
17792133843297022640685362770055.jpg
Do we first give antibiotic or dexamethasone or expedite the delivery and what is the appropriate action
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information to answer this question definitively. Here is the full explanation:
Question 25 — The Answer is (c) Expedite Delivery
Clinical Scenario Analysis
The patient is:
- 32-year-old primigravida
- PPROM at 34/52 weeks (late preterm)
- Temperature 39°C (fever)
- Pulse 100 bpm (tachycardia)
- Uterine tenderness
This is a classic triad of clinical chorioamnionitis (intrauterine infection):
"Clinical signs of chorioamnionitis include fever (>38°C), maternal and fetal tachycardia, uterine tenderness, and foul-smelling or purulent amniotic fluid." — Morgan & Mikhail's Clinical Anesthesiology
Why Expedite Delivery is the Most Appropriate Action
Once chorioamnionitis is established, delivery is the definitive treatment — you cannot cure an intrauterine infection by staying pregnant. The PROM management algorithm (Creasy & Resnik, Figure 39.2) is explicit:
When intrauterine infection is present → Deliver, with broad-spectrum antibiotics
The algorithm shown above confirms: in any gestational age, if intrauterine infection is identified, the branch goes directly to delivery (not conservative management, not just antibiotics alone).
At 34 weeks specifically:
"Conservative management increases the risks for chorioamnionitis and prolonged hospitalization." "Delivery should be considered after antenatal corticosteroid benefit has been achieved if delivery is planned within 7 days."
But here, infection is already present — there is no waiting.
What About Antibiotics and Dexamethasone?
| Option | Role in This Case |
|---|---|
| Antibiotics | Given alongside delivery (not instead of it). Broad-spectrum antibiotics are started immediately but do not replace delivery. They treat maternal/neonatal sepsis peripartum. |
| Dexamethasone | Given in uncomplicated PPROM without infection, to accelerate fetal lung maturity while awaiting delivery. When infection is already present and delivery is being expedited, steroids are secondary and cannot delay delivery. |
| Expedite delivery | Primary action — chorioamnionitis is an absolute indication to deliver regardless of gestational age. |
The key distinction: antibiotics and steroids are adjuncts to conservative management in preterm PPROM without infection. Once infection is clinically confirmed, the management shifts entirely to delivery + antibiotics, not watchful waiting with steroids.
The PROM Algorithm (Creasy & Resnik)
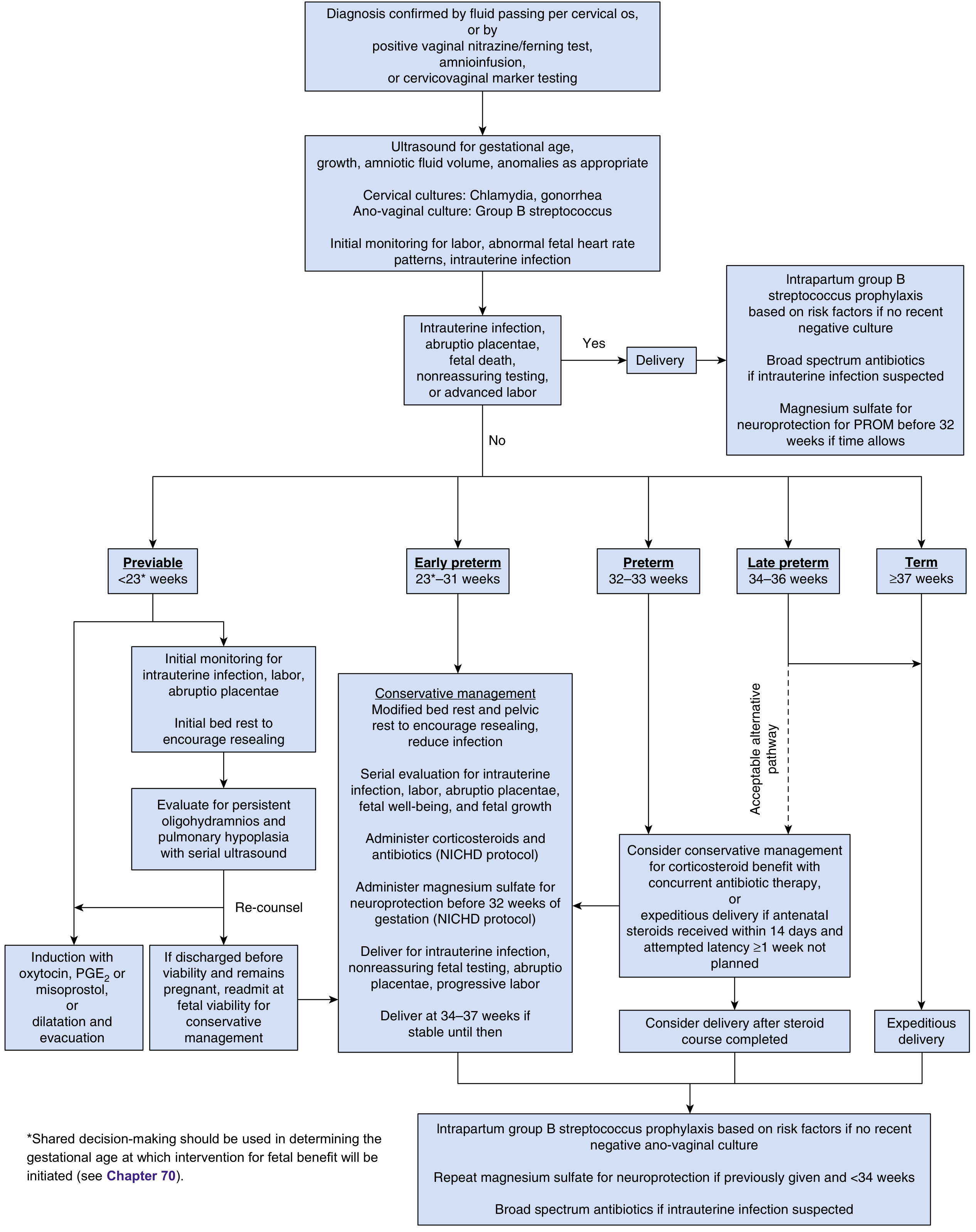
The top branch of this algorithm confirms: Intrauterine infection, nonreassuring fetal testing, advanced labor → YES → Delivery (with broad-spectrum antibiotics alongside).
Summary
The correct answer is (c) Expedite delivery.
- Fever 39°C + tachycardia + uterine tenderness = clinical chorioamnionitis
- Chorioamnionitis at any gestational age = absolute indication for delivery
- Broad-spectrum antibiotics are started concurrently but do not replace delivery
- Dexamethasone is for lung maturity in uninfected preterm PPROM managed conservatively — it is not the primary action when infection is established
Source: Creasy & Resnik's Maternal-Fetal Medicine, p. 924–926; Morgan & Mikhail's Clinical Anesthesiology, p. 1641

17792139738661047271895918402184.jpg
First Give antibiotic or dexamethasone with tocolytics
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Now I have everything needed. Let me answer both questions in the image comprehensively.
Question 32 — PPROM at 32 Weeks, No Infection
The answer is (a) Give tocolytics and dexamethasone
But the deeper question you're asking is: what is the order of priority, and do antibiotics come before dexamethasone?
The Correct Priority Order in Uncomplicated PPROM at 32 Weeks
This patient has no fever, no tachycardia, no uterine tenderness — so there is no chorioamnionitis. The approach is conservative (expectant) management, and the interventions are initiated together, but in this order of therapeutic priority:
1. 🔴 Antibiotics — FIRST (and most critical)
Broad-spectrum antibiotics (ampicillin + erythromycin — the NICHD protocol) are started immediately upon diagnosis of preterm PPROM, before or alongside steroids. Why?
"Broad-spectrum antibiotic (ampicillin/amoxicillin plus erythromycin) therapy for women with preterm PROM before 32 weeks' gestation prolongs pregnancy sufficiently to reduce neonatal gestational age-dependent morbidities and reduce the frequencies of maternal and neonatal infections. Up to a 7-day course of parenteral and oral therapy is recommended." — Creasy & Resnik's Maternal-Fetal Medicine, p. 927
Antibiotics serve two purposes in preterm PPROM:
- Prolong the latency period (delay delivery)
- Reduce risk of ascending chorioamnionitis
2. 🟡 Dexamethasone (Antenatal Corticosteroids) — Given Concurrently / Shortly After
Dexamethasone (or betamethasone) is given to accelerate fetal lung maturity. At 32 weeks, fetal lungs are immature and RDS is a major risk. The NICHD protocol specifies:
"Administer corticosteroids and antibiotics (NICHD protocol)" — the two are given together.
The full steroid course takes 48 hours for maximum benefit (2 doses of dexamethasone 12 mg IM, 12 hours apart).
3. 🟢 Tocolysis — Limited Role, Controversial
Tocolytics have a very limited role in PPROM:
"Therapeutic tocolysis, administered only after contractions occur, has not been shown to be effective in prolonging latency after PROM."
"Aggressive tocolysis was not associated with longer latency (3.8 versus 4.5 days; P = .16)." — Creasy & Resnik, p. 927
Tocolysis may be used briefly (24–48 hours) only to "buy time" for steroid administration to complete — not for long-term prolongation. It is NOT given indefinitely. The APOSTEL-III trial data confirm it does not significantly alter composite adverse neonatal outcomes.
Summary Table
| Intervention | Order | Rationale |
|---|---|---|
| Antibiotics (Ampicillin + Erythromycin) | 1st — immediately | Prolong latency, prevent ascending infection |
| Dexamethasone (Antenatal steroids) | 1st/concurrent | Fetal lung maturity (takes 48h to work) |
| Tocolytics | 2nd — only if contracting | Brief window to allow steroids to act; no proven long-term benefit |
| Magnesium sulfate | Concurrent (if <32 wks) | Neuroprotection |
Why the MCQ Answer is (a) "Give tocolytics and dexamethasone"
For an exam question at 32 weeks with no signs of infection, the emphasis is on preserving the fetus with corticosteroids for lung maturity + tocolysis to delay delivery long enough for steroids to work. The "most appropriate" single-best answer collapses the protocol into the two most visible interventions. In actual clinical practice, antibiotics are given first or simultaneously — they are not optional.
The Previous Question (2014 Nov Q09) — Management of Preterm Labour at 32 Weeks with Intact Membranes
Answers b (Dexamethasone injections) and e (Oral erythromycin 250 mg six-hourly) are both correct here:
- Dexamethasone → fetal lung maturity
- Oral erythromycin → in PPROM, this is part of the NICHD antibiotic protocol
Sources: Creasy & Resnik's Maternal-Fetal Medicine, pp. 924–928; Morgan & Mikhail's Clinical Anesthesiology, p. 1641
In this 32 mcq membrane ruptured 3 hr before so more prone to ascending infection why still we priotize the dexamethasone
This is an excellent and sharp clinical question. Let me give you the precise reasoning.
Why Dexamethasone is Still Prioritized at 32 Weeks PPROM (Even with Ruptured Membranes)
The Core Logic: "Infection Risk" ≠ "Infection Present"
At 3 hours of membrane rupture:
- There is no fever, no tachycardia, no uterine tenderness
- This means chorioamnionitis has not yet developed
- The membranes just ruptured — ascending infection takes time to establish
The question is asking: what do you do in the window before infection sets in?
The 48-Hour Window is the Key
Dexamethasone takes 48 hours to produce maximum benefit on fetal lung maturity. At 32 weeks:
- Surfactant production is still immature
- RDS (Respiratory Distress Syndrome) is a near-certain morbidity if you deliver now
- Those 48 hours of steroid benefit can dramatically reduce RDS, IVH (intraventricular hemorrhage), NEC, and neonatal death
The logic is a calculated trade-off:
| Risk of waiting 48h | Benefit of waiting 48h |
|---|---|
| Ascending infection may develop | Fetal lungs mature → less RDS |
| Managed by: starting antibiotics immediately | Lifelong benefit to the baby |
This is why antibiotics + dexamethasone are given together — the antibiotics cover the infection risk while dexamethasone does its job.
Antibiotics Are Not Being Ignored
The correct management at 32 weeks PPROM is:
Antibiotics + Dexamethasone simultaneously — neither is skipped.
Antibiotics (ampicillin + erythromycin, NICHD protocol) are started at the same time as dexamethasone. They:
- Reduce bacterial colonisation of the amniotic fluid
- Prolong latency
- Protect against the very ascending infection you are worried about
So dexamethasone is not prioritised instead of antibiotics — it is prioritised alongside them.
When Dexamethasone Becomes Irrelevant
If the patient had:
- Fever ≥38°C
- Uterine tenderness
- Fetal or maternal tachycardia
...then chorioamnionitis is established, and the priority shifts entirely to deliver + broad-spectrum antibiotics. Dexamethasone at that point is secondary and cannot delay delivery (as in Question 25 from your previous image).
The Rule in Simple Terms
| Clinical State | Priority |
|---|---|
| PPROM, no infection signs, <34 weeks | Antibiotics + Dexamethasone together; tocolysis briefly if contracting |
| PPROM, infection signs present (fever, tenderness, tachycardia) | Expedite delivery + Broad-spectrum antibiotics; dexamethasone is secondary |
The reason dexamethasone is prioritised in Q32 is that 3 hours of ruptured membranes with no clinical infection signs means you are still in the "safe window" to gain fetal lung maturity benefit — and antibiotics running concurrently protect against the ascending infection risk during that window.
This is a shared conversation. Sign in to Orris to start your own chat.