Cp angle mass lesion imaging
Reading File
Finding Sources
Finding Sources
Searching PubMed
cerebellopontine angle tumor MRI imaging diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive textbook data and images. Let me compile the complete answer.
Cerebellopontine Angle Mass Lesions - Imaging
Anatomy of the CPA
The CP angle is a CSF-filled subarachnoid cistern bounded:
- Anteriorly: CN VI and lateral clivus
- Laterally: medial surface of the petrous bone
- Medially: pons, middle cerebellar peduncle, ventral cerebellum
- Superiorly: CN V
- Inferiorly: CN IX, X, XI
- Posteriorly: cerebellar flocculus
CNs V, VII, VIII, IX, X, XI and the anterior inferior cerebellar artery (AICA) all traverse this space.
Classification of CPA Lesions
Common:
- Vestibular schwannoma (acoustic neuroma) - ~80-90%
- Meningioma - ~3-18%
- Epidermoid (primary cholesteatoma) - ~2.5%
- Facial nerve schwannoma - ~1%
- Paraganglioma - up to 10% when secondary tumors included
Less common: Arachnoid cyst, lipoma, hemangioma, choroid plexus papilloma, metastasis, ependymoma, brainstem glioma (extends into CPA via foramen of Luschka), petrous carotid aneurysm, meningeal carcinomatosis
Imaging Modality of Choice
Gadolinium-enhanced MRI is the gold standard. It can detect lesions as small as 1.5 mm. For screening purposes, heavily T2-weighted Fast Spin Echo (FSE) sequences are also highly accurate - schwannomas appear hypointense against bright CSF, showing as a filling defect in the IAC - comparable sensitivity to gadolinium-enhanced T1, at lower cost and without contrast risk.
CT still plays a role for assessing osseous changes (hyperostosis, IAC enlargement, erosion) and in patients who cannot undergo MRI.
Imaging Features of the Three Most Common CPA Lesions
(Cummings Otolaryngology, Table 179.2)
| Feature | Vestibular Schwannoma | Meningioma | Epidermoid |
|---|---|---|---|
| Location | Centered on IAC | Eccentric to IAC | Anterolateral/posterolateral to brainstem |
| Bone changes | Enlarges IAC (most) | Occasional hyperostosis | Occasional erosion |
| Shape | Spherical/ovoid; acute bone-tumor angle | Hemispherical, plaque-like; obtuse bone-tumor angle; may herniate through tentorium | Variable; "dumbbell" into middle fossa or contralateral CPA |
| CT density | Mostly isodense | Slightly hypodense; some calcified | Mostly hypodense; occasional peripheral Ca2+ |
| CT enhancement | Moderate-marked; inhomogeneous | Marked and homogeneous | Non-enhancing |
| T1 MRI | Isointense or hypointense | Isointense or hypointense | Hypointense |
| T2 MRI | Isointense or hypointense | Variable | Hyperintense |
| Gadolinium | Marked enhancement | Moderate enhancement | Non-enhancing |
| DWI | Facilitated diffusion | Facilitated diffusion | Restricted diffusion (bright) - key distinguisher |
Imaging Details by Lesion Type
1. Vestibular Schwannoma (Acoustic Neuroma)
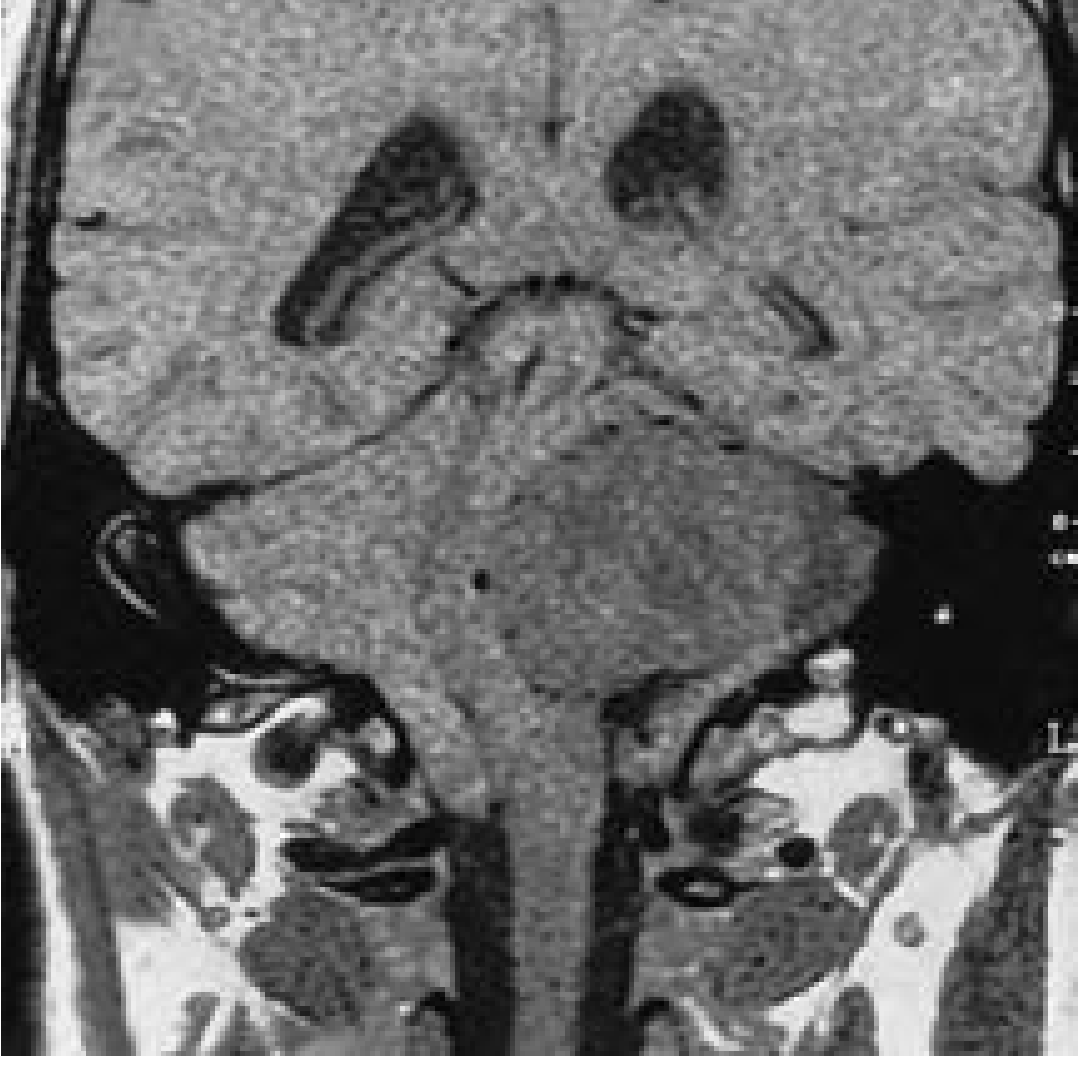
Large acoustic neuroma causing hydrocephalus, brainstem shift, and cerebellar tonsillar herniation - non-contrast coronal T1 MRI
- MRI T1: isointense or mildly hypointense to brain
- MRI T2: mildly hyperintense to brain; tumor appears as a filling defect (hypointense void) against bright CSF on FSE T2
- Gadolinium T1: marked, often inhomogeneous enhancement
- CT: ovoid lesion centered on IAC; moderate enhancement; ~85% show acute angles at bone-tumor interface
- Key sign: enlargement of the IAC on CT (most cases)
- Cystic variants: central areas of low T1 signal, increased T2 signal compared to solid tumors (see image below)
- "Fundal cap" sign: CSF visible lateral to the tumor in IAC on T2 = tumor not impacting fundus; absence of fundal cap = fundal involvement = poorer hearing prognosis
- 3D-FSE/CISS sequences: define nerve of origin and fundal involvement pre-operatively
- Intracanalicular tumors: detected as filling defects on T2-FSE without contrast
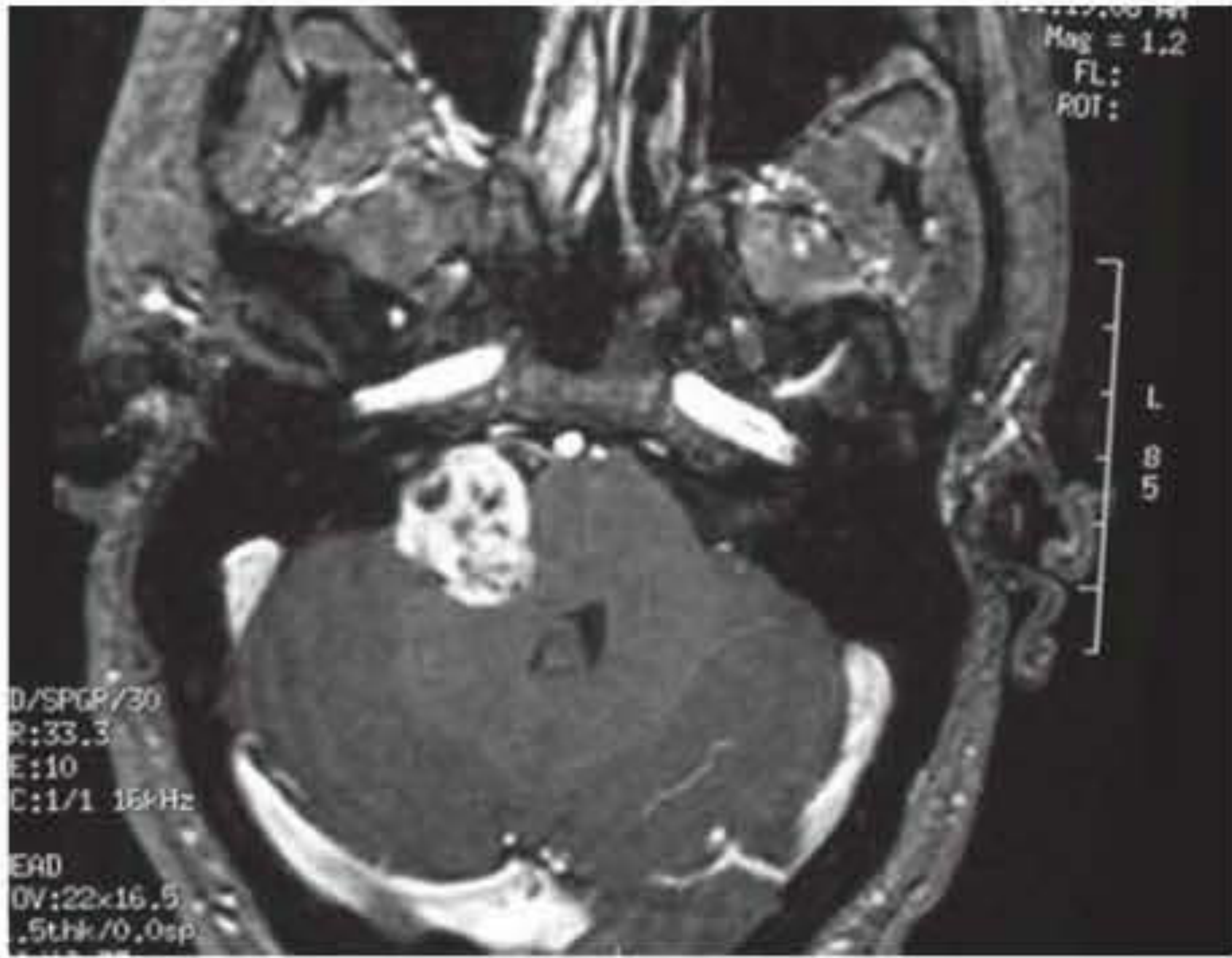
Cystic vestibular schwannoma: (A) T1+Gd axial - enhancing right CPA tumor with central cystic low intensity; (B) T2 axial - hyperintense cysts within the tumor
2. Meningioma
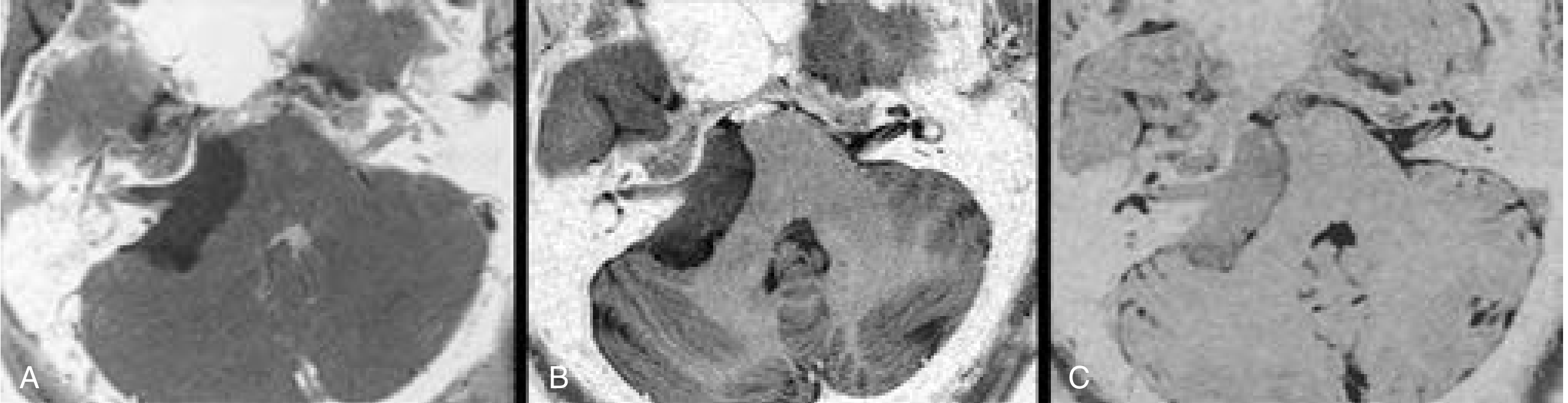
CPA meningioma: (A) Post-Gd T1 - hemispherical enhancing mass with dural tail; (B) T2 - CSF clefts surrounding tumor; (C) CISS - IAC margins better defined
- Location: eccentric to the IAC (does not arise from IAC)
- MRI T1: isointense or hypointense
- MRI T2: variable; surrounding CSF clefts ("CSF cleft sign") characteristic
- Gadolinium: moderate-to-marked, homogeneous enhancement; dural tail sign (enhancing dural attachment) is characteristic but not pathognomonic
- CT: hyperdense on non-contrast; calcifications in ~20-25%; adjacent hyperostosis in ~25%
- CISS/3D-FSE: best delineates IAC involvement and tumor margins
- Bone-tumor angle: obtuse in ~75% (vs. acute in schwannomas)
- IAC involvement is rare; IAC usually patent
3. Epidermoid (Primary Cholesteatoma)
- Location: anterolateral or posterolateral to brainstem; eccentric to porus acusticus; irregular margins
- CT: hypodense (CSF density), non-enhancing; irregular surface; occasional peripheral calcification
- MRI T1: hypointense (similar to CSF)
- MRI T2: homogeneous, isointense or hyperintense to brain
- DWI: bright (restricted diffusion) - the KEY differentiator from arachnoid cyst (which follows CSF signal on all sequences including DWI)
- Shape: variable, tends to insinuate into crevices; "dumbbell" pattern into middle fossa or across to contralateral CPA
- No gadolinium enhancement (enhancing components suggest malignant transformation)
4. Arachnoid Cyst vs. Epidermoid - Key Distinction
| Feature | Epidermoid | Arachnoid Cyst |
|---|---|---|
| CT density | CSF-like, hypodense | CSF-like, hypodense |
| T1 MRI | Hypointense | Hypointense (CSF) |
| T2 MRI | Hyperintense | Follows CSF exactly |
| FLAIR | Does NOT suppress (brighter than CSF) | Suppresses (follows CSF) |
| DWI | Bright (restricted) | Dark (follows CSF) |
| Surface | Irregular, insinuating | Smooth, well-defined |
| Enhancement | None | None |
5. Facial Nerve Schwannoma
- Arises anywhere along the facial nerve course
- Imaging similar to vestibular schwannoma but location follows CN VII, not CN VIII
- May involve geniculate ganglion, labyrinthine segment, or IAC
- MRI T1 + Gd: enhancing mass following facial nerve course
- CT: smooth expansion or erosion of fallopian canal
Special MRI Sequences for CPA
| Sequence | Purpose |
|---|---|
| T1 + Gadolinium | Detection of schwannomas and meningiomas; gold standard |
| T2-weighted FSE / CISS / FIESTA | Non-contrast screening; shows IAC filling defect; nerve anatomy |
| DWI | Epidermoid (restricted) vs. arachnoid cyst (free diffusion) |
| FLAIR | Epidermoid does not suppress vs. arachnoid cyst |
| 3D-FSE / Constructive Interference Steady State (CISS) | Surgical planning; nerve of origin; fundal cap assessment |
Role of CT
CT is adjunctive to MRI for CPA evaluation:
- Best for osseous changes: IAC enlargement (schwannoma), hyperostosis (meningioma), erosion (epidermoid, glomus)
- Non-contrast CT: calcification pattern helps distinguish meningioma
- Primary modality when MRI contraindicated (pacemaker, cochlear implant)
- Characteristic CT finding of acoustic neuroma: ovoid lesion centered on IAC; inhomogeneous moderate enhancement; ~85% show acute angles at bone-tumor interface; contrast CT misses tumors <1.5 cm
Imaging-Based Differential Summary
| Finding | Likely Diagnosis |
|---|---|
| Enhancing mass centered on IAC; IAC enlargement | Vestibular schwannoma |
| Enhancing mass eccentric to IAC; dural tail; hyperostosis | Meningioma |
| Non-enhancing, bright on DWI, irregular, CSF-like density | Epidermoid |
| Non-enhancing, follows CSF all sequences, smooth margins | Arachnoid cyst |
| Enhancing mass following facial nerve, geniculate region | Facial nerve schwannoma |
| Enhancing mass at jugular foramen extending into CPA | Paraganglioma |
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Ch. 179, Common CPA Neoplasms)
- Shambaugh Surgery of the Ear (Ch. 37, Magnetic Resonance Imaging)
Recent literature: A 2025 review (PMID 41052870) specifically addresses vestibular schwannoma imaging and differential diagnosis in Handbook of Clinical Neurology. A 2024 practice guideline (PMID 38346489) from Acta Otorrinolaringol Esp covers VS management including imaging recommendations - no major departures from the above framework are noted.
This is a shared conversation. Sign in to Orris to start your own chat.