Definitive treatment for ibs
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Definitive Treatment of IBS
IBS has no single curative treatment — management is tailored to the predominant symptom pattern (IBS-C, IBS-D, or mixed) and includes lifestyle, dietary, pharmacological, and psychological interventions.
1. General / Non-pharmacological
- Diet modifications: Low-FODMAP diet is the most evidence-based dietary intervention. Avoiding gas-producing foods, caffeine, and alcohol is helpful.
- Psychosocial modifications: Cognitive-behavioural therapy (CBT), gut-directed hypnotherapy, and mindfulness-based therapies have demonstrated efficacy, particularly in refractory cases.
- Exercise: Regular physical activity improves overall GI motility.
2. Pharmacological Treatment (by subtype)
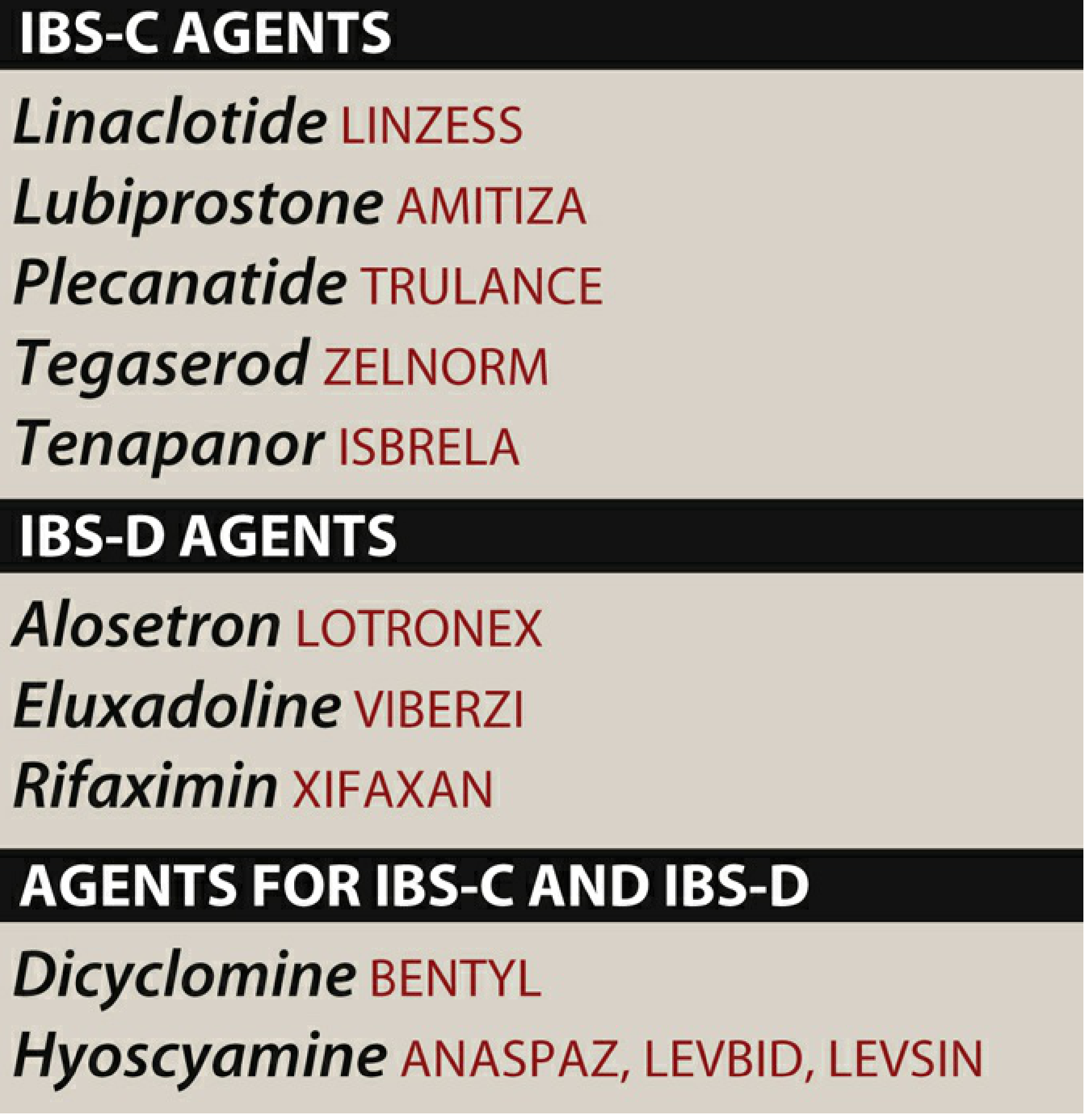
IBS-C (Constipation-predominant)
| Drug | Class | Mechanism | Key Notes |
|---|---|---|---|
| Linaclotide (Linzess) | Guanylate cyclase-C agonist | ↑ intestinal fluid secretion, ↓ visceral pain | First-line; avoid in GI obstruction |
| Plecanatide (Trulance) | Guanylate cyclase-C agonist | Same as linaclotide | Also approved for chronic idiopathic constipation |
| Lubiprostone (Amitiza) | Chloride channel activator | ↑ intestinal fluid secretion | Approved for women with IBS-C; no tolerance/dependence |
| Tegaserod (Zelnorm) | 5-HT₄ partial agonist | Prokinetic | Restricted use; risk of MI/stroke |
| Tenapanor (Isbrela) | NHE3 inhibitor | ↓ Na⁺ absorption → ↑ luminal fluid | Newer agent |
IBS-D (Diarrhea-predominant)
| Drug | Class | Mechanism | Key Notes |
|---|---|---|---|
| Alosetron (Lotronex) | 5-HT₃ antagonist (high potency) | ↓ smooth muscle activity in gut | Approved for severe IBS-D in women; risk of ischemic colitis — restricted prescribing program |
| Eluxadoline (Viberzi) | Mixed μ/κ-opioid agonist + δ-antagonist | ↓ intestinal motility and secretion | Contraindicated in absence of gallbladder (↑ pancreatitis risk) |
| Rifaximin (Xifaxan) | Non-absorbable antibiotic | Alters gut microbiome / treats SIBO component | 2-week course; can retreat |
Both IBS-C and IBS-D (Antispasmodics)
- Dicyclomine (Bentyl) — anticholinergic; reduces bowel spasm
- Hyoscyamine (Levsin) — anticholinergic; relieves cramping
3. Adjunct Pharmacotherapy
- Antidepressants: Low-dose TCAs (e.g., amitriptyline) for IBS-D (slow motility + central pain modulation); SSRIs for IBS-C (↑ motility) and comorbid anxiety/depression.
- Antidiarrheals: Loperamide for symptom control in IBS-D (does not improve pain).
- Soluble fibre (psyllium): Beneficial in IBS-C; insoluble fibre may worsen symptoms.
- Peppermint oil: Smooth muscle relaxant; reduces abdominal pain.
Key Point
IBS is a functional disorder — there is no curative single treatment. The goal is symptom control. Drug choice is driven by predominant bowel habit (C vs. D), severity, sex (some drugs are approved only for women), and individual response.
— Lippincott Illustrated Reviews: Pharmacology; Katzung's Basic and Clinical Pharmacology, 16th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.