Hodgkin lymphoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Hodgkin lymphoma"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive information to compile a thorough answer. Let me deliver it.
Hodgkin Lymphoma
Definition and Overview
Hodgkin lymphoma (HL) is a B-cell lymphoid neoplasm defined by the presence of distinctive neoplastic giant cells - Reed-Sternberg (RS) cells - in a background of reactive inflammatory cells. It differs from non-Hodgkin lymphoma (NHL) in several key respects: it arises in a single lymph node or chain of nodes, spreads in a stepwise fashion to anatomically contiguous lymphoid tissues, and is curable in the majority of cases. It accounts for ~0.7% of all new cancers in the US, with approximately 9,000 new cases per year.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 573
- Goldman-Cecil Medicine, Chapter 172
Epidemiology
- Age distribution: Bimodal - an early peak in young adults (25-30 years) and a second peak in adults >55 years
- Sex: Slightly more common in men
- Race: More frequent in Whites than Blacks; much less frequent in Asian populations
- Incidence: ~2.7 per 100,000 per year in North America; approximately 30,000 new cases annually in North America and Europe combined
- Geography: Highest rates in the US, Canada, Switzerland, and northern Europe; much lower rates in eastern Asia
- In developing countries (e.g., Indian subcontinent), the age distribution shifts strongly into childhood
Classification (WHO)
Five subtypes are recognized, the first four grouped as Classic Hodgkin Lymphoma (cHL):
| Subtype | Frequency |
|---|---|
| Nodular sclerosis | ~60% |
| Mixed cellularity | ~9% |
| Lymphocyte rich | ~3% |
| Lymphocyte depleted | ~1% |
| Nodular lymphocyte-predominant HL (NLPHL) | ~8% |
| HL, not otherwise classifiable | ~19% |
- Goldman-Cecil Medicine, Table 172-1
Note: In the 2022 International Consensus Classification (ICC), nodular lymphocyte-predominant HL has been renamed "nodular lymphocyte-predominant B-cell lymphoma", dropping the Hodgkin designation entirely, because its RS cells carry a germinal center B-cell immunophenotype distinct from classic HL.
Pathogenesis
Cell of Origin
Elegant single-cell microdissection studies revealed that RS cells in classic HL carry clonal IGH gene rearrangements with the hallmarks of somatic hypermutation, establishing their origin as germinal center or post-germinal center B cells. Despite this B-cell origin, RS cells paradoxically fail to express most B-cell-specific genes (including immunoglobulin), due to widespread epigenetic reprogramming.
NF-κB Activation
Activation of NF-κB is the central oncogenic event, promoting RS cell growth and survival via several mechanisms:
- EBV+ tumors: The viral protein LMP-1 directly signals NF-κB upregulation
- EBV- tumors: Acquired loss-of-function mutations in IκB or TNF-α-induced protein 3 (both NF-κB inhibitors)
- Copy number gains in the REL proto-oncogene (chromosome 2p) also boost NF-κB activity
EBV Association
- EBV is present in RS cells in ~50% of classic HL cases overall (up to 70% in mixed-cellularity subtype)
- The integration site of EBV is identical in all RS cells in a given case, indicating infection preceded clonal expansion
- A history of infectious mononucleosis triples the lifetime risk of subsequent HL
Immune Evasion
RS cells escape immune destruction by:
- Loss of β2-microglobulin → failure to express class I MHC molecules → invisible to cytotoxic T cells
- High expression of PD-L1 and PD-L2 (from chromosome 9p copy number gains) - immune checkpoint ligands that suppress T-cell responses
Inflammatory Microenvironment
RS cells secrete multiple cytokines that recruit a reactive infiltrate (which paradoxically supports tumor survival):
- IL-5 → attracts eosinophils
- TGF-β → promotes fibrosis (nodular sclerosis subtype)
- IL-13 → may drive RS cell growth via autocrine loop
- IL-10, M-CSF, eotaxin → additional microenvironment modulation
The RS cells comprise only ~1-10% of total tumor cellularity; the remainder is reactive lymphocytes, macrophages, eosinophils, plasma cells, and fibroblasts.
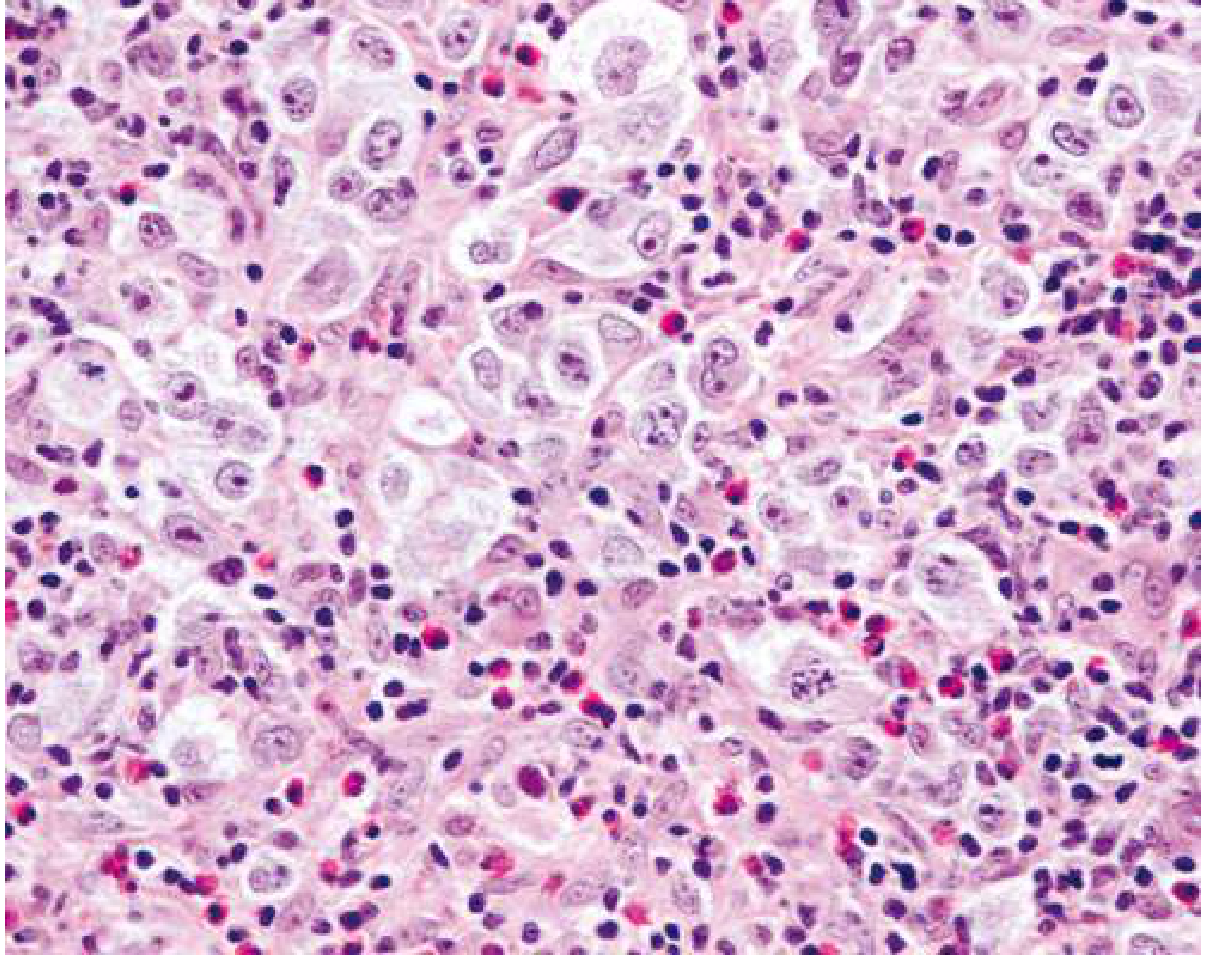
Morphology
Reed-Sternberg Cell (Diagnostic)
The classic RS cell is large (~45 μm in diameter) with:
- Multiple nuclei (or a single nucleus with multiple lobes)
- Large "owl-eye" nucleoli (~5-7 μm, the size of a small lymphocyte)
- Abundant pale cytoplasm
Histology of nodular sclerosing HL showing lacunar RS cells in a background of lymphocytes and eosinophils:
RS Cell Variants
| Variant | Appearance | Associated Subtype |
|---|---|---|
| Mononuclear (Hodgkin cell) | Single nucleus with prominent nucleolus | Classic HL |
| Lacunar cell | Folded/multilobate nucleus, pale cytoplasm that retracts in formalin (sits in a "lacuna") | Nodular sclerosis |
| Mummified cell | Pyknotic, shrunken cell death variant | Classic HL |
| Lymphohistiocytic (L&H / "popcorn cell") | Polypoid/multilobate nucleus, inconspicuous nucleolus | Nodular lymphocyte predominant |
Subtype Characteristics
1. Nodular Sclerosis (~60%): Most common; predominates in young women; mediastinal involvement typical; collagen bands divide tissue into nodules; lacunar cells present; birefringent collagen on polarized light
2. Mixed Cellularity (~9%): Classic RS cells in pleomorphic background; EBV+ in up to 70%; more common in males, older patients, HIV+ patients; intermediate prognosis
3. Lymphocyte Rich (~3%): Abundant small lymphocytes; few RS cells; excellent prognosis
4. Lymphocyte Depleted (~1%): Numerous RS cells, scant lymphocytes; most aggressive subtype; associated with HIV and older age
5. Nodular Lymphocyte Predominant (~8%): "Popcorn cells" (L&H cells) in a nodular background of B cells and follicular dendritic cells; distinct immunophenotype; rarely transforms to diffuse large B-cell lymphoma
Immunophenotype
| Marker | Classic HL | Nodular LP HL |
|---|---|---|
| CD30 | + (90-100%) | - |
| CD15 | + (75-85%) | - |
| PAX5/BSAP | + (dim, >90%) | + (strong) |
| CD20 | +/- (weak, ~40%) | ++ (strong) |
| CD79a | - | + |
| CD45 (LCA) | - | + |
| EBV (LMP-1) | + in ~50% of cHL | - |
This profile distinguishes HL from anaplastic large cell lymphoma (CD30+, CD15-, CD20-) and T-cell/histiocyte-rich B-cell lymphoma (resembles NLPHL but CD30-, IgD+ mantle cells present).
Clinical Features
Typical presentation:
- Painless cervical or supraclavicular lymphadenopathy (most common)
- Mediastinal adenopathy with or without cough/dyspnea (~60% have mediastinal involvement)
- Hepatosplenomegaly in advanced disease
B symptoms (present in ~30%, indicate worse prognosis):
- Unexplained fever >38°C (recurrent)
- Drenching night sweats
- Unexplained weight loss >10% body weight in 6 months
Alcohol-induced pain in involved lymph nodes - rare but pathognomonic
Pel-Ebstein fever: cyclical fever pattern (less common)
Staging - Modified Ann Arbor System (Cotswold Modification)
| Stage | Involvement |
|---|---|
| I | Single lymph node region (I) or one extralymphatic site (IE) |
| II | Two or more lymph node regions, same side of diaphragm (II), or local extralymphatic extension + lymph nodes, same side (IIE) |
| III | Lymph node regions on both sides of the diaphragm (III) ± local extranodal extension |
| IV | Diffuse involvement of one or more extralymphatic organs (bone marrow, liver, lung, bone) |
- Suffix A = no B symptoms; suffix B = B symptoms present
- Suffix X = bulky disease (largest diameter ≥10 cm)
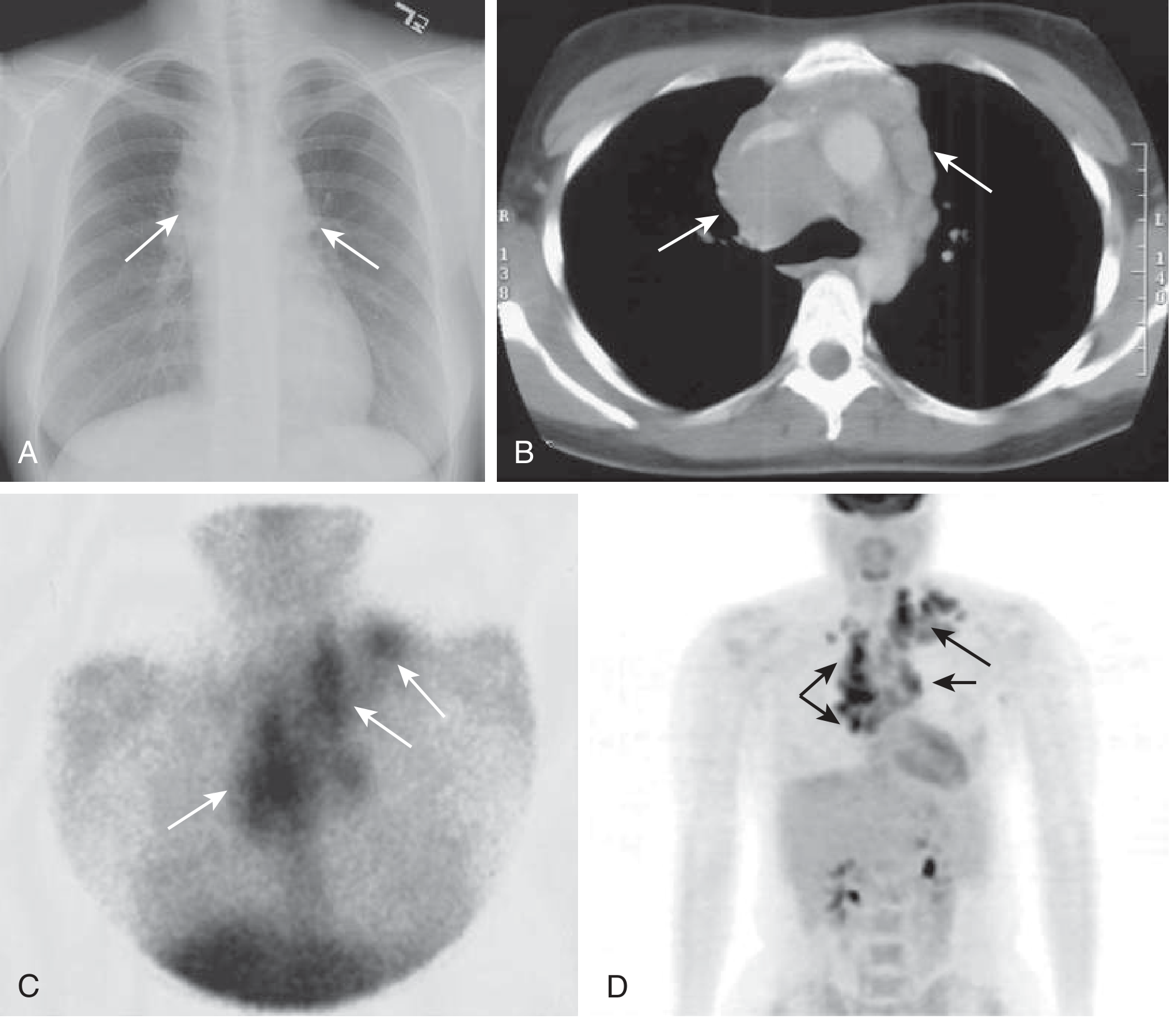
Staging Workup
- Complete history (B symptoms) + physical exam
- CBC, LDH, ESR, creatinine, alkaline phosphatase, albumin, serum protein electrophoresis
- Contrast-enhanced CT of neck, thorax, abdomen, pelvis
- FDG-PET/CT - now mandatory; replaces need for bone marrow biopsy in most cases
- Excisional lymph node biopsy for diagnosis
Treatment
Treatment is stratified by stage:
Limited Stage (IA or IIA, non-bulky)
- Standard: ABVD x 2 cycles + involved-region radiotherapy (IRRT)
- Alternative: ABVD x 3 cycles alone - if PET scan shows complete metabolic response, no further treatment; if partial response, add IRRT or checkpoint inhibitor x 8 doses + AVD x 4
- For unfavorable limited-stage (bulky mediastinum, extranodal extension, elevated ESR, ≥3 nodal areas): checkpoint inhibitors (nivolumab or pembrolizumab) combined with AVD showing >98% PFS in trials
Advanced Stage (IB, IIB, III, IV, or any stage with bulky disease)
- ABVD x 6 cycles (long-standing standard)
- A+AVD x 6 cycles (brentuximab vedotin + doxorubicin + vinblastine + dacarbazine) - preferred in many centers; omits bleomycin (reduces pulmonary toxicity)
- Escalated BEACOPP x 4-6 cycles (bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, prednisone) - higher response rate but more toxicity
Regimen Summary
| Regimen | Drugs |
|---|---|
| ABVD | Adriamycin (doxorubicin) + Bleomycin + Vinblastine + Dacarbazine |
| A+AVD | Brentuximab vedotin + Doxorubicin + Vinblastine + Dacarbazine |
| BEACOPP | Bleomycin + Etoposide + Adriamycin + Cyclophosphamide + Oncovin + Procarbazine + Prednisone |
Relapsed/Refractory Disease
- Second-line chemotherapy (e.g., ICE, DHAP)
- Followed by high-dose chemoradiation + autologous hematopoietic cell transplantation (auto-HCT)
- Brentuximab vedotin (anti-CD30 antibody-drug conjugate) - active in relapsed cHL
- Checkpoint inhibitors: Nivolumab and pembrolizumab have shown significant activity in relapsed/refractory HL, exploiting the tumor's high PD-L1/L2 expression
Prognosis
Hodgkin lymphoma was the first human cancer to be successfully treated with radiation therapy and chemotherapy, and remains one of the most curable cancers:
- Early stage: ~90-95% cure rate
- Advanced stage: ~75-85% long-term disease-free survival
- The major clinical challenge today is minimizing long-term treatment toxicity (secondary malignancies, cardiac disease, pulmonary fibrosis from bleomycin) while maintaining cure rates
Adverse prognostic features for advanced disease (IPS - International Prognostic Score):
Albumin <4 g/dL, Hemoglobin <10.5 g/dL, Male sex, Stage IV, Age ≥45, WBC ≥15,000/μL, Lymphocyte count <600/μL or <8% of WBC - each factor subtracts ~7% from 5-year freedom from progression.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine, Chapter 172 (Connors & Savage); Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.