
Complaint of chest pain
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed to give a comprehensive analysis.
ECG Analysis — 55-year-old Male, Chest Pain
Patient Details (from ECG strip)
- Age/Sex: 55 years, Male
- Heart Rate: 75 bpm
- QRS duration: 350/390 ms (likely a machine printing artifact — clinically the QRS appears normal width)
- QTc: 196 ms (machine value)
- PR interval: 110 ms
- RR interval: 800 ms
- P-R-T axes: 55 / 18 / 31
- Date: 19-Apr-2026, 15:42:34
ECG Findings
| Lead Group | Finding |
|---|---|
| V1–V4 | ST-segment elevation — convex/tombstone morphology |
| V5–V6 | ST elevation extending laterally |
| I, aVL | ST elevation (lateral extension) |
| II, III, aVF | Reciprocal ST depression |
| aVR | ST depression |
Rhythm: Sinus rhythm, rate ~75 bpm
Interpretation
Acute Anterolateral STEMI (ST-Elevation Myocardial Infarction)
ST elevation in V1–V6, I, and aVL with reciprocal ST depression in II, III, and aVF is the classic pattern of an anterolateral STEMI, indicating occlusion of the Left Anterior Descending (LAD) artery, likely proximal — possibly the left main given the widespread territory involved.
The treating physician has already prescribed:
- Aspirin 325 mg
- Clopidogrel (loading dose)
- Ondansetron (anti-emetic)
- Atorvastatin
This is consistent with standard STEMI initial management.
Reference ECG for Comparison
Below is a textbook anterior wall STEMI for comparison — note the identical pattern of ST elevation in V1–V4:
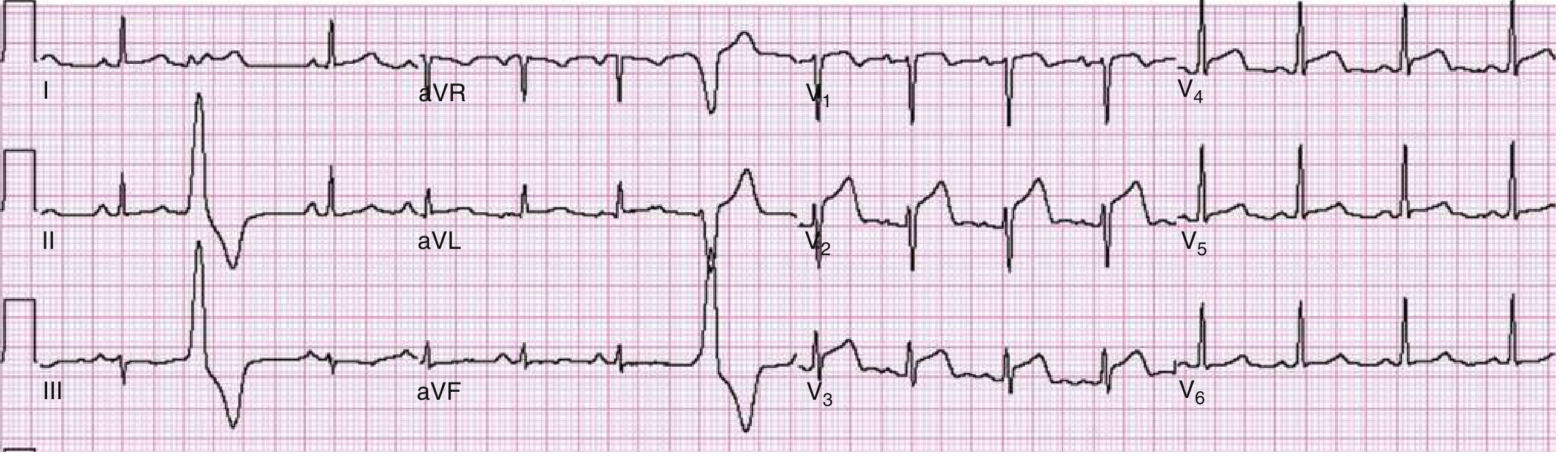
Fig. — Anterior wall acute STEMI. ST elevation in V1–V4, obliquely straight morphology, caused by 90% LAD stenosis. — Rosen's Emergency Medicine, p. 1003
Immediate Management (Time-Critical)
Per Rosen's Emergency Medicine and Tintinalli's Emergency Medicine:
1. Reperfusion — this is the priority:
- Primary PCI is the preferred reperfusion strategy — target door-to-balloon time ≤ 90 minutes
- If PCI is not available within 120 minutes → Fibrinolysis (e.g., tenecteplase/streptokinase) — target door-to-needle ≤ 30 minutes
2. Antiplatelet therapy (already initiated):
- Aspirin 325 mg loading ✓
- Clopidogrel 300–600 mg loading ✓ (Ticagrelor 180 mg preferred if available)
3. Anticoagulation:
- Heparin (UFH) 60 U/kg IV bolus + infusion, OR
- Enoxaparin 1 mg/kg SC
4. Other medications:
- Nitrates (sublingual/IV) — if BP allows, for pain relief
- Beta-blocker (oral, e.g., metoprolol) — if no contraindications (no bradycardia, hypotension, or acute LV failure)
- Statin (Atorvastatin already prescribed) ✓
- Morphine/fentanyl — for ongoing pain if needed (use judiciously)
- Ondansetron for nausea ✓
5. Monitoring:
- Continuous cardiac monitoring (risk of VF/VT)
- IV access × 2
- Oxygen only if SpO₂ < 90%
- Serial ECGs
6. Urgent cardiology referral / transfer to cath lab
⚠️ Red Flags on This ECG
- Widespread ST elevation (V1–V6 + I + aVL) suggests proximal LAD or left main occlusion — large territory at risk, high mortality
- This patient needs emergent cath lab activation now
This is a time-critical cardiac emergency. Every minute of delay = myocardial cell death ("time is muscle").
This is a shared conversation. Sign in to Orris to start your own chat.