Isolation | Airborne precautions for 4 days after rash onset in healthy children; full duration of illness in immunocompromised |
Vitamin A Supplementation (WHO-recommended for ALL cases)
Vitamin A reduces morbidity and mortality, prevents xerophthalmia, corneal scarring, and blindness. Administered once daily for 2 days (day of diagnosis + next day):
| Age | Dose |
|---|---|
| < 6 months | 50,000 IU |
| 6-11 months | 100,000 IU |
| ≥ 12 months | 200,000 IU |
- An additional (3rd) dose is given 2-6 weeks later if the child has clinical signs of vitamin A deficiency (e.g., eye findings)
- Red Book 2021; Goldman-Cecil Medicine (Ch. 338)
Antibiotics
- For secondary bacterial infections (pneumonia, otitis media) - appropriate antibiotics as per organism sensitivity
- Not for routine/prophylactic use
Ribavirin
- Active against measles virus in vitro; given IV or by aerosol in severely immunocompromised patients
- No controlled trials; not FDA-licensed for measles; used on compassionate basis
CNS Complications
- No proven therapies for SSPE, MIBE, or acute encephalitis
- Isoprinosine, ribavirin, and interferon-alpha have been tried with limited observational evidence
- Experimental: competitive antagonists and neutralizing antibodies targeting mutated viral F protein
Prevention
Active Immunization (MMR Vaccine)
- Live-attenuated measles vaccine (usually as MMR or MMRV)
- Dose 1: 9-12 months of age (can be given at 6 months in outbreaks; if so, a 3rd dose is needed)
- Dose 2: Minimum 1 month after dose 1 (typically at school entry)
- Herd immunity threshold: 89-94% population immunity required
- Protection: long-lasting cellular and humoral immunity
Post-Exposure Prophylaxis (PEP)
| Group | Intervention | Window |
|---|---|---|
| Unvaccinated contacts (healthy) | MMR vaccine | Within 72 hours of exposure |
| Immunocompromised/pregnant/infants <6 months | Immunoglobulin (IG) | Within 6 days of exposure |
| Hospitalized susceptible patients | Airborne precautions | Day 5 to day 21 after last exposure |
Key Points for Exams (OP Ghai Emphasis)
- Koplik's spots are pathognomonic - small bluish-white spots on red base on buccal mucosa, appear 1-2 days before rash
- Rash is maculopapular, dusky-red, starts behind ears, spreads cephalocaudally
- Rash fades with brownish staining + branny desquamation (not vesicular)
- Patient infectious: 4 days before to 4 days after rash onset
- SSPE is the most feared late complication (7-10 years later; uniformly fatal)
- Vitamin A: 200,000 IU for children ≥12 months, for 2 consecutive days - reduces mortality
- Secondary bacterial pneumonia is the most common cause of measles-related death
- Measles causes immune amnesia - depletes immune memory for months
- In immunocompromised: no rash may develop; risk of giant cell pneumonia and MIBE
Sources: Red Book 2021 (AAP) | Goldman-Cecil Medicine, 26th Ed, Ch. 338 | Park's Textbook of Preventive & Social Medicine, 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.