Describe the role of HPV in etiopathogenesis, differential diagnosis in carcinoma cervix.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
HPV cervical carcinoma etiopathogenesis
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
HPV cervical cancer molecular mechanism oncogenesis
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive, authoritative content from multiple textbooks and two excellent diagrams. I can now compose a thorough, well-structured answer.
HPV in the Etiopathogenesis and Differential Diagnosis of Carcinoma Cervix
1. Overview: HPV as the Central Etiologic Agent
Human papillomavirus (HPV) is the single most important etiologic factor in carcinoma of the cervix. All major subtypes of invasive cervical carcinoma - squamous cell carcinoma (80%), adenocarcinoma and mixed adenosquamous carcinoma (~15%), and small cell neuroendocrine carcinoma (<5%) - are caused by high-risk HPV. HPV is a necessary but not sufficient cause; additional co-factors drive malignant transformation.
- Robbins & Kumar Basic Pathology, p. 685-688
2. Virology of HPV
HPV is an icosahedral, nonenveloped, double-stranded DNA virus (~8000 base pairs, 55 nm diameter). Its genome has three regions:
| Region | Components | Function |
|---|---|---|
| Early (E) region | E1, E2, E4, E5, E6, E7 | Viral replication and cellular transformation |
| Late (L) region | L1, L2 | Capsid proteins (L1 = 54 kDa major capsid; L2 = 77 kDa minor capsid) |
| Non-coding region | Upstream regulatory region | Contains regulatory elements |
E6 and E7 are the key oncoproteins responsible for malignant transformation.
Over 200 HPV types are identified. ~40 types infect the anogenital tract, divided into:
-
High-risk types (HPV 16, 18, 31, 33, 45, 52, 58): associated with CIN and invasive carcinoma. HPV 16 and 18 together account for ~70% of all CIN and cervical carcinomas.
-
Low-risk types (HPV 6, 11): cause genital warts (condylomas) and ~10% of low-grade cervical lesions.
-
Harrison's Principles of Internal Medicine 22E, p. 1569
3. Route of Infection and Tissue Tropism
HPV is a tissue-tropic virus that targets basal keratinocytes of specific epithelial sites. Infection occurs after microtrauma exposes basal cells to the virus. The virus replicates as keratinocytes differentiate; virions assemble in the nuclei of differentiated keratinocytes and are shed during desquamation. Transmission is by direct contact (typically sexual).
The transformation zone (TZ) - the area between the original squamocolumnar junction (SCJ) and the new SCJ - is the principal site of vulnerability. Metaplastic squamous cells here are immature, actively dividing, and susceptible to HPV integration. CIN and virtually all invasive carcinomas arise in the TZ.
4. Molecular Pathogenesis: The Role of E6 and E7
The Critical Distinction: Episomal vs. Integrated HPV
| State | HPV Type | Outcome |
|---|---|---|
| Episomal (non-integrated) | Low-risk (6, 11) | Condyloma; no malignant transformation |
| Integrated into host genome | High-risk (16, 18) | Disrupts E1/E2 repressor → increased E6/E7 expression → carcinogenesis |
Integration always disrupts the E1/E2 open reading frame, leading to:
- Loss of the E2 viral repressor (which normally keeps E6/E7 in check)
- Overexpression of E6 and E7 oncoproteins
- Increased genomic instability, enabling accumulation of additional pro-oncogenic mutations
E6 Oncoprotein Actions
- Binds and degrades p53 (via ubiquitin-mediated proteasomal degradation) - removes the cell's "guardian of the genome"
- Upregulates telomerase (TERT) - promotes cellular immortalization
- E6 from high-risk HPV types has higher affinity for p53 than low-risk E6 (key distinction)
E7 Oncoprotein Actions
- Binds RB protein, displacing E2F transcription factors that are normally sequestered - drives cells through the G1/S checkpoint
- Inactivates CDK inhibitors p21 and p27 - further removing cell cycle brakes
- Activates cyclins A and E - accelerates S-phase entry
- E7 from high-risk HPV has higher RB affinity than low-risk E7
Net Oncogenic Effect
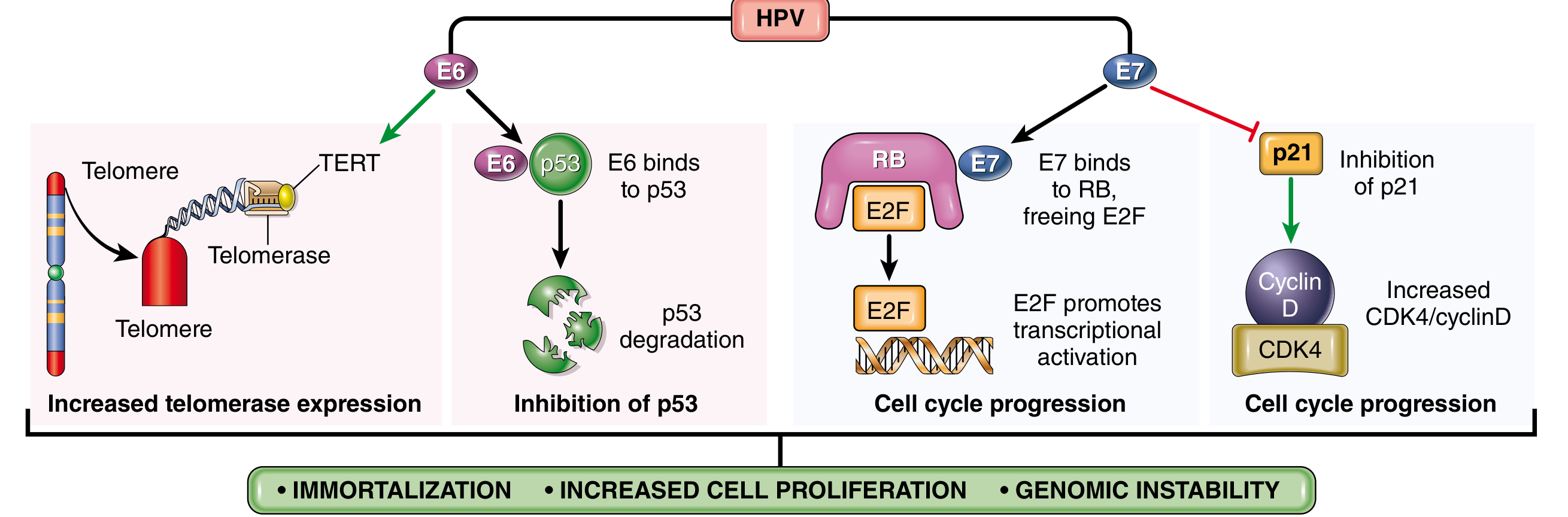
E6 and E7 together produce: immortalization (via TERT) + increased cell proliferation (via RB/E2F and CDK inhibitor disruption) + genomic instability (via p53 loss)
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 306-307
- Robbins & Kumar Basic Pathology, p. 685-686
5. The SIL/CIN-to-Carcinoma Continuum (Stepwise Pathogenesis)
Sequence of Events
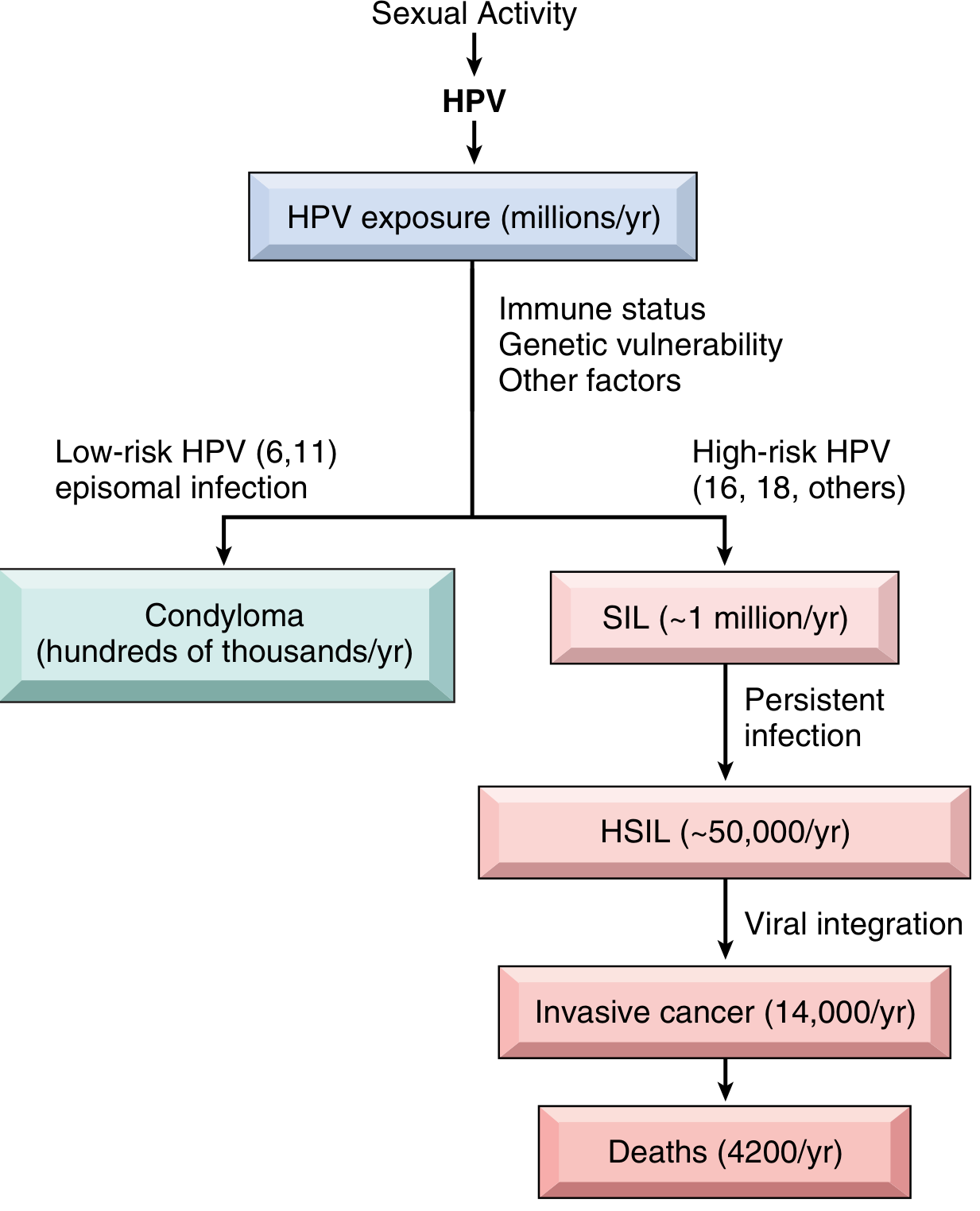
High-risk HPV (16, 18) → persistent infection → SIL → HSIL (via viral integration) → invasive carcinoma
Classification and Natural History
| Lesion | CIN Equivalent | Regress | Persist | Progression |
|---|---|---|---|---|
| LSIL | CIN I | 60% | 30% | 10% (to HSIL) |
| HSIL | CIN II, III | 30% | 60% | 10% (to carcinoma) |
Progression within 2-10 years
Key points:
-
LSIL: High viral replication, mild host cell alteration - NOT premalignant; most regress spontaneously
-
HSIL: Increased proliferation, arrested maturation, low viral replication - genuinely premalignant, ~10% progress to invasive cancer
-
SIL peaks at ~30 years; invasive carcinoma peaks at ~45 years - a 10-15 year lag
-
~20% of HSIL arise de novo, without a preceding LSIL phase
-
Despite millions of HPV infections annually, only ~14,000 develop into invasive cancers per year in the US - reflecting the role of host immunity and co-factors
-
Robbins & Kumar Basic Pathology, p. 686-688
6. Co-factors Required for Malignant Transformation
HPV infection alone is not sufficient for carcinogenesis. Additional factors include:
| Co-factor | Mechanism |
|---|---|
| Cigarette smoking | Carcinogens in cervical mucus act as co-carcinogens |
| Immunosuppression (e.g., HIV) | Reduces CD4+ T cell-mediated immune surveillance; higher rates of persistent HPV |
| Multiple sexual partners / early age at first intercourse | Increased HPV exposure and probability of high-risk strain contact |
| Coexisting STIs (HSV-2, Chlamydia) | Inflammation, DNA damage, impaired immune clearance |
| Dietary deficiencies | Nutritional co-factors (folate, vitamins) |
| Hormonal changes | Oral contraceptive use (long-term) |
| Mutated RAS and other oncogenic mutations | In vitro: HPV-transfected keratinocytes only form tumors when co-transfected with mutated RAS |
7. Morphology of Invasive Carcinoma
Invasive carcinomas develop in the transformation zone, ranging from microscopic stromal invasion to grossly visible exophytic tumors:
- Microscopically: Tongues and nests of squamous cells with desmoplastic stromal response; grading based on squamous differentiation (keratin pearls in well-differentiated tumors)
- "Barrel cervix": Tumors encircling the cervix, penetrating into stroma
- Parametrial extension: Can affix uterus to pelvic structures
- Spread: Risk of pelvic lymph node metastasis correlates with depth of invasion (<1% for <3 mm; >10% for >3 mm invasion)
- Rare variants: Small cell neuroendocrine carcinoma - morphologically resembles small cell lung carcinoma; very poor prognosis
8. Differential Diagnosis of Carcinoma Cervix
The differential diagnosis encompasses lesions that can mimic cervical carcinoma clinically, colposcopically, or histologically:
A. Benign/Premalignant Cervical Lesions
| Condition | Key Distinguishing Features |
|---|---|
| Cervical ectropion (erosion) | Columnar epithelium exposed on ectocervix; common in young women/OCP users; non-malignant, bleeds on contact but colposcopy/biopsy benign |
| Cervicitis (acute/chronic) | Infectious etiology (gonorrhea, chlamydia, trichomonas, herpes); inflammatory exudate; culture/PCR positive; no dysplastic cells on Pap |
| LSIL / CIN I | Koilocytosis, mild nuclear atypia confined to lower third; HPV productive infection; managed conservatively |
| HSIL / CIN II-III | Full-thickness dysplasia without invasion; managed with excision (LLETZ/cone biopsy); no stromal invasion |
| Cervical polyp | Pedunculated benign polyp of endocervical glands; soft, red, bleeds easily; benign histology |
| Nabothian cysts | Mucous retention cysts; smooth, pale yellow; entirely benign |
B. Malignant - Primary Cervical Tumors (Subtypes to Distinguish)
| Type | Features |
|---|---|
| Squamous cell carcinoma (most common, 80%) | Keratinizing or non-keratinizing; arises from SCJ; HPV 16/18 |
| Adenocarcinoma (~15%) | Endocervical glandular origin; endocervical or endometrioid pattern; HPV 18 predominant; Pap test less sensitive |
| Adenosquamous carcinoma | Mixed glandular and squamous components |
| Small cell neuroendocrine carcinoma (<5%) | Resembles small cell lung Ca; synaptophysin/chromogranin positive; most aggressive |
| Clear cell carcinoma | Rare; associated with DES exposure in utero |
| Glassy cell carcinoma | Poorly differentiated; large cells with "ground glass" cytoplasm |
C. Non-Cervical Pelvic Lesions Mimicking Cervical Carcinoma
| Condition | How to Differentiate |
|---|---|
| Endometrial carcinoma extending to cervix | Endometrial biopsy/curettage; MRI shows endometrial primary; ER/PR positive; HPV negative |
| Cervical leiomyoma | Smooth muscle origin; firm, whorled; US and MRI show heterogeneous mass without invasion; benign histology |
| Vaginal carcinoma extending to cervix | Primary vaginal tumor extending upward; if cervix is involved, consider cervical primary by convention |
| Metastatic carcinoma to cervix | Rare; from colon, ovary, breast; clinical history; immunohistochemistry |
| Cervical endometriosis | Blue-red nodules; cyclic symptoms; no cytologic atypia |
| Condyloma acuminatum | Exophytic, cauliflower-like; low-risk HPV 6/11; koilocytosis but no invasion |
D. Imaging Differential (MRI/CT)
On imaging, cervical carcinoma must be distinguished from:
-
Cervical leiomyoma: hypointense T2 signal, well-defined margins, no parametrial invasion
-
Nabothian cysts: simple cysts, T2 bright
-
Cervicitis with hypertrophy: No stromal invasion; resolves with treatment
-
Hydro/haematometra: Secondary to canal obstruction by tumor; distinguish from primary uterine pathology
-
Grainger & Allison's Diagnostic Radiology, p. 876
9. Immune Escape in HPV Carcinogenesis
In HPV-associated cancers:
- HPV infection has no viremic phase, so antibody responses are incomplete (~60-70% of infected individuals develop detectable antibodies)
- CD4+ T cell regulation is critical - immunosuppressed patients (especially HIV+) have higher rates of progression
- Measurable suppression of antigen presentation and antitumor activity in established cancers
- Strong T cell response to HPV16 E2 protein is associated with non-progression
10. Prevention and Vaccine Relevance
The effectiveness of HPV vaccines (targeting primarily HPV 16, 18, and low-risk 6, 11) in preventing CIN and cervical carcinoma directly validates the causal role of HPV in cervical carcinogenesis - Robbins, Cotran & Kumar (p. 307).
Recent Literature (2024-2026)
Recent reviews continue to refine our understanding:
- Legaki et al., 2026 (PMID 41596450): Highlights both genetic and epigenetic mechanisms (promoter methylation, histone modification) in HPV-driven cervical carcinogenesis, alongside evolving diagnostic approaches.
- Singh et al., 2026 (PMID 41697429): Emphasizes the role of HPV variants and host genetic susceptibility in determining who progresses from infection to carcinoma.
- Xiao et al., 2025 (PMID 40350456): Broad review of viral oncogenesis mechanisms, placing HPV E6/E7 within the broader context of cancer hallmarks.
No findings in these recent reviews contradict the mechanisms described above; they expand on epigenetic co-factors and host genetics.
Summary: HPV - specifically high-risk types 16 and 18 - drives cervical carcinogenesis through integration into host DNA, with consequent overexpression of E6 (which degrades p53 and activates telomerase) and E7 (which inactivates RB, p21, p27, and activates cyclins). The result is unchecked cell proliferation, immortalization, and genomic instability. The progression from infection through SIL/CIN to invasive carcinoma spans 10-15 years and requires co-factors (immunosuppression, smoking, coinfections). Differentiating cervical carcinoma from its mimics requires integration of clinical features, Pap cytology, colposcopy, biopsy with immunohistochemistry, and cross-sectional imaging.
This is a shared conversation. Sign in to Orris to start your own chat.