Suggest some good books for orthopedics and traumatology for a MS3 student
best orthopedics traumatology textbooks for medical students MS3 2024
Orthopedics & Traumatology Books for MS3
Available in Our Library (Accessible Right Now)
| Book | Why It's Good for MS3 |
|---|---|
| Campbell's Operative Orthopaedics, 15th Ed (2026) | The definitive ortho reference - exhaustive coverage of every procedure and condition. Best used as a reference when rotating through ortho, not for cover-to-cover reading. |
| Rockwood and Green's Fractures in Adults, 10th Ed (2025) | The gold standard for trauma - fracture classification, management principles, complications. Essential for trauma rotations. Most up-to-date edition available. |
| Miller's Review of Orthopaedics, 9th Ed | Ideal for MS3 boards prep and rotation review. Condenses the key facts clearly, great for shelf exam preparation. |
Highly Recommended (Not in Library, But Worth Getting)
- Netter's Concise Orthopaedic Anatomy - Consistently ranked #1 by ortho residents for students. Beautiful Netter illustrations linked to clinical relevance. Great to carry on rounds.
- Hoppenfeld's Physical Examination of the Spine and Extremities - Systematic, step-by-step guide to musculoskeletal exam. Invaluable on clinical rotations.
- Handbook of Fractures (Koval & Zuckerman) - Compact, pocket-sized reference. Perfect for the ER and on-call nights. Covers classification systems and management algorithms concisely.
- Apley & Solomon's System of Orthopaedics & Trauma - More student-friendly than Campbell's. Balances basic science, clinical features, and management in a readable format. Very popular in UK/international programs.
- Oxford Handbook of Orthopaedics and Trauma - Pocket reference for ward use, concise and practical.
Suggested Approach for MS3
- Start with Miller's Review (in library) - get the big picture and board-relevant facts
- Use Campbell's (in library) as a reference when you encounter specific conditions on rounds
- Use Rockwood & Green (in library) on trauma/fracture calls
- Carry Netter's Concise Ortho Anatomy or Handbook of Fractures in your white coat pocket for quick lookups
What are the clinical features of fractures? What is a ganglion cyst? Explain Whistler's technique for hip dislocation What is arthroscopy and what are its indications? What is Volkmann's contracture and its complications? What are the indications for K-wire insertion? What are traumatic chest injuries? Differentiate between Smith fracture and Colles fracture. What factors affect bone healing What is Talipes Equino Varus? What are the disadvantages of external fixation? clinical approach to shoulder dislocation? What is arthrotomy and what are its indications? Explain proximal humerus fracture and Neer's classification What are the complications of POP cast? What is fat embolism syndrome? What is a Bennett fracture?
Orthopedics & Traumatology - Complete Study Notes
1. Clinical Features of Fractures
- History of trauma (mechanism of injury)
- Localized pain at the fracture site
- Swelling and visible deformity
- Loss of function of the affected limb
- Local bony tenderness - most important clinical sign
- Local bony irregularity - step deformity palpable
- Crepitus - grating sensation when fragment ends rub; never deliberately elicited (causes pain and neurovascular injury)
- Deformity - angulation, shortening, rotation
- Abnormal mobility - movement at a site where none should exist
- Swelling and bruising/ecchymosis
- X-ray - confirms diagnosis and defines pattern
The most diagnostically important signs are local bony tenderness, local bony irregularity, crepitus, and X-ray findings.
-
Neurovascular injury (check pulses, sensation, motor function distal to fracture)
-
Skin integrity (open vs. closed fracture)
-
Joint involvement
-
S Das Manual on Clinical Surgery, 13th Ed.
2. Ganglion Cyst
- Most common site: dorsal wrist (also volar wrist, foot, finger DIP joint)
- Smooth, tense, transilluminable
- May be painful or symptom-free; pain is often the reason for seeking treatment
- Mucous cysts (finger DIP joint) are associated with underlying osteophytes and may cause nail deformity
- Observation - many resolve spontaneously
- Aspiration ± injection - indicated when symptomatic (pain, paresthesias, motion limitation) or for cosmetic concern
- Surgical excision - performed under regional/general anesthesia by a hand surgeon; risks include infection, neurovascular injury, recurrence, and joint stiffness if arising from a capsular/ligamentous defect
- Pfenninger and Fowler's Procedures for Primary Care; Campbell's Operative Orthopaedics 15th Ed.
3. Whistler's Technique for Hip Dislocation
- Secure the patient's pelvis to the bed with a bed sheet or strap placed over the ischial wings and pubic symphysis (prevents lifting the patient off the bed).
- Bend the contralateral leg so the knee is flexed 90 degrees with the foot flat on the bed.
- Bend the ipsilateral (affected) leg to the same position.
- The clinician places their arm under the ipsilateral knee, which rests on top of the contralateral knee as a fulcrum.
- The clinician rotates their body perpendicular to the patient (facing the feet), assuming a squatting stance.
- While holding the ipsilateral ankle with the other hand, the clinician lifts with the leg muscles (not the back), keeping the arm straight. This applies axial traction on the femur and reduces the dislocation.
- If traction alone fails, the hand on the ankle is used to internally or externally rotate the leg to complete reduction.
- Rosen's Emergency Medicine, Concepts and Clinical Practice
4. Arthroscopy - Definition and Indications
- Torn meniscus - resection or repair
- Anterior/posterior cruciate ligament (ACL/PCL) reconstruction
- Loose body removal
- Cartilage regeneration techniques (e.g., microfracture)
- Septic arthritis washout
- Inflammatory arthritis / pigmented villonodular synovitis (PVNS) - synovectomy
- Diagnosis of unexplained knee pain
- Tibial plateau fractures - allows intraoperative articular surface assessment and reduction
-
Soft-tissue impingement
-
Bony impingement
-
Intraarticular loose bodies
-
Osteochondral lesions of the talus
-
Fractures about the ankle and hindfoot
-
Ankle instability
-
Septic arthritis of the ankle
-
Persistent ankle pain after failed conservative management
-
Bailey and Love's Short Practice of Surgery, 28th Ed.; Campbell's Operative Orthopaedics 15th Ed.
5. Volkmann's Contracture and Its Complications
- Elbow flexion
- Forearm pronation
- Wrist flexion
- Thumb adduction
- MCP joint extension
- Finger flexion (intrinsic-plus posture of the hand)
| Grade | Features | Treatment |
|---|---|---|
| Mild | Partial profundus ischemia; 2-3 finger contractures; no sensory loss | Dynamic splinting; muscle-tendon lengthening/sliding after 3 months |
| Moderate | FDP + FPL + wrist flexors involved; median/ulnar nerve sensory changes; intrinsic minus deformity | Muscle sliding operation + neurolysis |
| Severe | Flexors AND extensors involved; sensory impairment; forearm bone fractures and skin scars | Excision of necrotic muscle + complete neurolysis + free muscle transfers |
-
Permanent flexion contracture of fingers and wrist
-
Median and ulnar nerve dysfunction (sensory and motor deficits)
-
Intrinsic minus hand deformity
-
Joint stiffness and contractures
-
If untreated or severe: loss of hand function
-
Campbell's Operative Orthopaedics 15th Ed.; Tintinalli's Emergency Medicine
6. Indications for K-Wire (Kirschner Wire) Insertion
- Phalangeal fractures - transverse K-wires for long oblique fractures; intramedullary K-wires for short oblique fractures
- Bennett fracture - closed pinning to maintain reduction of the thumb metacarpal base fracture (Wagner technique)
- Pediatric fractures - including adolescent thumb metacarpal base fractures
- Supplementary fixation - e.g., after ORIF where additional stabilization is needed
- Joint fusion (temporary arthrodesis) in some settings
- Holding bone fragments during reduction in periarticular fractures
- Sabiston Textbook of Surgery; Campbell's Operative Orthopaedics 15th Ed.
7. Traumatic Chest Injuries
- Rib fractures (most common)
- Sternal fracture
- Clavicular fracture
- Flail chest - multiple adjacent rib fractures creating a free-floating segment that moves paradoxically with respiration
- Pneumothorax - air in pleural space; tension pneumothorax is life-threatening
- Hemothorax - blood in pleural space; as little as 5 mL is detectable; retained hemothorax is a major complication
- Pulmonary contusion - bruising of lung parenchyma, a major cause of hypoxemia
- Pulmonary laceration
- Aortic injury (traumatic aortic transection) - very high mortality
- Cardiac contusion
- Tracheobronchial injury
- Diaphragmatic injury
- Esophageal injury
- Pneumonia
- Sepsis
- Empyema
- Retained hemothorax
- Chronic pain
- ARDS
- Rockwood and Green's Fractures in Adults, 10th Ed.; Rosen's Emergency Medicine; Murray & Nadel's Respiratory Medicine
8. Colles Fracture vs Smith Fracture
| Feature | Colles Fracture | Smith Fracture |
|---|---|---|
| Type | Extra-articular distal radius fracture | Extra-articular (or intra-articular) distal radius fracture |
| Displacement | Dorsal displacement and angulation of distal fragment | Volar displacement and angulation of distal fragment |
| Mechanism | Fall on outstretched hand (FOOSH) with wrist in dorsiflexion | Fall on dorsum of hand / backward fall with forearm in supination (extreme palmar flexion) |
| Deformity | "Dinner fork" deformity - dorsal prominence | "Garden spade" deformity - volar fullness |
| Population | Common in elderly women (osteoporosis) | Less common; any age |
| Stability | Often stable | More likely unstable, higher rate of operative repair |
| Neurovascular | Acute carpal tunnel syndrome possible | Higher risk of median nerve compression |
| Nickname | - | "Reverse Colles fracture" |
| Treatment | Closed reduction + immobilization in dorsiflexion splint | Closed reduction if extra-articular; often requires operative fixation |
- Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; S Das Manual on Clinical Surgery; Schwartz's Principles of Surgery
9. Factors Affecting Bone Healing
Patient (Host) Factors:
- Age (elderly heal slower)
- Sex/gender
- Comorbidities: renal disease, osteoporosis, arthritis, endocrine disorders (especially diabetes)
- Nutritional status and obesity
- Smoking - strongly linked to delayed union, nonunion, and failure of nonunion treatment
- Vitamin D deficiency
- Metabolic bone diseases
- Medications: NSAIDs, corticosteroids, chemotherapeutics, opioids, anticoagulants
Local/Injury Factors:
- Vascular injury - disrupted blood supply at the fracture site
- Infection (especially in open fractures - nonunion rate approaches 20%)
- Soft tissue compromise and periosteal stripping
- Bone loss/comminution
- Fracture location: femoral neck, scaphoid waist, talar neck, 5th metatarsal base have vulnerable vascular supplies
- Diaphyseal fractures (especially tibial shaft) have limited blood supply vs. metaphyseal fractures
- Radiation exposure
- Mechanical environment (tension-sided fractures prone to nonunion - e.g., subtrochanteric)
Treatment Factors:
-
Damage to blood supply during surgery
-
Poor reduction (malalignment)
-
Inadequate mechanical stability (too flexible or too stiff a construct)
-
Rockwood and Green's Fractures in Adults, 10th Ed.
10. Talipes Equino Varus (TEV / Clubfoot)
- C - Cavus (high arch)
- A - Adductus (forefoot adduction / metatarsus adductus)
- V - Varus (hindfoot varus)
- E - Equinus (plantarflexion deformity - tight Achilles)
- Ponseti technique - serial manipulation and corrective casting, starting in neonatal period. High success rate. Casting may be complete in 1-5 months. The last cast is usually accompanied by a percutaneous Achilles tenotomy to correct the equinus component.
- Foot abduction brace - worn after casting to maintain correction (worn 23 hr/day initially, then nights until age 4-5)
- Surgical release - posteromedial soft tissue release and tendon lengthening, reserved for: severe disease, late presenters (>9 months), or failed conservative treatment
- Schwartz's Principles of Surgery, 11th Ed.
11. Disadvantages of External Fixation
- Cumbersome to the patient - bulky, limits clothing, activities of daily living, and mobility
- Pin site infection - the most common complication; pins traversing skin and soft tissue create a potential route for bacteria
- Pin loosening over time
- Joint stiffness - if the fixator immobilizes an adjacent joint
- Neurovascular injury during pin insertion
- Malunion if reduction is inadequate or lost
- Psychological impact of an external device
- Requires patient compliance with pin site care
- Not suitable for severely obese patients
- Bailey and Love's Short Practice of Surgery, 28th Ed.
12. Clinical Approach to Shoulder Dislocation
- Anterior (subcoracoid) - most common (>95%)
- Posterior - much less common; often missed; associated with epileptic seizures and electrocution
- Inferior (luxatio erecta) - very rare; arm held elevated above head
- Flattening of the deltoid contour (normally rounded)
- Shoulder drops in a straight line from the acromion tip (loss of normal curve)
- Patient holds arm against the chest, supported by the other hand
- Fullness/prominence below the clavicle (humeral head palpable anteriorly)
- Mandatory neurological examination - axillary nerve injury is not uncommon; produces deltoid paralysis + sensory blunting over the deltoid insertion ("regimental badge" area)
- Assess also for brachial plexus injury and axillary artery injury (rare)
- Hanging arm (Stimson) - patient prone with arm hanging over bed edge; weight of arm + muscle relaxation allows spontaneous reduction
- Hippocratic method - patient supine; traction on arm with foot counter-traction in axilla (historical, less commonly used)
- Milch technique, Cunningham technique, FARES method are modern alternatives requiring less sedation
- Adequate analgesia/sedation is essential before any technique
- Arm in broad sling, strapped to chest for 3 weeks
- Neurological re-assessment post-reduction
- Physiotherapy for range of motion after sling removed
- In the elderly: shorter immobilization to prevent stiffness
- Pye's Surgical Handicraft, 22nd Ed.
13. Arthrotomy and Its Indications
- Septic arthritis - joint washout and debridement; arthrotomy is preferred over arthroscopy in very young children or when arthroscopy is not available
- Intra-articular fracture fixation - open reduction and internal fixation when arthroscopic assistance is insufficient
- Removal of loose bodies - when arthroscopy is not feasible or multiple/large bodies are present
- Total joint replacement - entry to the joint is by arthrotomy
- Synovectomy - in inflammatory arthritis if arthroscopic synovectomy is not possible
- Osteochondral fragment fixation - reduction and fixation of detached osteochondral fragments; important note: loose bodies move freely between compartments when the joint is opened, so careful exploration is required
- Bone biopsy or tumor surgery involving a joint
- Campbell's Operative Orthopaedics 15th Ed.
14. Proximal Humerus Fracture and Neer's Classification
- Humeral head (articular segment)
- Greater tuberosity
- Lesser tuberosity
- Humeral shaft (diaphysis)
- 1-part fracture - no fragment displaced >1 cm or angulated >45 degrees, regardless of number of fracture lines (most common; ~80%)
- 2-part fracture - one fragment displaced
- 3-part fracture - two fragments displaced
- 4-part fracture - all four segments displaced (highest risk of avascular necrosis of the humeral head)
- Articular surface fractures - head-splitting or impression fractures (anterior = Hill-Sachs lesion; posterior = reverse Hill-Sachs)
- Poor interobserver reliability - in one study, all 5 observers agreed in only 30-32% of cases
- Poor radiographs (difficult to obtain a true lateral in an acute injury) worsen reliability
- The definitions (1 cm / 45°) are clear but often misapplied
- CT scan significantly improves classification accuracy
-
1-part and many 2-part fractures: conservative management (sling, physiotherapy)
-
Displaced 2-part, 3-part, 4-part fractures in active patients: ORIF or hemiarthroplasty
-
4-part fractures in elderly: reverse shoulder arthroplasty often preferred
-
Rockwood and Green's Fractures in Adults, 10th Ed.
15. Complications of POP (Plaster of Paris) Cast
- Pressure sores / skin necrosis - from improperly applied cast, inadequate padding, or swelling after application
- Compartment syndrome - the most dangerous complication; tight cast restricts swelling, raises intracompartmental pressure, leads to ischemia. Warning signs: pain out of proportion, pain on passive stretch, pallor, paresthesia, paralysis, pulselessness (the 5 P's or 6 P's). Requires urgent cast splitting/removal and fasciotomy
- Volkmann's ischemic contracture - late consequence of unrelieved compartment syndrome (see above)
- Thermal injury - heat generated during plaster setting can burn the skin
- Neurovascular compromise - nerve palsy from direct pressure (e.g., peroneal nerve at fibular neck)
- Joint stiffness - from prolonged immobilization (especially elbow and shoulder)
- Muscle wasting/weakness - disuse atrophy
- DVT - reduced mobility, especially lower limb casts
- Skin maceration and fungal infections under the cast
- Malunion - loss of fracture reduction within the cast
- Delayed union / nonunion - immobilization alone may not provide adequate stability
- Osteoporosis - localized disuse osteoporosis
- Algodystrophy / CRPS - complex regional pain syndrome post-cast removal
16. Fat Embolism Syndrome (FES)
- Most common after fractures of the tibia and femur in young adults, or hip fractures in the elderly
- Incidence: 1-2% after isolated long bone fracture; 5-10% with multiple fractures
- Symptoms appear 1-2 days after injury or after intramedullary surgical nailing
- Respiratory - respiratory distress, hypoxemia (earliest and most common); ARDS may develop and is the usual cause of death
- Neurological - restlessness, confusion, deteriorating consciousness (early sign)
- Petechial rash - from thrombocytopenia; classically over the chest, axillae, conjunctivae
- Fever
- Tachycardia
- Jaundice
- Retinal changes (fat emboli visible on fundoscopy)
- Renal involvement
- Fat in urine (lipuria) in 50% of patients within 3 days
- CT chest: ground glass opacities and consolidation
-
Primarily supportive - ICU care
-
Supplemental oxygen; often requires mechanical ventilation (intubation)
-
Early fracture fixation reduces risk
-
Mortality once FES develops: 10-20%
-
Rosen's Emergency Medicine
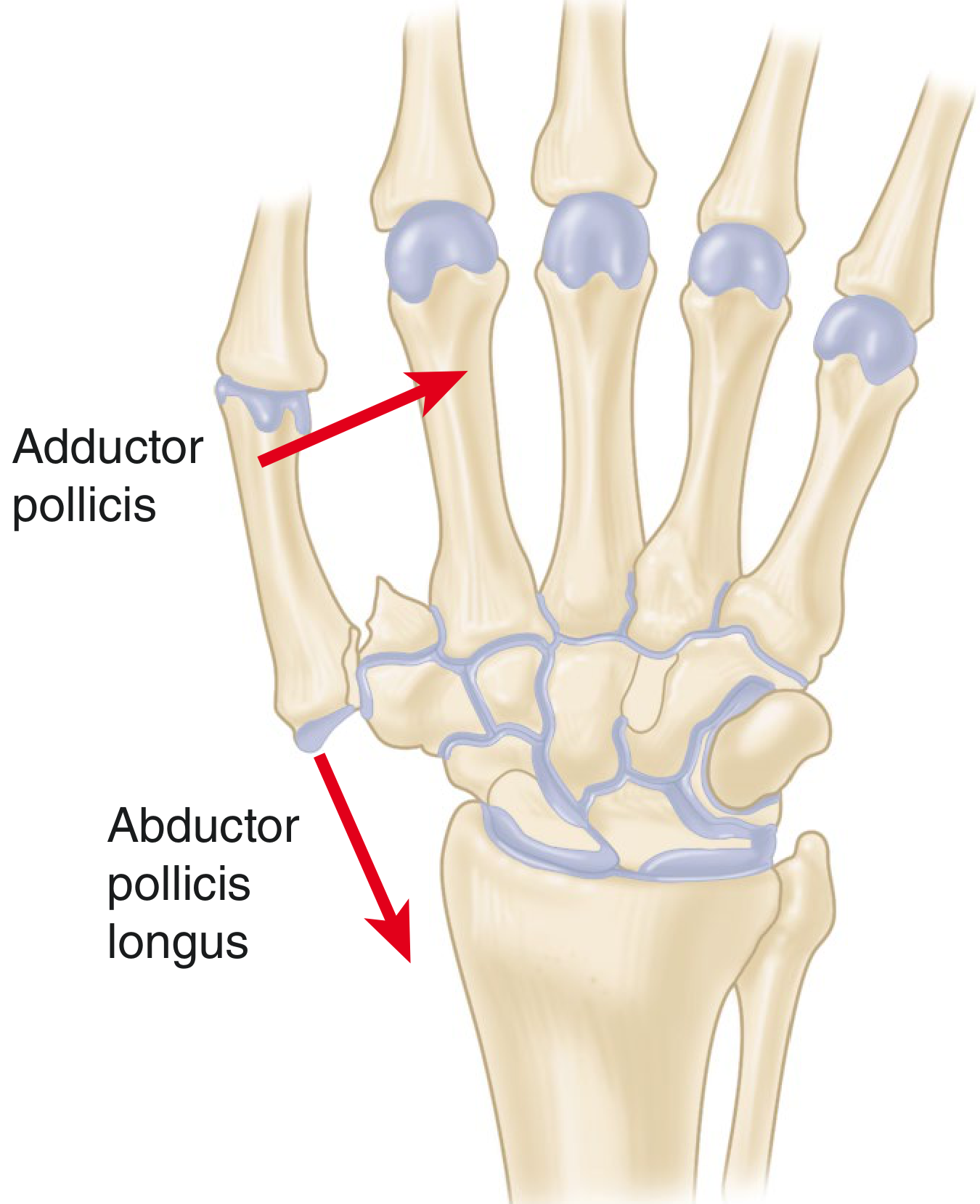
17. Bennett Fracture
- The fracture line creates a small volar-medial fragment which is held in place by the volar oblique (beak) ligament attached to the trapezium
- The remainder of the thumb metacarpal shaft is displaced laterally and dorsally by the unopposed pull of the abductor pollicis longus (APL)
- The adductor pollicis contributes to the deforming force
- Pain, swelling, and bruising at the base of the thumb
- Tenderness and deformity at the first CMC joint
- Weakness of grip
- X-ray confirms the intra-articular fracture line
- Closed reduction is possible but difficult to maintain (cast pressure alone often unsatisfactory and risks skin necrosis)
- Gold standard: Closed reduction and percutaneous K-wire fixation (Wagner technique) - K-wire from the thumb metacarpal into the trapezium or index metacarpal to hold reduction
- ORIF if closed reduction is inadequate (>1-3 mm articular incongruity)
- Articular incongruity of 1-3 mm is generally well-tolerated if union and joint stability are achieved
- Campbell's Operative Orthopaedics 15th Ed.; Imaging Anatomy: Bones, Joints, Vessels and Nerves