protocol acc to dm medicine decide acc to hba1c
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching the Web
ADA 2024 2025 type 2 diabetes treatment algorithm HbA1c based stepwise protocol
Reading File
Reading Web Page
https://www.medils.com/static/guide/ADA-Pharmacologic-Approa…
Loading Image
I now have all the information needed. Here is the complete DM treatment protocol based on HbA1c:
Type 2 Diabetes (DM) Treatment Protocol - Based on HbA1c
Glycemic Targets (HbA1c Goals)
| Patient Group | HbA1c Target |
|---|---|
| Most adults with T2DM | < 7.0% (53 mmol/mol) |
| Young, no comorbidities, long life expectancy | < 6.5% |
| Elderly, frail, hypoglycemia-prone, short life expectancy | < 8.0-8.5% |
| Pregnancy (T1DM/T2DM) | < 6.0-6.5% |
Key principle: Monotherapy with most noninsulin agents reduces HbA1c by 0.5-2.0%. If HbA1c is > 8.5%, a single agent will likely be insufficient - combination therapy should be considered upfront.
Step 1 - Foundation for ALL patients at diagnosis
Lifestyle modification + Metformin
- Diet, exercise (≥150 min/week moderate activity), weight loss (5-10%)
- Metformin: start 500 mg once or twice daily with meals, increase gradually
- Target dose: up to 1000 mg twice daily (max 2550 mg/day)
- HbA1c reduction: 1.0-1.5%
- Hold if eGFR < 30 mL/min; check vitamin B12 on long-term use
Step 2 - Choose next agent based on comorbidities AND HbA1c
Here is the algorithm from Goldman-Cecil Medicine:
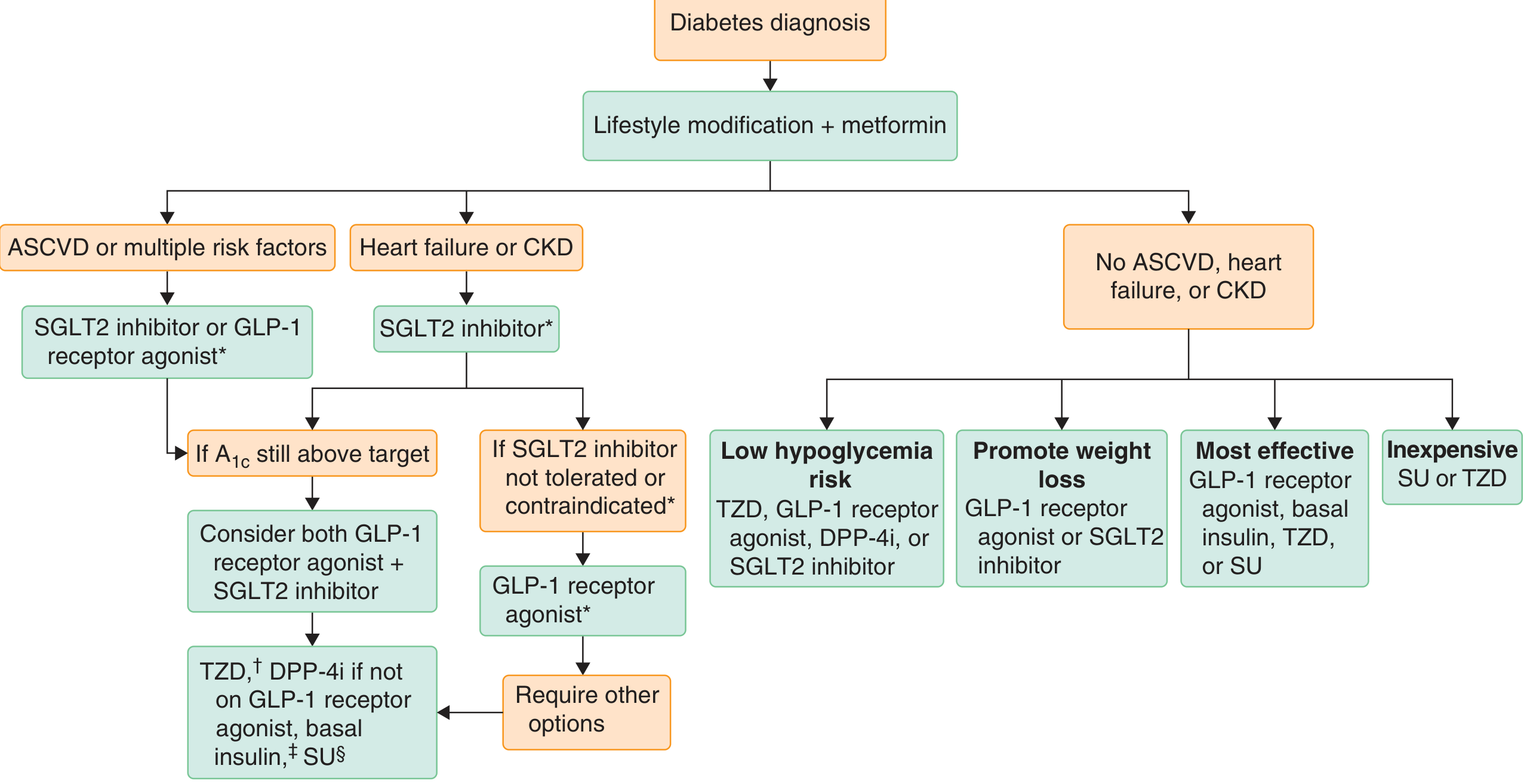
Branch A: ASCVD or multiple CV risk factors
- Add SGLT2 inhibitor OR GLP-1 receptor agonist (independent of HbA1c - for CV protection)
- If HbA1c still above target: combine both GLP-1 RA + SGLT2i
- Further escalation: TZD, DPP-4i (if not on GLP-1 RA), basal insulin, or SU
Branch B: Heart failure or CKD
- Add SGLT2 inhibitor (first choice - proven renal and cardiac protection)
- If SGLT2i not tolerated/contraindicated: switch to GLP-1 receptor agonist
- If still uncontrolled: TZD, DPP-4i, basal insulin, SU
Branch C: No ASCVD, no HF, no CKD (glucose-focused approach)
Choose based on priority:
| Priority | Drug(s) of Choice |
|---|---|
| Low hypoglycemia risk | TZD, GLP-1 RA, DPP-4i, or SGLT2i |
| Weight loss desired | GLP-1 RA or SGLT2i |
| Maximum HbA1c lowering | GLP-1 RA, basal insulin, TZD, or SU |
| Cost-sensitive | SU (sulfonylurea) or TZD |
HbA1c-Guided Escalation Summary
| HbA1c at presentation | Approach |
|---|---|
| < 7.5% | Lifestyle + Metformin monotherapy; reassess in 3 months |
| 7.5-9.0% | Metformin + 1 add-on agent (chosen by comorbidities above) |
| > 9.0% | Dual/triple combination therapy from start; consider early insulin |
| > 10-12% or symptomatic | Insulin initiation (basal insulin ± prandial), then simplify later |
Drug Classes - HbA1c Lowering Capacity
| Drug Class | HbA1c Reduction | Notes |
|---|---|---|
| Metformin | 1.0-1.5% | First-line; no hypoglycemia |
| GLP-1 RAs (liraglutide, semaglutide, dulaglutide) | 1.0-1.2% | Weight loss, CV benefit |
| Tirzepatide (GIP + GLP-1 dual agonist) | 1.5-2.0%+ | Best-in-class for HbA1c + weight |
| SGLT2 inhibitors (empagliflozin, dapagliflozin) | 0.5-1.0% | CV/renal protection, weight loss |
| Sulfonylureas (glimepiride, glipizide) | 1.0-1.5% | Cheap; hypoglycemia risk |
| DPP-4 inhibitors (sitagliptin, vildagliptin) | 0.5-0.8% | Weight-neutral; safe in CKD (dose-adjust) |
| TZDs (pioglitazone) | 1.0-1.5% | Weight gain, fluid retention |
| Basal insulin (glargine, detemir, degludec) | 1.5-3.5% | Most potent; hypoglycemia risk |
Insulin Initiation (when oral agents fail)
- Start basal insulin: 10 units/day OR 0.1-0.2 units/kg/day at bedtime
- Titrate: Increase by 2 units every 3 days to reach fasting glucose target (FPG 80-130 mg/dL)
- If HbA1c still > 8%: Add prandial insulin with the largest meal (4 units or 10% of basal dose)
- Stepwise prandial addition: add to 2nd meal, then 3rd meal (basal-bolus regimen)
- If HbA1c < 8% when adding prandial: reduce basal by 4 units or 10% to avoid hypoglycemia
2025 ADA Update - Key Changes
Per the ADA 2025 Standards of Care:
- Combination therapy earlier is now favored over purely stepwise addition for patients with high baseline HbA1c
- GLP-1 RAs and tirzepatide are recommended broadly - not just for weight or CV risk but also for MASLD (fatty liver disease)
- Pharmacotherapy should start at diagnosis without delay
- GLP-1 RAs preferred for T2DM + CKD to reduce CV and kidney disease risk
Sources: Goldman-Cecil Medicine (26th ed.), p. 2477; ADA Standards of Care 2025 (Diabetes Care 48 Suppl.1)
This is a shared conversation. Sign in to Orris to start your own chat.