Standard guidelines for hypertension
Reading File
Searching the Web
hypertension guidelines 2025 ACC AHA ESC treatment targets
Finding Sources
Searching PubMed
"hypertension" AND "guidelines" AND "treatment"
Finding Sources
Reading Article
PMID: 39210715
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from the textbooks, web sources, and PubMed. Let me compile the full response.
Standard Guidelines for Hypertension
1. Definitions and Classification
ACC/AHA 2025 (USA) - the most current guideline, replacing 2017
| Category | Systolic (mmHg) | Diastolic (mmHg) |
|---|---|---|
| Normal | < 120 | < 80 |
| Elevated BP | 120-129 | < 80 |
| Stage 1 Hypertension | 130-139 | 80-89 |
| Stage 2 Hypertension | ≥ 140 | ≥ 90 |
-
Both the 2017 and 2025 ACC/AHA guidelines retain ≥ 130/80 mmHg as the diagnostic threshold.
-
ESC 2024 uses a higher threshold: ≥ 140/90 mmHg for diagnosis (130-139/85-89 mmHg is "high normal," treated with lifestyle only).
-
Washington Manual of Medical Therapeutics, p. 74
-
Comprehensive Clinical Nephrology 7e, p. 530+
2. Initial Evaluation
History and exam should assess:
- Target organ damage: LVH, retinopathy, CKD, stroke/TIA history, PAD
- Secondary causes: renal artery stenosis, primary aldosteronism, obstructive sleep apnea, pheochromocytoma, Cushing syndrome
- Drug/substance contribution: cocaine, sympathomimetics, NSAIDs, OCPs, alcohol withdrawal, clonidine rebound
Baseline workup: Urinalysis, BMP (creatinine, potassium, glucose), fasting lipids, HbA1c, CBC (hematocrit), uric acid, ECG. Echocardiography if LVH suspected. Ambulatory BP monitoring (ABPM) for white-coat or masked hypertension - strongly emphasized in AHA 2025.
Cardiovascular risk stratification: The 2025 ACC/AHA guideline now uses the PREVENT Equation (replacing the old Pooled Cohort Equations) to guide pharmacotherapy decisions.
- Washington Manual of Medical Therapeutics, p. 75-78
3. Treatment Thresholds
| Guideline | Initiate Pharmacotherapy At |
|---|---|
| ACC/AHA 2025 | Stage 1 (≥130/80) + ASCVD or 10-yr CVD risk ≥7.5% (PREVENT); Stage 2 always |
| ACC/AHA 2025 | Stage 1, low-risk (<7.5%): lifestyle 3-6 months first, then add meds if not at goal |
| ESC 2024 | ≥140/90 mmHg; 130-139/80-89 mmHg only if high CV risk, after lifestyle trial |
4. Lifestyle Modifications
Recommended for all hypertensive patients regardless of pharmacotherapy:
| Modification | Approximate SBP Reduction |
|---|---|
| Weight reduction (per 10 kg loss) | 5-20 mmHg |
| DASH diet | 8-14 mmHg |
| Sodium restriction (< 2 g/day) | 2-8 mmHg |
| Aerobic exercise | 4-9 mmHg |
| Limit alcohol (≤ 2 drinks/day men, ≤ 1/day women) | 2-4 mmHg |
| Smoking cessation | Reduces overall CV risk |
- Washington Manual of Medical Therapeutics, Table 3-3
5. Pharmacotherapy
First-Line Agents (Grade I, Level A evidence)
- Thiazide/thiazide-like diuretics (chlorthalidone preferred over HCTZ for 24-hour coverage)
- Calcium channel blockers (CCBs) - especially dihydropyridines (amlodipine)
- ACE inhibitors (ACEi)
- Angiotensin receptor blockers (ARBs)
Beta-blockers are not first-line unless a specific indication exists (HFrEF, post-MI, angina, AF, or pregnancy in younger women).
- Comprehensive Clinical Nephrology 7e, Table 37.9
Combination Strategy
The 2025 ACC/AHA guideline (like ESC 2018/2024) strongly favors starting with dual combination therapy in most patients at typical targets, because single-drug response is often limited by compensatory pressor mechanisms (e.g., RAS activation countering diuretics/CCBs).
- Stage 1, lower-risk: Single agent with titration is reasonable (Grade IIa)
- Stage 2 (BP >20/10 above target): Two agents from different classes recommended upfront (Grade I), either as separate pills or a single-pill combination (SPC)
European algorithm (ESC/ESH):
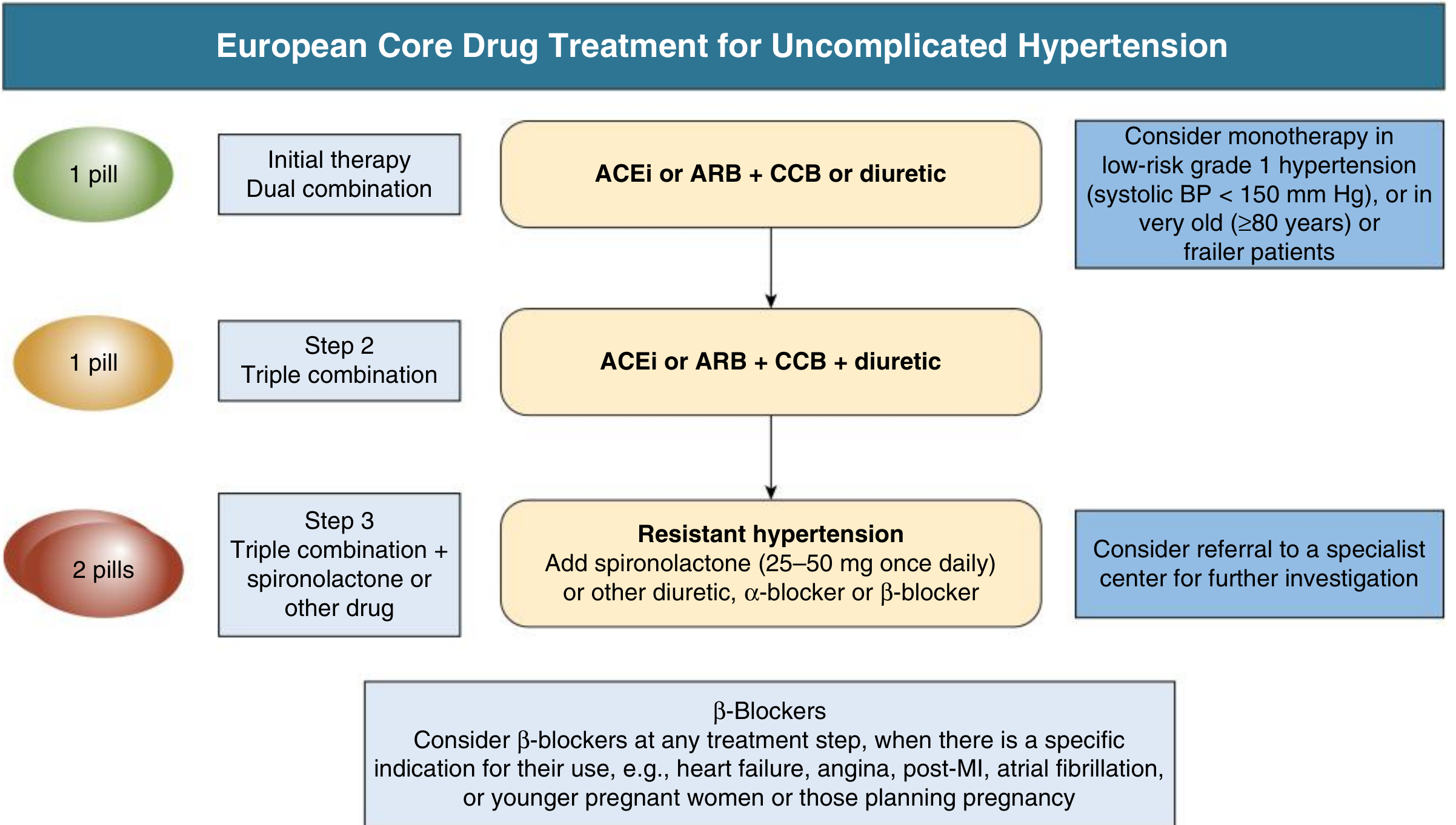
- Comprehensive Clinical Nephrology 7e, Fig. 37.3
6. Treatment Targets
| Population | Target BP |
|---|---|
| General adults (ACC/AHA 2025) | < 130/80 mmHg |
| Older/frail adults (individualized) | < 140 mmHg systolic |
| CKD with proteinuria | < 130/80 (some guidelines < 125/75) |
| Diabetes (ACC/AHA) | < 130/80 mmHg |
| Post-stroke / cognitive protection | < 130 mmHg systolic |
| ESC 2024 (age 18-64) | 120-129/70-79 mmHg |
| ESC/ESH 2024 (age 65-79) | 130-139 mmHg systolic |
| ESH 2024 (age ≥80 or frail) | 140-150 mmHg systolic |
The J-curve concern (excessive BP lowering causing harm) applies particularly at DBP < 60-65 mmHg in patients with CAD.
7. Special Populations and Compelling Indications
| Comorbidity | Preferred Agents |
|---|---|
| Diabetes | ACEi or ARB (especially if albuminuria present); SGLT2 inhibitors offer added BP-lowering + renoprotection |
| CKD with proteinuria | ACEi or ARB as first-line (renoprotective beyond BP effect) |
| Heart failure (HFrEF) | ACEi/ARB/ARNI + beta-blocker + aldosterone antagonist |
| Post-MI / stable angina | Beta-blocker + ACEi or ARB |
| Atrial fibrillation | Beta-blocker or non-DHP CCB for rate control |
| Isolated systolic hypertension (elderly) | Thiazide or long-acting DHP-CCB |
| Pregnancy | Labetalol, methyldopa, nifedipine (ACEi/ARBs are contraindicated) |
| Black patients | Thiazides and CCBs preferred (RAS blockers less effective as monotherapy) |
8. Resistant Hypertension
Defined as BP remaining above target despite ≥ 3 optimally dosed agents (including a diuretic), or requiring ≥ 4 agents to maintain control.
Steps:
- Confirm true resistance with ABPM/HBPM (exclude pseudo-resistance from poor adherence, white-coat effect, or suboptimal measurement)
- Screen for primary aldosteronism - now a Class 1 recommendation in all patients with resistant hypertension (AHA 2025, ESC 2024, Endocrine Society 2025)
- Evaluate for other secondary causes (renal artery stenosis, OSA, pheochromocytoma)
- Add spironolactone 25-50 mg/day as fourth agent (strongest evidence)
- Consider renal denervation (RDN) - newly incorporated in ACC/AHA 2025, ESC 2024, and ESH 2024 for carefully selected patients with eGFR ≥40 ml/min/1.73m² and uncontrolled BP despite optimal therapy
9. Hypertensive Emergency vs. Urgency
| Urgency | Emergency | |
|---|---|---|
| Definition | Severe BP elevation (≥ 180/100-120) without acute target organ damage | Severe BP + acute end-organ damage |
| Management | Oral antihypertensives; gradual reduction over 24-48 hours; no IV needed | IV agents (labetalol, nicardipine, nitroprusside, clevidipine); ICU admission |
| Target | Reduce by ~20-25% over first hours; normalize over days | Reduce MAP by ~25% in first hour, then gradual over 24-48 hours |
Note: The term "hypertensive urgency" has been retired in the 2025 ACC/AHA guidelines - replaced with "severe hypertension without acute target organ damage" to prevent over-treatment and unnecessary ED visits.
- Brenner and Rector's The Kidney 2-Volume Set; Harrison's Principles of Internal Medicine 22e
10. Monitoring
- Reassess BP in 1 month after pharmacotherapy initiation in high-risk patients; every 3-6 months once stable.
- Home BP monitoring (HBPM) and ABPM are more prominently recommended in AHA 2025 for better phenotyping and preventing over/under-treatment.
- Monitor potassium and creatinine after starting ACEi/ARB/diuretics.
Key Guideline Documents
| Guideline | Year | Threshold | Target |
|---|---|---|---|
| ACC/AHA 2025 | 2025 | ≥ 130/80 | < 130/80 |
| ESC 2024 | 2024 | ≥ 140/90 | 120-139 (age-dependent) |
| Hypertension Canada | 2025 | ≥ 130/80 | < 130/80 |
Note on ESC 2024 erratum: An erratum was issued (PMID: 41319970) - use the corrected version.
Sources:
- Washington Manual of Medical Therapeutics, pp. 74-78
- Comprehensive Clinical Nephrology 7e, pp. 530-531
- ACC/AHA 2025 High Blood Pressure Guideline (Circulation 2025)
- 2024 ESC Guidelines for hypertension - McEvoy JW et al., Eur Heart J. 2024 [PMID: 39210715]
- Hypertension Canada 2025 - Goupil R et al., CMAJ 2025 [PMID: 40419299]
This is a shared conversation. Sign in to Orris to start your own chat.