Anion gap
Reading File
Finding Sources
Searching PubMed
"anion gap" AND "metabolic acidosis"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a thorough breakdown of the anion gap based on multiple authoritative textbooks.
Anion Gap
Definition and Formula
The anion gap (AG) is a calculated value representing the unmeasured anions in plasma. It arises from the principle of electrical neutrality: total cation charge must equal total anion charge. By looking only at the three most abundant measured electrolytes:
AG = [Na⁺] - ([Cl⁻] + [HCO₃⁻])
- Normal range: 8-12 mEq/L (most labs; some use 10-14 if K⁺ is included)
- The gap is "apparent" because it represents anions that are real but not routinely measured
The normal AG is composed primarily of anionic albumin and, to a lesser extent, phosphate, sulfate, urate, and organic acid anions such as lactate.
- National Kidney Foundation Primer on Kidney Diseases, 8e
Visual: Normal vs. High AG vs. Hyperchloremic Acidosis (Gamblegram)
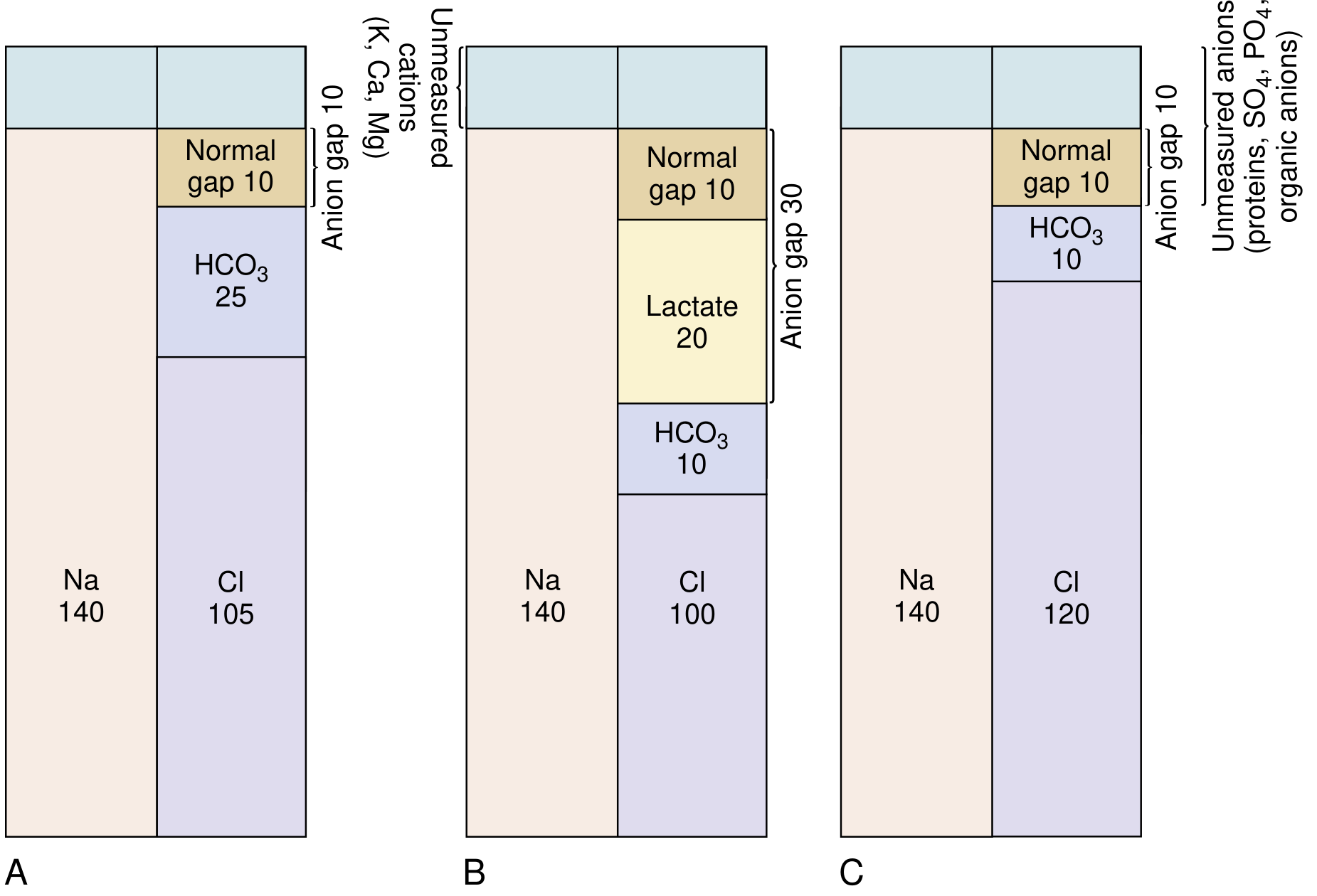
(A) Normal: Na 140, Cl 105, HCO₃ 25, AG = 10
(B) High AG acidosis (lactic): Na 140, Cl 100, HCO₃ 10, Lactate 20 - AG rises to 30
(C) Hyperchloremic/normal AG acidosis: Na 140, Cl 120, HCO₃ 10 - AG stays at 10
Why the Gap Exists
When an unmeasured anion (e.g., lactate, ketoacid) accumulates:
- It titrates HCO₃⁻, causing HCO₃⁻ to fall
- Cl⁻ stays the same (it is not the compensating anion)
- So AG = Na⁺ - (Cl⁻ + HCO₃⁻) increases
When HCO₃⁻ is lost and replaced by Cl⁻ (e.g., diarrhea, RTA):
- One measured anion replaces another
- AG stays normal (hyperchloremic acidosis)
Causes of Metabolic Acidosis by AG Type
High AG Metabolic Acidosis - Mnemonic: GOLDMARK
| Category | Causes |
|---|---|
| Lactic acidosis | Type A (hypoperfusion, sepsis), Type B (metformin, liver failure), D-lactic acidosis |
| Ketoacidosis | Diabetic (DKA), alcoholic, starvation |
| Toxins/Drugs | Methanol, ethylene glycol (glycols), salicylates (aspirin), oxoproline (acetaminophen) |
| Renal failure | Accumulation of sulfate, phosphate, urate, hippurate |
- Costanzo Physiology, 7th Edition; National Kidney Foundation Primer, 8e
Normal AG Metabolic Acidosis (Hyperchloremic)
| Cause | Mechanism |
|---|---|
| Diarrhea | Loss of HCO₃⁻, replaced by Cl⁻ |
| Renal tubular acidosis (RTA) | Failure to excrete acid or retain HCO₃⁻ |
| Carbonic anhydrase inhibitors | Urinary HCO₃⁻ wasting |
| Saline infusion | Dilutional, Cl⁻ load |
| Early renal failure | - |
Albumin Correction (Critical Concept)
The normal AG is largely anionic albumin. In hypoalbuminemia (common in critically ill patients), the AG is falsely low and may mask a true AG acidosis.
Corrected AG (AGc) = AG + 2.5 × (4 - measured albumin [g/dL])
For every 1 g/dL drop in albumin below 4, add 2.5 mEq/L to the AG.
- National Kidney Foundation Primer, 8e
The Delta-Delta Ratio (Δ/Δ)
Once a high AG acidosis is confirmed, the delta-delta ratio detects concurrent metabolic disturbances:
Δ/Δ = (Measured AG - Normal AG) / (Normal HCO₃⁻ - Measured HCO₃⁻) Using: Normal AG = 12, Normal HCO₃⁻ = 24
| Delta Ratio | Interpretation |
|---|---|
| < 0.4 | Hyperchloremic (normal AG) acidosis predominates |
| 0.4 - 1.0 | Mixed high AG + hyperchloremic acidosis |
| 1.0 - 2.0 | Pure high AG metabolic acidosis (expected) |
| > 2.0 | High AG acidosis + concurrent metabolic alkalosis (or pre-existing elevated HCO₃⁻) |
- Miller's Anesthesia, 10e; Barash Clinical Anesthesia, 9e
Osmolar Gap (Special Consideration)
In methanol and ethylene glycol poisoning, a high AG acidosis is accompanied by an osmolar gap (measured osmolality > calculated osmolality by >10 mOsm/kg). This is because these low-molecular-weight toxins directly increase measured osmolality but are not included in the standard osmolality formula. Ketoacids and lactate do NOT typically cause a significant osmolar gap due to their higher molecular weights.
Clinical Approach Summary
- Calculate AG = Na⁺ - (Cl⁻ + HCO₃⁻)
- Correct for albumin if hypoalbuminemic
- If AG > 12: identify cause using GOLDMARK; check for osmolar gap if toxin suspected
- If AG normal: evaluate for hyperchloremic causes (diarrhea, RTA)
- In high AG acidosis: calculate Δ/Δ to unmask mixed disorders
This is a shared conversation. Sign in to Orris to start your own chat.