Auscultation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Excellent - rich content from multiple authoritative sources. I now have enough to write a comprehensive answer.
Auscultation
Auscultation is the clinical technique of listening to body sounds - typically with a stethoscope - to assess the function of the heart, lungs, blood vessels, and abdominal organs. It remains one of the most diagnostically powerful tools at the bedside.
The Stethoscope
The stethoscope has two key components, each suited to different sound frequencies:
- Diaphragm - detects higher-pitched sounds (normal breath sounds, S1, S2, aortic murmurs, pericardial rubs)
- Bell - detects lower-pitched sounds (S3, S4, mitral stenosis rumble). The bell must be applied very lightly to hear low-pitched sounds; pressing hard causes the underlying skin to act as a diaphragm and filters out low frequencies
Practical tips: always apply the stethoscope directly to skin (not clothing), use a warm chest piece, and ensure a quiet room. Stethoscope tubing degrades with prolonged skin contact and poor maintenance; glycerin-free isopropyl alcohol wipes are preferred for cleaning.
- Murray & Nadel's Textbook of Respiratory Medicine
Cardiac Auscultation
Auscultation Areas
The four classic areas are not directly over the valves; sounds travel along the direction of blood flow:
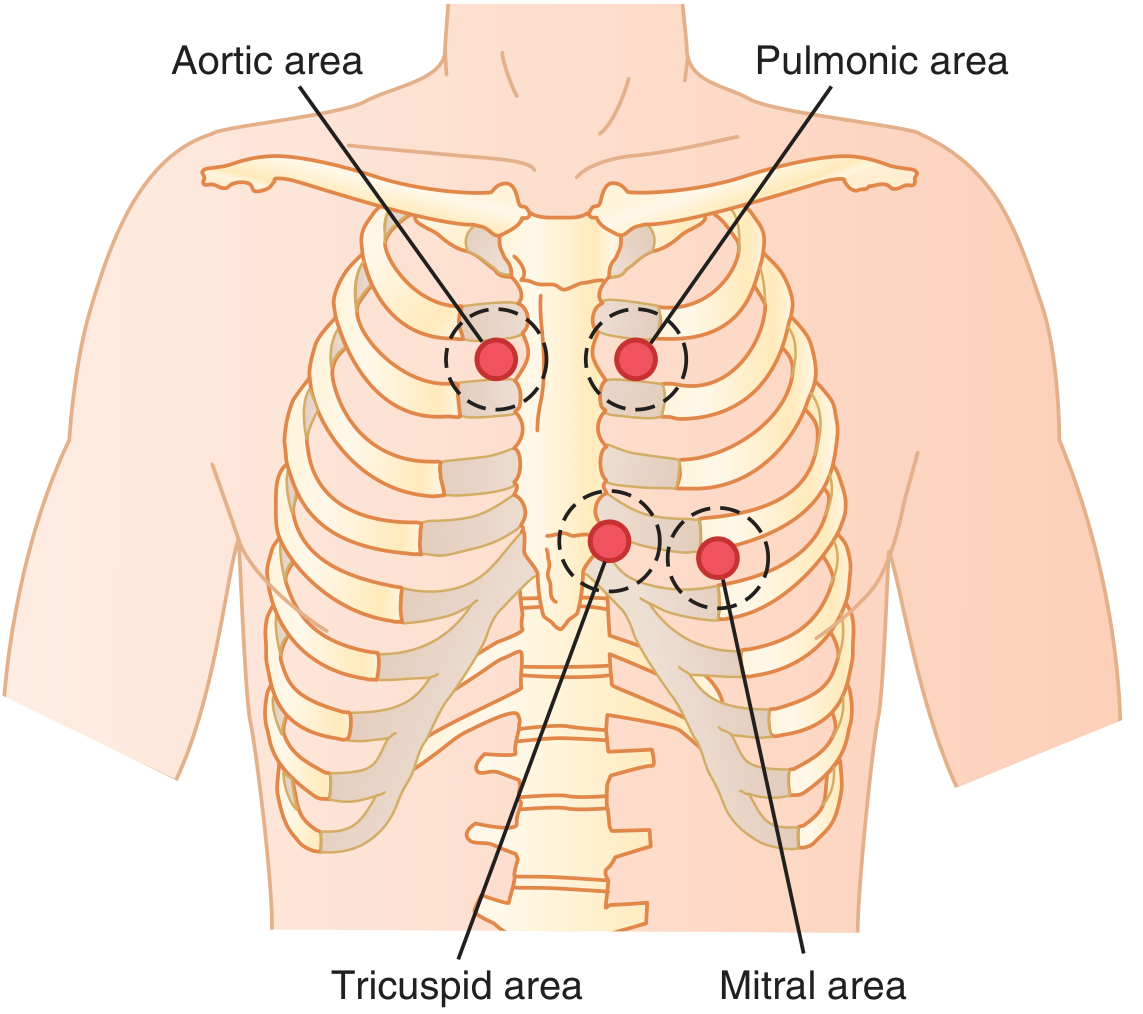
| Area | Location | Best For |
|---|---|---|
| Aortic | Right 2nd intercostal space, sternal border | Aortic stenosis/regurgitation |
| Pulmonic | Left 2nd intercostal space, sternal border | Pulmonic stenosis, P2 intensity |
| Tricuspid | Left 4th intercostal space, lower sternal border | Tricuspid valve disease, right-sided S3/S4 |
| Mitral (Apex) | Left 5th intercostal space, midclavicular line | Mitral stenosis/regurgitation, left-sided S3/S4 |
| Erb's Point | Left 3rd intercostal space | Nearly all heart sounds and murmurs can be heard here |
- Guyton and Hall Textbook of Medical Physiology; Color Atlas of Human Anatomy Vol. 2
Heart Sounds
S1 (First Heart Sound)
- Produced primarily by mitral valve closure, with a lesser contribution from tricuspid closure
- Louder in mitral stenosis (with mobile leaflets) and high-output states
- Softer in mitral regurgitation (poor coaptation) and cardiomyopathy
S2 (Second Heart Sound)
- Produced by aortic valve closure (A2) followed by pulmonic closure (P2)
- During expiration: A2 and P2 are nearly superimposed
- During inspiration: Increased RV stroke volume delays P2, producing physiological splitting
- Fixed splitting: atrial septal defect, right bundle branch block
- Paradoxical (reversed) splitting: left bundle branch block, severe aortic stenosis (A2 comes after P2)
- Increased A2: systemic hypertension
- Decreased A2: aortic stenosis (especially severe/calcified)
- Increased P2: pulmonary hypertension
S3 (Third Heart Sound)
- Occurs during rapid ventricular filling in early diastole
- Normal in children and young adults; in adults >40 years, it is pathological
- Causes: mitral regurgitation (volume overload), advanced heart failure (elevated early diastolic pressure)
- Heard best with the bell at the apex (left ventricular S3) or left 4th ICS (right ventricular S3)
S4 (Fourth Heart Sound)
- Occurs during atrial contraction (late diastole), just before S1
- Reflects reduced ventricular compliance - the atrium contracts forcefully against a stiff ventricle
- Common with hypertension, LV hypertrophy, ischemic heart disease, heart failure
- Heard best with the bell
Added Sounds
| Sound | Timing | Heard Best | Causes |
|---|---|---|---|
| Ejection click | Early systole | Base | Congenital aortic stenosis (mobile valve), hypertension, high-output states |
| Mid/late systolic click | Mid-to-late systole | Apex | Mitral valve prolapse |
| Opening snap | Early diastole (after S2) | Apex/left 3rd-4th ICS | Mitral/tricuspid stenosis (mobile leaflets) |
| Pericardial rub | Any phase | Left sternal border | Pericarditis (scratchy, "leather-on-leather") |
Opening snap vs. S3: Opening snap is high-pitched (heard with diaphragm); S3 is low-pitched (heard with bell). The S2-OS interval is also typically shorter than S2-S3.
- Goldman-Cecil Medicine; Braunwald's Heart Disease
Heart Murmurs
Murmurs are graded on a 1-6 scale:
| Grade | Description |
|---|---|
| 1 | Faint; heard only with careful auscultation |
| 2 | Readily audible |
| 3 | Moderately loud; no thrill |
| 4 | Loud; palpable thrill |
| 5 | Very loud; audible with stethoscope partially off chest |
| 6 | Audible without the stethoscope |
Systolic Murmurs
| Murmur | Type | Best Heard | Radiation | Key Features |
|---|---|---|---|---|
| Aortic stenosis | Ejection (crescendo-decrescendo) | Aortic area | Carotids | Late-peaking; Gallavardin phenomenon (apex radiation mimics MR); decreases with Valsalva/standing, increases with squatting |
| Mitral regurgitation | Pansystolic | Apex | Axilla | Holosystolic; not affected by beat-to-beat variation |
| Tricuspid regurgitation | Pansystolic | Left sternal border | - | Increases with inspiration (Carvallo's sign) |
| HOCM | Ejection | Left sternal border | - | Increases with Valsalva/standing, decreases with squatting |
| Pulmonary stenosis | Ejection | Pulmonic area | - | Wide splitting of S2 |
Diastolic Murmurs (always pathological)
| Murmur | Type | Best Heard | Key Features |
|---|---|---|---|
| Aortic regurgitation | Early diastolic (decrescendo) | Left sternal border, sitting forward | High-pitched; heard with diaphragm |
| Mitral stenosis | Mid-diastolic rumble | Apex (bell) | Preceded by opening snap; low-pitched |
| Tricuspid stenosis | Mid-diastolic | Left 3rd-4th ICS |
Continuous Murmurs
- Patent ductus arteriosus (PDA): "machinery" murmur, heard under left clavicle, continuous through systole and diastole
Dynamic Auscultation (Maneuvers)
| Maneuver | Effect on Preload | Changes |
|---|---|---|
| Valsalva (strain phase) | Decreases | Most murmurs softer; HOCM louder; MVP click moves earlier |
| Standing | Decreases | Same as Valsalva |
| Squatting | Increases | Most murmurs louder; HOCM softer; MVP click moves later |
| Inspiration | Increases RV filling | Right-sided murmurs louder (Carvallo's sign) |
| Expiration | Increases LV filling | Left-sided murmurs louder |
- Braunwald's Heart Disease; Goldman-Cecil Medicine
Lung Auscultation
The American Thoracic Society standardized lung sound terminology:
| Sound | Characteristics | Significance |
|---|---|---|
| Normal (vesicular) | 200-600 Hz; soft, nonmusical; inspiratory > expiratory | Healthy lung parenchyma |
| Bronchial | Louder, hollow quality; expiratory ≥ inspiratory | Consolidation (e.g., pneumonia) |
| Crackles (fine) | Discontinuous, high-pitched "velcro-like" | Interstitial lung disease, early pulmonary edema |
| Crackles (coarse) | Discontinuous, lower-pitched, bubbling | Secretions, pneumonia, bronchiectasis |
| Wheezes | Continuous, musical, high-pitched | Airway narrowing (asthma, COPD, bronchospasm) |
| Rhonchi | Continuous, low-pitched, snoring | Large airway secretions; clear with coughing |
| Pleural friction rub | Superficial, leathery, creaking | Pleuritis |
| Stridor | High-pitched, inspiratory, heard without stethoscope | Upper airway obstruction |
Added value: Auscultation can detect pathology even when chest radiograph is normal (e.g., wheeze in asthma, crackles in early interstitial lung disease).
- Murray & Nadel's Textbook of Respiratory Medicine
Other Sites of Auscultation
- Abdomen: Bowel sounds (absent in ileus, hyperactive in early obstruction); bruits over aorta or renal arteries suggest stenosis
- Carotids: Bruits suggest stenosis (though absence does not exclude high-grade stenosis)
- Thyroid: Bruit over an enlarged gland suggests Graves' disease (hyperthyroidism)
- Peripheral vessels: Femoral bruits in peripheral arterial disease
Clinical Pearls
- A murmur of grade 3+ with a late peak strongly suggests severe aortic stenosis; however, a soft murmur does NOT exclude severe AS (the murmur softens when LV stroke volume falls)
- Diastolic murmurs are always pathological; systolic murmurs may be benign ("innocent" flow murmurs)
- Splitting of S2 helps exclude severe AS - normal splitting implies flexible, mobile aortic leaflets
- S3 after age 40 = heart failure until proven otherwise
- S4 reflects decreased ventricular compliance - think hypertension, LVH, or ischemia
- The Gallavardin phenomenon (AS murmur radiating to apex mimicking MR) is a classic auscultatory trap
This is a shared conversation. Sign in to Orris to start your own chat.