How to treat herpes simplex 2 viral infection with henital lesions
Reading File
Finding Sources
Finding Sources
Searching PubMed
"herpes simplex" AND "genital" AND "treatment"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, well-sourced information to provide a complete answer. Let me compile it.
Treatment of Herpes Simplex Virus Type 2 (HSV-2) Genital Infection
Overview
HSV-2 is the predominant cause of genital herpes, a sexually transmitted infection characterized by recurrent painful vesicular ulcers in the genital area. Primary (first) infection is typically more severe than recurrences. Antiviral therapy does not eradicate the latent virus but significantly reduces symptom duration, lesion healing time, viral shedding, and recurrence frequency.
Mechanism of Action of Antivirals
All three first-line agents (acyclovir, valacyclovir, famciclovir) work by the same fundamental mechanism:
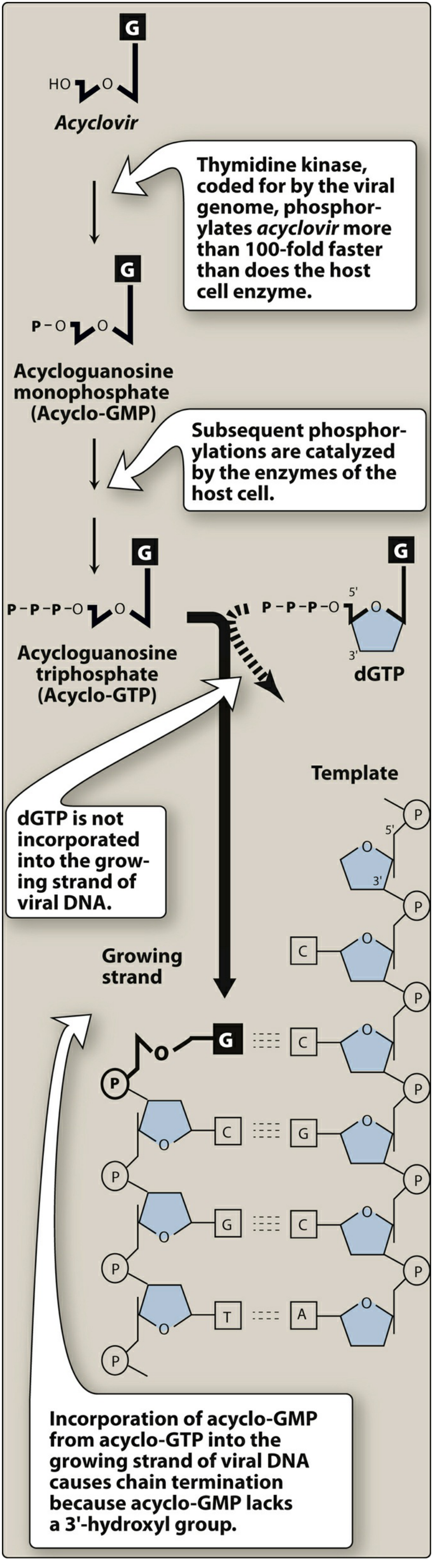
- The drug (a guanosine analogue) enters HSV-infected cells and is phosphorylated to its monophosphate form by viral thymidine kinase (100-fold faster than host cell enzymes - so it is highly selective).
- Host cell kinases further phosphorylate it to the triphosphate form.
- Acyclo-GTP competes with deoxyguanosine triphosphate (dGTP) as substrate for viral DNA polymerase and is incorporated into the growing DNA strand, causing premature chain termination (because acyclo-GMP lacks a 3'-hydroxyl group).
- Lippincott Illustrated Reviews: Pharmacology, p. 1122-1123
Treatment Regimens
1. First Episode / Primary Genital Herpes
This is typically the most severe presentation and warrants the longest treatment course:
| Drug | Dose | Duration |
|---|---|---|
| Acyclovir | 400 mg orally 3x/day or 200 mg 5x/day | 7-10 days |
| Valacyclovir | 1 g orally twice daily | 7-10 days |
| Famciclovir | 250 mg orally 3x/day | 7-10 days |
Treatment should continue until symptoms and lesions resolve. Compared to placebo, acyclovir reduces healing time from 16 to 12 days, duration of pain from 7 to 5 days, and constitutional symptoms from 6 to 3 days.
- Fitzpatrick's Dermatology, p. 3059
- Harrison's Principles of Internal Medicine 22E, Table 196-1
For severely ill or immunocompromised patients: IV acyclovir 5-10 mg/kg every 8 hours.
2. Recurrent Episodes - Episodic Therapy
Initiated at the first sign of prodrome (tingling, itching) or lesion onset. Most effective when started within 24-48 hours:
| Drug | Dose | Duration |
|---|---|---|
| Acyclovir | 800 mg orally twice daily | 5 days |
| Valacyclovir | 1 g once daily for 5 days or 500 mg twice daily for 3 days | 3-5 days |
| Famciclovir | 1 g once daily for 1 day | 1 day |
- Goldman-Cecil Medicine, p. 3607
- Harrison's Principles of Internal Medicine 22E
3. Suppressive (Long-Term) Therapy
Recommended for patients with 6 or more recurrences per year, or in patients who want to reduce transmission risk to susceptible partners. Suppressive therapy is highly effective at reducing both symptomatic recurrences and asymptomatic viral shedding:
| Drug | Dose |
|---|---|
| Acyclovir | 400 mg orally twice daily |
| Valacyclovir | 500 mg - 1 g orally once daily |
| Famciclovir | 250 mg orally twice daily |
Valacyclovir at 500 mg once daily is also specifically FDA-approved to reduce HSV-2 transmission to uninfected partners (reduces transmission by ~50% when combined with condoms).
- Goldman-Cecil Medicine, p. 3607
- Fitzpatrick's Dermatology, p. 3060
Drug Comparison: Why Valacyclovir is Preferred
Valacyclovir is the L-valyl ester prodrug of acyclovir. It achieves 3-5 times higher oral bioavailability than acyclovir, producing plasma levels comparable to IV acyclovir. This allows for less frequent dosing (once or twice daily vs. 3-5x daily for acyclovir), which greatly improves adherence.
Famciclovir (prodrug of penciclovir) has a comparable efficacy profile and similar adverse effects (headache, nausea, diarrhea). It has a very long intracellular half-life.
- Fitzpatrick's Dermatology, p. 3059
Special Populations
Pregnancy
- Acyclovir and valacyclovir are both used in pregnancy and are considered safe.
- Women with primary HSV infection during pregnancy should be treated with antiviral therapy.
- Women at or beyond 36 weeks gestation with a history of recurrent genital herpes should receive suppressive therapy - this reduces viral shedding at delivery, active lesions near term, and the need for cesarean section.
- Active genital lesions at delivery are an indication for cesarean section to prevent neonatal HSV.
- Fitzpatrick's Dermatology, p. 3059; Creasy & Resnik's Maternal-Fetal Medicine
Immunocompromised Patients
- Higher risk of severe, disseminated infection and acyclovir-resistant HSV.
- Resistance typically arises from mutations in viral thymidine kinase, causing cross-resistance to valacyclovir and famciclovir.
- Resistant strains are treated with IV foscarnet or, less commonly, IV cidofovir.
- Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine, p. 3606
Renal Impairment
- Both acyclovir and valacyclovir are renally excreted (glomerular filtration and tubular secretion). Dose reduction required with reduced GFR.
- IV acyclovir can cause reversible renal tubular crystallization - ensure adequate hydration.
- Lippincott Illustrated Reviews: Pharmacology, p. 1123
Topical Therapy
Topical acyclovir is much less effective than oral therapy and is generally not recommended for genital herpes. Its efficacy for genital lesions is minimal. Oral antivirals are strongly preferred.
- Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E
Counseling Points
-
Asymptomatic shedding is responsible for most transmission - patients should be informed even when no visible lesions are present.
-
Patients should abstain from sexual contact during outbreaks and use condoms between outbreaks (condoms reduce but do not eliminate transmission risk).
-
Antivirals do not cure HSV-2; the virus establishes latency in sacral dorsal root ganglia permanently.
-
Recurrence is common; frequency tends to decrease over years.
-
All patients with symptomatic genital HSV recurrences should be considered candidates for long-term suppressive therapy.
-
Swanson's Family Medicine Review; Fitzpatrick's Dermatology, p. 3059
Summary Table
| Scenario | First Choice | Alternative |
|---|---|---|
| First episode | Valacyclovir 1g PO BID x 10d | Acyclovir 400mg PO TID x 10d |
| Recurrence - episodic | Valacyclovir 1g PO OD x 5d | Famciclovir 1g PO once |
| Suppression | Valacyclovir 500mg PO OD | Acyclovir 400mg PO BID |
| Severe / hospitalized | IV Acyclovir 5-10mg/kg q8h | - |
| Acyclovir-resistant | IV Foscarnet | IV Cidofovir |
This is a shared conversation. Sign in to Orris to start your own chat.