Give important long ques and short ques from whole syllabus of forensic medicine from reddy book for models examination mbbs
Important Questions - Forensic Medicine & Toxicology
(Reddy's Essentials, 36th Edition - 2026)
For Model/University Examinations MBBS
SECTION A: FORENSIC MEDICINE
CHAPTER 1 - INTRODUCTION, HISTORY & ETHICS
- Describe and discuss ethical principles: Respect for autonomy, non-maleficence, beneficence and justice.
- Differentiate between nonmaleficence and beneficence.
- Mention the skills needed for a successful medico-legal practice.
- Mention the basic principles of ethics.
- What is Autonomy?
- What is Beneficence?
- What is Nonmaleficence?
CHAPTER 2 - LEGAL COMPETENCIES, COURTS & MEDICAL WITNESS
- Enumerate the criminal courts in India in order. What are the powers of magistrate courts?
- Describe in brief the trial of an expert witness in the court. What is perjury? What is hearsay evidence?
- Explain the difference between common and expert witness.
- Explain the difference between dying declaration and dying deposition.
- Cognizable offence
- Cross examination
- Perjury
- Dying deposition
- Hostile witness
CHAPTER 3 - MEDICAL NEGLIGENCE & NATIONAL MEDICAL COMMISSION
- Define medical negligence and describe the defenses available for doctors in cases of medical negligence.
- Give an account of the constitution and functions of the National Medical Commission (NMC).
- Describe the disciplinary control over medical practitioners, including penal erasure, infamous conduct, and warning notices issued by the NMC.
- Consent
- Professional misconduct
- Vicarious liability
- Professional secrecy
- Privileged communication
- Write a short note on Dichotomy.
- State the difference between civil and criminal negligence.
- Write a short note on Res judicata.
CHAPTER 4 - IDENTIFICATION
- Define identification. Write in detail the medico-legal importance of bones in identification.
- Describe in detail the medico-legal importance of teeth.
- Describe in detail the medico-legal importance of age. Give a note on how teeth help in determining age.
- What are all the data used for human identification for civil and criminal cases?
- Write a note on Dactylography.
- Discuss Disorders of Sexual Development (DSD) and their medico-legal significance.
- How will you perform age estimation by Gustafson's method?
- Write a note on Inter-sex and its medico-legal importance.
- Describe in detail the medico-legal importance of Hair.
- State the medico-legal importance of Age 18.
- Klinefelter's Syndrome
- Concealed sex
- Difference between human and animal hair
- Mixed dentition
- Pseudohermaphroditism
- Rule of Haase
- Poroscopy
CHAPTER 5 - POSTMORTEM EXAMINATION (AUTOPSY)
- What are the prerequisites for postmortem examination? Describe various types of incisions and methods for organ removal in postmortem examination.
- Explain various dissection techniques used at Autopsy.
- Dissection procedure of stomach while conducting a medicolegal autopsy.
- Aims and objectives of medicolegal autopsy.
- Discuss the role of Virtopsy in forensic medicine.
- Letulle technique.
- Exhumation.
CHAPTER 6 - DEATH & THANATOLOGY
- What are the criteria to diagnose brain stem death and its significance?
- Sudden death.
- Negative autopsy.
- Define obscure autopsy.
- Enumerate Minnesota criteria of brain death.
CHAPTER 7 - POSTMORTEM CHANGES & TIME SINCE DEATH
- Classify postmortem changes. What are the methods of estimating the time since death?
- What is Rigor mortis? Discuss in detail the formation and factors affecting formation of rigor mortis. Add a note on cadaveric spasm.
CHAPTER 8 - MECHANICAL INJURIES (WOUNDS)
- Define injury. Describe the types and medico-legal importance of abrasions.
- A 35-year-old man was found dead in front of a mirror, having a cut-throat injury with a blood-stained knife firmly clasped in his hand. He had multiple superficial cuts over the flexor aspect of left forearm with a reddish-brown scab. Analyze and answer:
- A. Identify the nature of injury.
- B. Explain the findings suggestive of manner of injury during postmortem.
- C. Mention the reason for clasping the knife.
- D. Explain the inference you would draw from the forearm injuries.
- Define laceration. Mention the various types and describe any two types. Mention the features of a lacerated wound.
- What is culpable homicide? Discuss justifiable homicide.
- Define wound. Discuss the medico-legal classification of wounds and their importance in determining the nature of weapon, manner of death, and cause of death.
- Describe the medico-legal aspects of mechanical injuries - abrasions, contusions, lacerations, stab wounds, and firearm injuries.
- Differentiate between suicidal and homicidal cut-throat injuries.
- Difference between incised wound and stab wound.
- Difference between penetrating and perforating injuries with examples.
- Describe the medico-legal importance of abrasions.
- Write short notes on medico-legal aspects of contusions (bruises).
- Discuss the medico-legal significance of lacerated wounds.
- Write short notes on incised wounds and their medico-legal importance.
- Explain the medico-legal aspects of stab wounds.
- Write short notes on the medico-legal value of firearm injuries.
- Patterned bruising.
- Tentative cuts.
- Ricochet bullet.
- Self-inflicted injuries.
- Chop wound.
- Ectopic contusion.
- Define a wound in medico-legal terms.
- What is the medico-legal importance of defense wounds?
- Define hesitation cuts.
- Give two examples of fabricated wounds.
CHAPTER 9 - REGIONAL INJURIES
- Define regional injuries. Describe the types, medico-legal significance, and postmortem findings of regional injuries involving the head, neck, chest, and abdomen. Discuss their importance in determining cause of death.
- Write short notes on scalp injuries and their medico-legal importance.
- Describe the different types of intracranial hemorrhages with medico-legal relevance.
- Explain the medico-legal importance of neck injuries.
- Write short notes on rib fractures and their complications.
- Describe the medico-legal aspects of abdominal injuries.
- Write short notes on injuries to the spinal cord and their medico-legal significance.
- Explain the importance of defense wounds in regional injuries.
- Write short notes on regional injuries in road traffic accidents.
- List the types of scalp hemorrhages seen in head injuries.
- Name two types of intracranial hemorrhage.
- Define concussion.
- What is a contre-coup injury?
- Mention two medico-legal points of neck injuries.
- List common causes of rib fractures.
- What is the medico-legal importance of abdominal injuries?
- Define defense wounds and give one example.
- Name two complications of spinal cord injury.
- What is the significance of regional injuries in road traffic accidents?
CHAPTER 10 - THERMAL INJURIES
- Define thermal deaths. Discuss in detail the causes, pathophysiology, clinical features, postmortem findings, and medico-legal importance of deaths due to burns, heat stroke, hypothermia, and electrocution.
- Discuss the postmortem findings in death due to burns.
- Write short notes on the medico-legal importance of pugilistic attitude.
- Describe the clinical features and postmortem findings of heat stroke.
- Explain the medico-legal aspects of death due to hypothermia.
- Write short notes on immersion hypothermia (death in cold water).
- Define thermal death.
- What is the pugilistic attitude?
- Name two postmortem findings in burn deaths.
- What is the medico-legal importance of soot in the airways?
- Mention two causes of heat stroke.
- What is heat rigor?
- List two postmortem findings of hypothermia.
- Define immersion foot/trench foot.
CHAPTER 11 - STARVATION
- Define starvation. Describe in detail the clinical features, stages, postmortem findings, and medico-legal significance of starvation.
- Define starvation and mention its types.
- Describe the stages of starvation with clinical features.
- Write the postmortem findings of starvation.
- Discuss the medico-legal importance of starvation.
- Differentiate between acute and chronic starvation.
- Enumerate causes of starvation and mention their types.
- What are the postmortem findings in starvation death?
CHAPTER 12 - ASPHYXIA
- Define mechanical asphyxia. Discuss in detail the types, pathophysiology, clinical features, postmortem findings, and medico-legal importance of mechanical asphyxia.
- Define mechanical asphyxia. Enumerate its various types with examples.
- Discuss the pathophysiology of death in mechanical asphyxia.
- Describe the postmortem findings in hanging.
- Describe the postmortem findings in strangulation.
- Write a short note on traumatic asphyxia.
- Discuss the medico-legal importance of drowning.
- Differentiate between suicidal hanging and homicidal strangulation.
- Write a short note on café coronary.
- Discuss postmortem findings in smothering.
- Write a short note on throttling and its medico-legal significance.
CHAPTER 13 - ANESTHETIC & OPERATIVE DEATHS
- Define anesthetic and operative deaths. Discuss in detail the causes, clinical features, postmortem findings, and medico-legal importance of deaths occurring during or following anesthesia and surgical operations.
- Malignant hyperthermia.
- Describe the common postmortem findings in anesthetic deaths.
- Write short notes on respiratory causes of anesthetic death.
- Discuss the medico-legal importance of consent in operative deaths.
- Define anesthetic death.
- What is meant by operative death?
- Mention two respiratory causes of anesthetic death.
- Give two cardiac causes of anesthetic death.
- Name two examples of drug-related causes of anesthetic death.
CHAPTER 14 - IMPOTENCE, STERILITY & SEXUAL MEDICINE
- Define impotence and sterility. Explain the causes of impotence and sterility in male and female.
- Describe Artificial Insemination.
- What are the causes of male infertility? Name the methods of overcoming each cause.
- Causes of temporary impotence in male.
- Name and discuss various methods of sterilization.
- Impotence quoad hoc.
CHAPTER 15 - RAPE & SEXUAL OFFENCES
- Define rape. Describe the procedure of examination of a victim of rape. Add a note on materials to be collected for laboratory investigations.
- A child of 8 years of age suddenly started acting very withdrawn, with crying and anger episodes. Parents suspect sexual abuse. Discuss:
- A. Specific laws pertaining to such cases (POCSO) and role of doctor in intimation to police.
- B. Medical examination and probable signs and symptoms.
- C. Possible criteria to rule out parental involvement.
- Evidentiary materials collected in a victim of rape and their relevance.
- Sodomy.
- POCSO Act 2012.
- Signs of recent penetration into female genitalia.
- Voyeurism.
- Findings in a habitual passive agent.
- Transvestism.
- Sadism.
- Incest.
CHAPTER 16 - INFANTICIDE
- Define infanticide. Describe methods usually adopted for carrying out infanticide. Add a note on macerated fetus.
- Differentiate between still birth and live birth. Describe features of live birth.
- A dead fetus recovered from dustbin brought for postmortem - how will you assess viability from ossification centres? How will you differentiate live birth from still born?
- Sudden Infant Death Syndrome (SIDS).
- Battered baby syndrome.
- Write a short note on maceration.
- Write a short note on the viability of fetus.
- Define still birth.
CHAPTER 17 - CRIMINAL ABORTION
- Discuss the different causes of death and pathology of different organs in cases of death due to criminal abortion.
- Indications for termination of pregnancy under Medical Termination of Pregnancy Act (Amendment Act) 2021.
CHAPTER 18 - FORENSIC BIOLOGY / BLOOD STAINS
- Define blood stains. Discuss the methods of identification and confirmation of blood stains, including chemical, microscopic, and serological tests. Explain the medico-legal importance of blood stain examination.
- Name the confirmatory tests for blood and their applications in medico-legal practice.
- Kastle-Meyer test.
- Secretors.
- Microscopic tests for blood stain detection.
- Paternity tests.
CHAPTER 19 - POSTMORTEM ARTEFACTS
- What are postmortem artefacts? Describe in detail the artefacts produced by putrefaction, animal activity, and resuscitative procedures, and discuss their medico-legal importance.
- Discuss artefacts caused by injuries during handling, transportation, and autopsy. How can these be differentiated from true ante-mortem injuries?
- Enumerate the types of postmortem artefacts and explain their medico-legal importance.
- Artefacts due to decomposition.
- Agonal artefacts.
- Resuscitative artefacts.
- Artefacts of autopsy.
SECTION B: TOXICOLOGY
Note: The Toxicology section covers multiple chapters on general principles of toxicology and specific poisons. Key question themes from the book include:
- Classify poisons. Describe the general management of a case of acute poisoning (gastric lavage, antidotes, supportive care).
- Describe the clinical features, postmortem findings, and treatment of organophosphorus (OP) compound poisoning.
- Describe the clinical features, postmortem findings, and treatment of corrosive acid poisoning (H₂SO₄, HCl, HNO₃).
- Describe the clinical features, postmortem findings, and treatment of alkali poisoning.
- Describe the clinical features, postmortem findings, and treatment of opium/morphine poisoning.
- Describe the clinical features, postmortem findings, and treatment of alcohol (ethyl/methyl) poisoning.
- Describe the clinical features, postmortem findings, and treatment of carbon monoxide poisoning.
- Describe the clinical features, postmortem findings, and treatment of arsenic poisoning.
- Describe the clinical features, postmortem findings, and treatment of snake bite.
- Carbamate poisoning vs. organophosphorus poisoning.
- Atropine treatment in OP poisoning.
- Pralidoxime (PAM) - mechanism of action.
- Carbon monoxide poisoning postmortem findings (cherry-red lividity).
- Dhatura/Belladonna alkaloid poisoning - features.
- Barbiturate poisoning.
- Cannabis poisoning.
- Lead poisoning (chronic) - features and treatment.
- Mercury poisoning.
- Cyanide poisoning - clinical features and treatment.
- DDT poisoning.
- Alcohol - medico-legal aspects.
- Preservatives used for viscera in poisoning cases.
- SLUDGE syndrome (OP poisoning).
- Mees' lines (arsenic).
- Peripheral neuropathy in arsenic.
- Gastric lavage contraindications.
- Acrodynia (pink disease - mercury).
- Blue line of gums (lead poisoning).
- Burtonian line.
- Wrist drop vs. foot drop.
- Diatom test in drowning.
- Gettler test.
- Classification of poisons (irritant, corrosive, neurotic, cardiac).
QUICK REFERENCE: HIGH-YIELD TOPICS FOR MODELS EXAM
| Priority | Topic | Type |
|---|---|---|
| ★★★ | Medical negligence & defenses | Long |
| ★★★ | Rigor mortis - formation, factors, cadaveric spasm | Long |
| ★★★ | Mechanical asphyxia - hanging vs. strangulation | Long |
| ★★★ | Rape - examination procedure | Long |
| ★★★ | Identification (bones, teeth, age) | Long |
| ★★★ | Organophosphorus poisoning | Long |
| ★★★ | Postmortem changes / time since death | Long |
| ★★★ | Mechanical injuries classification | Long |
| ★★ | NMC - constitution and functions | Long |
| ★★ | Infanticide vs. stillbirth | Long |
| ★★ | Criminal abortion - causes of death | Long |
| ★★ | Thermal deaths (burns, heat stroke) | Long |
| ★★ | Consent | Short |
| ★★ | Professional misconduct | Short |
| ★★ | Dying declaration vs. dying deposition | Short |
| ★★ | POCSO Act | Short |
| ★★ | SIDS | Short |
| ★★ | Battered baby syndrome | Short |
| ★★ | Dactylography | Short |
| ★★ | Gustafson's method | Short |
| ★★ | Café coronary | Short |
| ★★ | Contra-coup injury | Short |
| ★★ | Carbon monoxide poisoning | Short |
| ★★ | Kastle-Meyer test | Short |
| ★ | Perjury | Short note |
| ★ | Ectopic contusion | Short note |
| ★ | Poroscopy | Short note |
| ★ | Virtopsy | Short note |
| ★ | Letulle technique | Short note |
| ★ | Malignant hyperthermia | Short note |
Tip for exam preparation: Focus especially on chapters covering Mechanical Injuries, Asphyxia, Postmortem Changes, Identification, Medical Negligence, and Toxicology (OP compounds, corrosives, CO) - these are the most consistently tested topics across university model exams.
Give important topics
⭐ HIGH-YIELD TOPICS - Forensic Medicine (Reddy)
For MBBS Model Examination
🔴 MUST PREPARE (Appear Every Exam)
Forensic Medicine
| # | Topic | Expected Question Type |
|---|---|---|
| 1 | Rigor Mortis - formation, factors, cadaveric spasm, differences | Long Essay |
| 2 | Mechanical Asphyxia - types, PM findings, hanging vs. strangulation | Long Essay |
| 3 | Medical Negligence - definition, types, defenses available to doctor | Long Essay |
| 4 | Mechanical Injuries - classification, abrasions, bruises, lacerations, stab | Long Essay |
| 5 | Identification - bones, teeth, age, Gustafson's method | Long Essay |
| 6 | Rape - definition, examination procedure, evidence collection | Long Essay |
| 7 | Postmortem Changes - early & late, time since death estimation | Long Essay |
| 8 | Infanticide - definition, methods, live birth vs. stillbirth | Long Essay |
Toxicology
| # | Topic | Expected Question Type |
|---|---|---|
| 1 | Organophosphorus Poisoning - features, PM findings, treatment, PAM | Long Essay |
| 2 | Corrosive Acid Poisoning - H₂SO₄/HCl/HNO₃, features, PM findings | Long Essay |
| 3 | Alcohol Poisoning - ethyl vs. methyl, medico-legal aspects | Long Essay |
| 4 | Carbon Monoxide Poisoning - cherry-red lividity, features, treatment | Long Essay |
| 5 | Arsenic Poisoning - acute/chronic, Mees' lines, PM findings | Long Essay |
| 6 | General Management of Acute Poisoning - gastric lavage, antidotes | Long Essay |
🟡 VERY IMPORTANT (Frequent Short/Long Essays)
Forensic Medicine
- NMC - constitution, functions, disciplinary control, penal erasure
- Consent - types, informed consent, exceptions
- Cut-throat injuries - suicidal vs. homicidal differences
- Thermal injuries - burns, heat stroke, hypothermia, electrocution
- Regional head injuries - coup/contre-coup, intracranial hemorrhages
- Criminal abortion - causes of death, methods, PM findings
- Postmortem artefacts - types, medico-legal importance
- Drowning - wet vs. dry, diatom test, Gettler test
- Firearm injuries - entry vs. exit wound, contact/close range
- Blood stain examination - confirmatory tests (Kastle-Meyer, precipitin)
- Expert witness - vs. common witness, perjury, dying declaration
- Dactylography - fingerprints, types, medico-legal value
- POCSO Act 2012 - provisions, role of doctor
- Starvation - stages, PM findings, medico-legal importance
- Brain death - criteria (Harvard/Minnesota), significance
🟢 IMPORTANT SHORT NOTES (Write in 5-10 lines)
Forensic Medicine
- Cadaveric spasm
- Café coronary
- Ectopic contusion
- Patterned bruising
- Hesitation/tentative cuts
- Virtopsy
- Letulle technique
- Exhumation
- Poroscopy
- Dactylography
- Pseudohermaphroditism / Klinefelter's syndrome
- SIDS (Sudden Infant Death Syndrome)
- Battered baby syndrome
- Maceration of fetus
- Privileged communication
- Professional secrecy
- Vicarious liability
- Dying declaration vs. dying deposition
- Malignant hyperthermia
- Pugilistic attitude (burns)
- Immersion foot / trench foot
Toxicology
- SLUDGE syndrome (OP poisoning)
- Mees' lines
- Burtonian/blue line of gums (lead)
- Acrodynia / Pink disease (mercury)
- Wrist drop (lead) / Foot drop
- Diatom test
- Preservatives used for viscera
- Pralidoxime (PAM) - mechanism
- Dhatura/Belladonna poisoning
- Cannabis poisoning
- Cyanide poisoning
- DDT poisoning
📌 TOPIC-WISE PRIORITY SUMMARY
SECTION 1 - FORENSIC MEDICINE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Priority 1 (LE): Rigor mortis, Asphyxia, Negligence,
Injuries, Identification, Rape, PM changes
Priority 2 (SE): Consent, NMC, Drowning, Regional injuries,
Hanging, Strangulation, Infanticide, Abortion
Priority 3 (SN): Cadaveric spasm, Ectopic contusion, SIDS,
Perjury, Café coronary, Tentative cuts
SECTION 2 - TOXICOLOGY
━━━━━━━━━━━━━━━━━━━━━━
Priority 1 (LE): OP poisoning, Corrosive acids, CO poisoning,
Arsenic, Alcohol, Acute poisoning management
Priority 2 (SE): Dhatura, Barbiturates, Lead, Mercury, Snake bite
Priority 3 (SN): SLUDGE, Mees' lines, PAM, Burtonian line,
Diatom test, Preservatives for viscera
Golden Rule for Models: If a topic has a dedicated chapter in Reddy + appears in the NMC competency table (FM1.x, FM2.x, FM3.x) - it WILL come in the exam. Focus your long essay preparation on those 6-8 topics per section listed under "Must Prepare."
Important ques from legal procedure section
📋 Important Questions - Legal Procedure Section
Forensic Medicine (Reddy's 36th Edition)
MBBS Model Examination
🔴 LONG ESSAY QUESTIONS
-
Enumerate the criminal courts in India in order. What are the powers of each magistrate court?
-
Describe in brief the trial of an expert witness in the court. What is perjury? What is hearsay evidence?
-
What is an inquest? Differentiate between police inquest and magistrate's inquest. Mention the cases in which magistrate's inquest is mandatory.
🟡 SHORT ESSAY QUESTIONS
-
Explain the difference between a common witness and an expert witness.
-
Explain the difference between dying declaration and dying deposition.
-
Describe the conduct of a doctor in the witness box.
-
What is an inquest? Classify and explain its types.
-
Write a note on crime scene investigation - duties and responsibilities of a doctor.
🟢 SHORT ANSWER / SHORT NOTES
- Cognizable vs. non-cognizable offence - definition and examples
- Cross-examination - definition, purpose, leading questions
- Perjury - definition, punishment (S.229 BNS), when it occurs
- Dying deposition - definition, vs. dying declaration
- Hostile witness - definition, consequences
- Hearsay evidence - definition and example
- Subpoena / Summons - definition, types, punishment for non-attendance
- Chain of custody - definition and importance
- Conduct money
- Examination-in-chief, cross-examination, re-examination - differences
📌 TOPIC-WISE DETAIL (What to Know for Each Topic)
1. COURTS OF LAW (FM1.4)
| Court | Key Powers |
|---|---|
| Supreme Court | Highest appellate court, binding on all courts |
| High Court | Try any offence, pass any sentence; confirms death sentence |
| Sessions Court | Cannot try case until committed by Magistrate; death sentence needs HC confirmation |
| Chief Judicial Magistrate | Up to 7 years imprisonment |
| First Class Magistrate | Up to 3 years + fine |
| Second Class Magistrate | Up to 1 year + fine |
2. INQUEST (FM1.3)
- Conducted by: Officer-in-charge of police station (min. rank: Head Constable)
- Cases: Suicide, killed by person/animal/accident, suspicious deaths
- Doctor's role: Certify cause of death, examine body externally
- Prepares: Inquest report (panchanama)
- Death in police custody
- Death in prison/jail
- Dowry death (within 5 years of marriage)
- Exhumation cases
- Death of mentally ill person in psychiatric hospital
- Rape victims who die during treatment
3. WITNESSES (FM1.5)
| Feature | Common Witness | Expert Witness |
|---|---|---|
| Definition | Gives evidence of facts he personally observed | Gives opinion based on specialized knowledge |
| Knowledge | First-hand (personal observation) | Technical/scientific training |
| Allowed to give | Facts only | Facts + Opinion |
| Example | Eyewitness to accident | Doctor, fingerprint expert |
| Conduct money | Entitled | Not entitled (government duty) |
4. EXAMINATION OF WITNESS IN COURT
- Examination-in-chief: Questions by the side that called the witness. No leading questions allowed.
- Cross-examination: Questions by opposing counsel. Leading questions ARE allowed.
- Re-examination: By original side, only on new matters raised in cross-examination.
- Court questions: Judge may ask at any stage.
5. DYING DECLARATION vs. DYING DEPOSITION
| Feature | Dying Declaration | Dying Deposition |
|---|---|---|
| Recorded by | Magistrate / Doctor / Any person | Magistrate only |
| Oath | Not on oath | On oath |
| Cross-examined? | No | Yes |
| Admissibility | Admissible as secondary evidence | Admissible as primary evidence |
| Used when | Person likely to die / cannot attend court | Person too ill to attend court but alive |
| Legal basis | S.26, BSA (S.32 IEA) | S.351, BNSS (S.299 CrPC) |
| Weight in court | Less | More |
6. PERJURY (S.229 BNS)
- Definition: Giving false evidence (deliberately lying under oath in a court of law)
- Punishment: Imprisonment up to 7 years + fine
- Issuing/signing a false certificate: Punishable under S.234, BNS
- A doctor who gives a false certificate is liable for perjury
7. DOCUMENTARY EVIDENCE - TYPES
- Medical Certificates - ill-health, fitness, age, death
- Medico-Legal Reports - wound certificate, MLC report
- Post-mortem Certificate - cause of death
8. MEDICOLEGAL CASE (MLC) - IMPORTANT POINTS
- Traffic accidents, assaults, sexual offences
- Criminal abortion, burns, poisoning
- Deaths during operation/anesthesia
- Cases referred by police or court
- Suspicious deaths, suicides, homicides
9. NEW ACTS (2023) - MUST KNOW
| Old Act | New Act (2023) |
|---|---|
| Indian Penal Code (IPC) 1860 | Bharatiya Nyaya Sanhita (BNS) |
| Criminal Procedure Code (CrPC) 1973 | Bharatiya Nagarika Suraksha Sanhita (BNSS) |
| Indian Evidence Act (IEA) 1872 | Bharatiya Sakshya Adhiniyam (BSA) |
10. CRIME SCENE INVESTIGATION (FM2.23)
- Who - victim identification
- When - time of death/injuries
- Where - scene of death
- What - injuries present
- Which - significant injuries
- Why/How - mechanism and manner of death
Exam Tip: From the legal procedure section, the most commonly asked topics are:
- Courts + their powers (long essay)
- Expert witness vs. common witness (short essay)
- Dying declaration vs. dying deposition (short essay or table)
- Perjury (short note)
- Inquest types (short essay)
- BNS/BNSS/BSA - new acts replacing IPC/CrPC/IEA (short note)
Give important topics
⭐ Important Topics - Legal Procedure Section
Forensic Medicine (Reddy's 36th Edition)
🔴 MUST PREPARE (Always Asked)
| # | Topic | Type |
|---|---|---|
| 1 | Courts of Law - types, hierarchy, powers of each | Long Essay |
| 2 | Expert Witness vs. Common Witness | Short Essay |
| 3 | Dying Declaration vs. Dying Deposition | Short Essay |
| 4 | Inquest - Police vs. Magistrate inquest | Short Essay |
| 5 | Medical Negligence - definition, types, defenses | Long Essay |
| 6 | Consent - types, valid consent, exceptions | Short Essay |
🟡 FREQUENTLY ASKED
| # | Topic | Type |
|---|---|---|
| 7 | Professional Misconduct | Short Essay |
| 8 | NMC - constitution, functions, disciplinary control | Long/Short Essay |
| 9 | Perjury | Short Note |
| 10 | MLC (Medico-Legal Case) - labelling, procedure | Short Essay |
| 11 | BNS / BNSS / BSA - new 2023 acts replacing IPC/CrPC/IEA | Short Note |
| 12 | Crime Scene Investigation - 6 W's, doctor's duties | Short Essay |
| 13 | Privileged Communication | Short Note |
| 14 | Professional Secrecy | Short Note |
| 15 | Vicarious Liability | Short Note |
🟢 SHORT NOTES (5–10 lines each)
| # | Topic |
|---|---|
| 1 | Cognizable vs. Non-cognizable offence |
| 2 | Perjury - definition + punishment (S.229 BNS) |
| 3 | Dying deposition |
| 4 | Hostile witness |
| 5 | Hearsay evidence |
| 6 | Subpoena / Summons |
| 7 | Chain of custody |
| 8 | Cross-examination |
| 9 | Res judicata |
| 10 | Dichotomy |
| 11 | False certificate - punishment (S.234 BNS) |
| 12 | Conduct money |
📌 KEY FACTS TO REMEMBER
COURTS HIERARCHY (Criminal)
━━━━━━━━━━━━━━━━━━━━━━━━━━
Supreme Court → High Court → Sessions Court
→ Chief Judicial Magistrate → 1st Class Magistrate
→ 2nd Class Magistrate
INQUEST TYPES
━━━━━━━━━━━━
Police Inquest → Suspicious/unnatural deaths (S.194 BNSS)
Magistrate Inquest → Mandatory for:
• Death in police custody
• Dowry death (within 5 yrs)
• Death in prison
• Rape victim death during treatment
• Exhumation
NEW ACTS (2023) - MUST KNOW
━━━━━━━━━━━━━━━━━━━━━━━━━━
IPC 1860 → BNS (Bharatiya Nyaya Sanhita)
CrPC 1973 → BNSS (Bharatiya Nagarika Suraksha Sanhita)
IEA 1872 → BSA (Bharatiya Sakshya Adhiniyam)
PERJURY
━━━━━━━
False evidence in court → S.229 BNS → Up to 7 years
False certificate → S.234 BNS
DYING DECLARATION vs DYING DEPOSITION
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Declaration → Not on oath, NOT cross-examined → Less weight
Deposition → On oath, cross-examined → More weight
Bottom line for models exam: Focus on Courts + powers, Expert witness, Dying declaration vs. deposition, Inquest types, and New 2023 Acts (BNS/BNSS/BSA). These 5 topics cover 90% of what gets asked from the legal procedure section.
Answer also
✅ Complete Answers - Legal Procedure Section
Forensic Medicine (Reddy's 36th Edition)
1. COURTS OF LAW IN INDIA
Criminal Courts (Hierarchy - Highest to Lowest)
| Court | Location | Powers |
|---|---|---|
| Supreme Court | New Delhi | Highest tribunal; purely appellate in criminal cases; its law is binding on all courts (Art.134) |
| High Court | State capital | Try any offence; pass any sentence authorized by law; confirms death sentence from Sessions Court; judges appointed by President of India |
| Sessions Court | District HQ | Established by State Govt; can try only cases committed by a Magistrate; can pass death sentence but needs HC confirmation |
| Asst. Sessions Court | - | Up to 10 years imprisonment + unlimited fine |
| Chief Judicial Magistrate | - | Up to 7 years imprisonment |
| 1st Class Magistrate | - | Up to 3 years + fine |
| 2nd Class Magistrate | - | Up to 1 year + fine |
- Sessions judges and magistrates are appointed by the High Court
- Life imprisonment (≥20 years) can be commuted to 14 years by appropriate government
- In metro cities (>1 million population), CJM and 1st class magistrate replaced as per BNSS 2023
- If convicted for two offences at one trial, double punishment can be given
- IPC 1860 → BNS (Bharatiya Nyaya Sanhita)
- CrPC 1973 → BNSS (Bharatiya Nagarika Suraksha Sanhita)
- IEA 1872 → BSA (Bharatiya Sakshya Adhiniyam)
2. INQUEST
Types: (1) Police Inquest (2) Magistrate's Inquest
(A) Police Inquest (S.194, BNSS / S.174 CrPC)
- Conducted by: Officer-in-charge of police station (not below rank of Head Constable)
- Also called: Investigating Officer (I.O)
- Done in presence of two or more respectable persons (panchas)
- Prepares: Inquest Report (Panchanama) - describes wounds, fractures, injuries
- Body sent for PM to nearest authorized govt doctor with dead body challan + copy of inquest
- Private institutions CANNOT conduct autopsy without State Govt permission
(B) Magistrate's Inquest (S.196, BNSS / S.176 CrPC)
- Dowry death (death of woman within 7 years of marriage)
- Death in police custody
- Death in prison/jail
- Exhumation
- Rape victim dying during treatment (or rape alleged during custody)
- Death in psychiatric hospital
3. WITNESS
Types: (1) Common Witness (2) Expert Witness
| Feature | Common Witness | Expert Witness |
|---|---|---|
| Also called | Witness of fact / occurrence witness | Medical/scientific witness |
| What he gives | Evidence of facts personally observed | Opinion based on specialized knowledge |
| Principle | "First-hand knowledge rule" | S.39, BSA |
| Leading questions | Not allowed in examination-in-chief | Allowed in cross-examination |
| Conduct money | Entitled | Not entitled (official duty) |
| Example | Person who saw an accident | Doctor, fingerprint expert, handwriting expert |
| Weight | Positive evidence | Only corroborative (opinion evidence) |
Conduct of Doctor in Witness Box:
- Take oath before giving evidence ("I do swear in the name of God...")
- Give answers based on "reasonable medical certainty"
- Should NOT be dogmatic; say findings are "consistent with" particular injury
- Leading questions are permissible only in cross-examination
- Cannot change opinion in court but can indicate other possibilities
- Completely immune from defamation for anything said in witness box
- If a question is based on a new fact, ask lawyer to break it into parts
- If asked about previous published statement that differs - "Medicine advances with times"
Order of Examination:
- Examination-in-chief (direct): By side that called the witness; no leading questions
- Cross-examination: By opposing counsel; leading questions ALLOWED; no time limit
- Re-examination: By original side; only on new matters raised in cross-examination
- Court questions: Judge may ask at any time
Hostile Witness:
4. DYING DECLARATION vs. DYING DEPOSITION
| Feature | Dying Declaration | Dying Deposition |
|---|---|---|
| Definition | Statement of a person who believes they are about to die | Statement of a person too ill to attend court but still alive |
| Recorded by | Magistrate / Doctor / Any person | Magistrate only |
| Oath | NOT on oath | On oath |
| Cross-examination | NOT cross-examined | Cross-examined |
| Legal basis | S.26, BSA (S.32 IEA) | S.351, BNSS (S.299 CrPC) |
| Type of evidence | Secondary evidence | Primary evidence |
| Weight in court | Less | More |
| When used | Person dying or feared to die | Person very ill, cannot attend court |
- Need not be in any particular form
- Can be verbal, written, or by signs/gestures
- Doctor's certificate that declarant was in fit state of mind is important
- Conviction CAN be based solely on dying declaration without corroboration
5. PERJURY
- Definition: Giving false evidence deliberately under oath in a judicial proceeding
- Punishment: Imprisonment up to 7 years + fine (S.229, BNS)
- False certificate by doctor: Punishable under S.234, BNS
- Refusing to take oath: Imprisonment up to 6 months or fine (S.213, BNS)
- A doctor who deliberately gives false evidence or false certificate is guilty of perjury
6. MEDICAL NEGLIGENCE
Types:
- Civil Negligence
- Criminal Negligence
- Corporate Negligence
- Contributory Negligence
4 D's of Negligence (Elements):
- Duty - Existence of duty of care
- Dereliction - Failure to maintain standard of care
- Direct causation - Failure must lead to damage (proximate cause)
- Damage - Foreseeable type of damage
Civil vs. Criminal Negligence:
| Feature | Civil Negligence | Criminal Negligence |
|---|---|---|
| Negligence | Simple absence of care | Gross negligence/incompetence |
| Litigation | Between two parties | Between State and doctor |
| Court | Civil Court | Criminal Court |
| Evidence | Strong evidence sufficient | Guilt beyond reasonable doubt |
| Punishment | Pay damages | Imprisonment ± fine |
| Consent | Good defense | NOT a defense |
Contributory Negligence:
- Failure to give accurate history
- Leaving hospital against advice
- Refusal to follow instructions
Defenses Against Medical Negligence:
- No duty owed to plaintiff
- Duty discharged per prevailing standards
- Misadventure (therapeutic/diagnostic/experimental)
- Error of judgement
- Contributory negligence
- Res judicata - If already decided in one court, cannot be contested again in another
- Limitation - Suit must be filed within 2 years of alleged negligence (3 years for contract breach)
Vicarious Liability ("Respondeat Superior - Let the Master Answer"):
- Principal doctor responsible for assistant's negligence
- Partners liable for each other's negligence
- Hospital responsible for employees' negligence
- Surgeon liable for swab/sponge left in patient
7. CONSENT
Types of Consent:
- Implied consent - Patient attends hospital, holds arm for injection (most common in routine practice)
- Informed express consent - Specifically stated; can be verbal or written
Rules of Consent:
- Consent needed for every medical examination
- Oral consent in presence of a disinterested third party (e.g., nurse)
- Written consent needed for operations, blood transfusion, collection of blood
- Consent should be free, voluntary, informed, direct, personal - no fraud/coercion
- Consent for ONE specific procedure - not a blanket permission
Consent in Special Situations:
| Situation | Rule |
|---|---|
| Emergency | Consent is implied (to save life) |
| Minor (below 12 yrs) | Consent of parent/guardian |
| Mentally ill | Consent of legal guardian |
| Intoxicated patient | Implied consent; treat to save life |
| Prisoner | Can be treated without consent in society's interest |
| Rape victim | Written consent MUST be obtained |
| Compulsory by law (e.g., vaccination) | Law provides consent |
Therapeutic Privilege:
8. NATIONAL MEDICAL COMMISSION (NMC)
- Established under NMC Act 2019; came into existence 25 September 2020
- Replaced Medical Council of India (MCI) (63 years old)
- Composition: 33 members - 1 Chairman + 10 ex-officio + 22 part-time members
- Appointed by Central Government on recommendation of Search Committee
4 Autonomous Boards under NMC:
- UGMEB (Under-Graduate Medical Education Board) - UG curriculum, recognition
- PGMEB (Post-Graduate Medical Education Board) - PG/super-specialty
- MARB (Medical Assessment and Rating Board) - assessment of colleges
- EMRB (Ethics and Medical Registration Board) - National Register of doctors, ethical conduct
Key Functions of NMC:
- Conducts NEET (admissions to UG/PG)
- Conducts NEXT (National Exit Test - final year MBBS + license exam)
- Grants license to Community Health Provider (CHP) - mid-level practitioner
- Regulates fees of 50% seats in private medical colleges
- Frames rules for professional ethics and etiquette
Disciplinary Control (EMRB):
- Maintains National Register of doctors
- Can issue warning notice, penal erasure from register
- Penal erasure = removal of doctor's name from register (for infamous conduct)
- Infamous conduct = conduct which would be considered disgraceful or dishonorable by registered medical practitioners of good repute
9. PROFESSIONAL SECRECY (CONFIDENTIALITY)
- The doctor is obliged to keep secret all information obtained about a patient during professional work
- Patient can sue doctor if disclosure was voluntary, caused harm, and not in public interest
When Secrecy CAN be Broken (Privileged Communication):
- Notifiable diseases (cholera, plague, AIDS, etc.) - report to public health authority
- Court summons - compelled to disclose by court order
- Gunshot/injury wounds - must report to police
- Criminal abortion - report to police
- Child abuse - must report
- Death certificate - cause of death must be stated
- When patient gives consent to disclose
10. PROFESSIONAL MISCONDUCT (INFAMOUS CONDUCT)
- Dichotomy (fee splitting) - sharing fee with another doctor for referring a patient
- Issuing false certificates
- Performing criminal abortion (unless legal MTP)
- Selling drugs/prescriptions for personal profit
- Advertising - except under NMC permitted circumstances
- Practicing under a fictitious name
- Claiming unrecognized degrees/qualifications
- Performing euthanasia (active)
- Alcohol/drug addiction affecting practice
- Sexual misconduct with patient
11. QUICK REFERENCE TABLES
Subpoena (Summons) - Key Points:
- A document compelling witness attendance under penalty
- Subpoena duces tectum - also requires bringing documents/records
- Issued in writing, signed by presiding officer, bears court seal
- Punishment for non-attendance (criminal case): Fine + imprisonment + warrant (S.208, BNS)
Important Sections to Remember:
| Section | Act | Topic |
|---|---|---|
| S.194 BNSS | BNSS | Police Inquest |
| S.196 BNSS | BNSS | Magistrate's Inquest |
| S.229 BNS | BNS | Perjury (up to 7 yrs) |
| S.234 BNS | BNS | False certificate |
| S.213 BNS | BNS | Refusing to take oath (6 months) |
| S.39 BSA | BSA | Expert witness |
| S.26 BSA | BSA | Dying declaration |
| S.351 BNSS | BNSS | Dying deposition |
| S.51 BNSS | BNSS | Medical examination of accused |
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) - K.S. Narayan Reddy
Professional secrecy answer 15 marks eassy ques
PROFESSIONAL SECRECY
15 Marks Essay Answer
INTRODUCTION
LEGAL BASIS
- Regulated by NMC (Professional Conduct) Regulations
- Any voluntary and harmful disclosure entitles the patient to sue the doctor for damages (mental suffering, shame, humiliation)
GENERAL RULES OF PROFESSIONAL SECRECY
-
A doctor must NOT discuss the illness of his patient with others without patient's consent.
-
Even if the patient is a major, the doctor should not disclose illness details to parents or relatives - even if they are paying the fees. However, if the patient is a minor or unsound mind, guardians/parents MUST be informed.
-
A doctor should NOT answer any enquiry by third parties (even near relatives) without the consent of the patient.
-
A doctor should NOT disclose information even when requested by a public or statutory body, except in case of notifiable diseases.
-
Husband and wife - facts about illness of one must NOT be disclosed to the other without consent of the concerned person.
-
In divorce and nullity cases - no information should be given without consent.
-
Government doctors are ALSO bound by professional secrecy, even when the patient is treated free of charge.
-
When a doctor examines a government servant on behalf of the government, he CANNOT disclose the illness to the government without patient's consent.
-
Master-servant relationship - a doctor examining a domestic servant at the request of the master must NOT disclose facts to the master without servant's consent, even though the master is paying.
-
Factory/firm medical officer must NOT disclose examination results to the employer without consent of the employee.
-
An undertrial prisoner has the right to not permit disclosure of his illness. However, a convicted prisoner has no such right - doctor can disclose to authorities.
-
In reporting a case in any medical journal, patient's identity must not be revealed from case notes or photographs.
-
In examination of a dead body, facts that may affect the reputation of the deceased or cause mental suffering to relatives must be kept confidential.
-
For life insurance examination - a doctor must NOT give information to an insurance company about a person who consulted him before, without patient's consent. For a dead person - only with consent of nearest relative.
-
Sex of unborn child detected on ultrasonography must NOT be disclosed (as per PCPNDT Act).
PRIVILEGED COMMUNICATION
- The communication must be made to a person having direct interest in it
- Doctor should first persuade the patient to consent before notifying authorities
- If done in good faith and in public interest - doctor is NOT liable for damages
The 10 Exceptions (When Secrecy Can Be Broken):
- If a syphilitic patient is about to marry - doctor must advise not to marry until cured
- If patient refuses - doctor can disclose the condition to the woman concerned or her parents
- Swimming pools should be prohibited to those having syphilis/gonorrhea
- Doctor can inform the warden of a hostel if a boarder is suffering from venereal disease
- Every person aware of a crime or intention to commit a crime must immediately inform the nearest Magistrate or police (Section 33, BNSS; Section 211, BNS)
- If a doctor treats a victim of gunshot wound, stab injuries, murder, assault, rape - he is BOUND to inform the police
- A doctor who knowingly omits to inform the police of an offence shall be punished with imprisonment up to 6 months (Section 239, BNS)
- A doctor CANNOT claim privilege in a court if the information about the patient's illness is relevant to the inquiry
- Doctor should appeal to the Judge before disclosing a professional secret
- If the court does not accept the plea, doctor may request to give answer in writing so the public does not hear it
- If denied, the doctor MUST answer to avoid contempt of court charges
- The doctor is protected from civil action for disclosing information demanded by the court
PHYSICIAN'S RESPONSIBILITY IN CRIMINAL MATTERS
-
A doctor who is aware of crimes such as murder, dacoity, or escape of prisoners is legally bound to report to the nearest Magistrate or police (Section 33, BNSS).
-
In cases of attempted suicide - the doctor is NOT legally bound to report to police while patient is alive. However, if the person dies, he MUST inform the police.
-
In cases of criminal abortion - the doctor must report to police.
-
In road traffic accidents and assault injuries - the doctor is obliged to give necessary medical aid and ensure the patient reaches a proper institution as early as possible.
SUMMARY TABLE
| Situation | Can Disclose? | Reason |
|---|---|---|
| Notifiable disease | ✅ YES | Statutory duty |
| Venereal disease before marriage | ✅ YES | Public/partner interest |
| Dangerous occupation (driver with epilepsy) | ✅ YES | Public safety |
| Court order | ✅ YES | Legal obligation |
| Suspected crime / gunshot wound | ✅ YES | S.33 BNSS duty |
| Insurance company | ❌ NO | Without patient consent |
| Near relatives (of a major patient) | ❌ NO | Requires patient consent |
| Husband to wife / wife to husband | ❌ NO | Requires individual consent |
| Employer (without patient consent) | ❌ NO | Unless safety risk |
| Medical journal | ❌ NO | Identity must be protected |
| Sex of unborn child (USG) | ❌ NO | PCPNDT Act |
CONCLUSION
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) - K.S. Narayan Reddy, Chapter 3 (Medical Jurisprudence)
Professional misconduct
PROFESSIONAL MISCONDUCT
(Infamous Conduct in Professional Respect)
Complete Essay Answer - Reddy's 36th Edition
DEFINITION
DISCIPLINARY CONTROL (FM10.5)
- Issuing a Warning Notice - to a practitioner found guilty of professional misconduct
- Penal Erasure - permanently or temporarily removing the name from the medical register
- Restoration of the name after the period of punishment
Judicial Procedure on Complaint:
- Complaint received → submitted to Council President
- Referred to Sub-committee/Executive Committee
- If prima facie case exists → notice issued to the practitioner
- Hearing held - both complainant and practitioner must be present
- After evidence → majority vote decides guilt
- Second vote decides: Warning Notice or Name Removed from Register
- Deletion is published widely in local press and medical associations so the practitioner cannot practice
ERASURE FROM MEDICAL REGISTER
- Death of the registered practitioner
- Error or fraud in entry
- Penal Erasure - for serious professional misconduct
Penal erasure is called the "professional death sentence" - it deprives the practitioner of ALL privileges of a registered practitioner.
ACTS CONSTITUTING PROFESSIONAL MISCONDUCT
1. Improper Conduct with a Patient
- Maintaining an improper personal/sexual association with a patient
- Adultery arising out of professional relationship
2. Conviction by a Court of Law
- For offences involving moral turpitude or criminal acts
3. Issuing False or Misleading Certificates
- False certificates for sickness benefit, insurance, passport, attendance in court, public services, etc.
- Issuing certificates of efficiency to unqualified or non-medical persons
4. Drug-Related Violations
- Prescribing steroids or psychotropic drugs without absolute medical indication
- Selling Schedule H and I drugs and poisons to the public (except to his own patients)
- Contravening the Drugs and Cosmetics Act
5. Running an Open Shop
- Running a shop for sale of medicines
- Dispensing prescriptions of other doctors for commercial purposes
- Manufacturing or selling proprietary medicines whose formulae are not displayed on the label
6. Advertising (Improper)
- Writing in lay press or giving interviews that advertise himself or solicit practice
- Advertising through manufacturing firms directly or indirectly
- (Exception: He MAY write on matters of public health, hygienic living, or give talks on radio/TV/internet in public interest)
- An institution (nursing home, maternity home) may be advertised but with limited details only (name, type of patients, facilities, fees)
- Announcing start/change/resumption of practice is allowed but not more than twice
7. Signboard Violations
- Using an unusually large signboard
- Writing anything other than: name, qualifications, specialty, registration number
- Affixing signboard at a chemist's shop or a place where he does not reside or work
8. Dichotomy (Fee-Splitting)
- Receiving or giving commission to a professional colleague, manufacturer, trader in drugs, chemist, dentist, etc., for referring patients
- This is called dichotomy - one of the most serious forms of misconduct
9. Covering
- Assisting an unqualified person to attend, treat, or operate on a patient in matters requiring professional skill
- (Exception: Proper training of bona fide students, midwives, dispensers, surgical attendants under personal supervision is allowed)
10. Association with Manufacturing Firms
- Having personal ownership in patents for drugs, instruments used in medicine/surgery
- Asking or receiving rebates or commission from prescribing therapeutic agents
- Writing prescriptions in private formulae that only he or a specific pharmacy can read
11. Disclosing Patient's Secrets
- Disclosing professional secrets except:
- Under court order by the presiding judge
- Serious and identified risk to a specific person/community
- Notifiable diseases
12. Failure to Obtain Consent
- Failing to obtain informed consent from the patient before an operation
- Failing to obtain consent from guardians for a minor patient
- Failing to obtain consent of both husband and wife for an operation that may result in sterility
13. Publishing Patient Information
- Publishing photographs or case reports of patients in any form by which their identity can be made out, without their permission
14. Refusal on Religious Grounds
- Refusing on religious grounds alone to perform: sterility procedures, birth control, circumcision, or MTP when there is medical indication - unless the doctor feels personally incompetent
15. Using Touts or Agents
- Using touts or agents to procure patients
- This is unethical canvassing of patients
16. Practicing Under a Fictitious Name
- Practicing or assisting in practice under a fictitious name
17. Claiming False Specialization
- Claiming to be a specialist without having special qualification in that branch
18. Drunk and Disorderly
- Being drunk and disorderly so as to interfere with proper skilled practice of medicine
19. Violation of Laws
- Not assisting in upholding the laws of the country in regulating medical practice
- Assisting others to evade such laws
20. Non-Maintenance of Medical Records
- Not maintaining indoor patient records for a minimum period of 3 years
- Refusing to provide records within 72 hours of a request by patient or authorized representative
21. Not Displaying Registration Number
- Failure to display the registration number issued by State Medical Council on clinic, prescriptions, and certificates
22. Sex Determination for Female Feticide
- Undertaking sex determination tests with the intent to terminate normal female fetus
- This amounts to female feticide and is a crime under the PCPNDT Act
23. IVF/Artificial Insemination Without Consent
- Performing IVF or AI without written informed consent of the female patient, her spouse, and the donor
24. Violation of ICMR Research Guidelines
- Conducting clinical drug trials or research on humans/animals without following ICMR ethical guidelines
THE MOST SERIOUS MISCONDUCTS - "THE 6 A's"
| # | "A" | Meaning |
|---|---|---|
| 1 | Adultery | Improper relationship with patient |
| 2 | Advertising | Self-promotion/canvassing |
| 3 | Abortion | Unlawful criminal abortion |
| 4 | Association | With unqualified persons in professional matters (Covering) |
| 5 | Addiction | To drugs |
| 6 | Alcohol | Consumption at workplace |
PROFESSIONAL NEGLIGENCE vs. INFAMOUS CONDUCT
| Feature | Professional Negligence | Infamous Conduct |
|---|---|---|
| Definition | Absence of care and skill / willful negligence | Violation of Code of Medical Ethics |
| Duty of care | Must be present | Need NOT be present |
| Damage to person | Must be present | Need NOT be present |
| Trial by | Courts (civil or criminal) | State Medical Council |
| Punishment | Fine or Imprisonment | Erasure of name or Warning |
| Appeal | To higher Court | To State and Central Governments |
RIGHTS OF REGISTERED MEDICAL PRACTITIONERS
- Right to practice medicine
- Right to choose a patient
- Right to dispense medicines
- Right to possess and supply dangerous drugs to patients
- Right to add titles and descriptions to their name
- Right to recovery of fees
- Right for appointment to public hospitals
- Right to issue medical certificates
- Right to give evidence as an expert witness
PRECAUTIONS FOR A DOCTOR TO AVOID NEGLIGENCE CHARGES
- Obtain informed written consent
- Maintain full, accurate, legible medical records
- Do sensitivity tests before injections likely to cause anaphylaxis
- Never examine a female patient without a third person present
- Never guarantee a cure
- Do not criticize or condemn another doctor in front of the patient
- Do not make statements admitting fault
- Seek consultation when appropriate
- Keep yourself updated with technical advances
- Never practice "defense by denial" (claiming the patient is not yours = abandonment)
CONCLUSION
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) - K.S. Narayan Reddy, Chapter 3 (Medical Jurisprudence - FM10.5)
Most important topics for eassy from whole book
⭐ MOST IMPORTANT ESSAY TOPICS
Whole Book - Reddy's Forensic Medicine 36th Edition
MBBS Model/University Examination
🔴 TIER 1 - MUST WRITE (Highest Frequency - Almost Always Asked)
| # | Topic | Chapter | Marks |
|---|---|---|---|
| 1 | Medical Negligence - definition, types (civil/criminal/contributory/corporate), 4D's, defenses | Ch. 3 | 15 |
| 2 | Rigor Mortis - mechanism, stages, factors affecting, cadaveric spasm, heat stiffening | Ch. 7 | 15 |
| 3 | Mechanical Asphyxia - types, pathophysiology, PM findings, hanging vs strangulation | Ch. 13 | 15 |
| 4 | Identification - bones, teeth, age, hair, Gustafson's method, fingerprints | Ch. 4 | 15 |
| 5 | Rape - definition, examination of victim, evidence collection, materials sent to lab | Ch. 16 | 15 |
| 6 | Organophosphorus Poisoning - mechanism, clinical features, PM findings, treatment, PAM | Tox | 15 |
| 7 | Postmortem Changes - classification, early/late, time since death estimation | Ch. 7 | 15 |
| 8 | Mechanical Injuries - classification, abrasions, contusions, lacerations, stab, incised | Ch. 8 | 15 |
🟠 TIER 2 - VERY IMPORTANT (Asked Frequently)
| # | Topic | Chapter | Marks |
|---|---|---|---|
| 9 | Professional Secrecy - rules, privileged communication, exceptions | Ch. 3 | 10-15 |
| 10 | Professional Misconduct - 6 A's, Warning Notice, Penal Erasure, NMC | Ch. 3 | 10-15 |
| 11 | Consent - types, informed consent, rules, special situations | Ch. 3 | 10 |
| 12 | NMC - constitution, functions, 4 boards, disciplinary control | Ch. 3 | 10 |
| 13 | Courts of Law - hierarchy, powers of each court | Ch. 2 | 10 |
| 14 | Thermal Deaths - burns, heat stroke, hypothermia, electrocution | Ch. 12 | 15 |
| 15 | Criminal Abortion - methods, causes of death (immediate/delayed/remote), PM findings | Ch. 17 | 15 |
| 16 | Infanticide - definition, methods, live birth vs stillbirth, viability | Ch. 18 | 15 |
| 17 | Postmortem Examination - prerequisites, incisions, organ removal techniques | Ch. 5 | 10 |
| 18 | Corrosive Acid Poisoning - H₂SO₄/HCl/HNO₃, features, PM findings, treatment | Tox | 15 |
| 19 | Carbon Monoxide Poisoning - mechanism, features, cherry-red lividity, treatment | Tox | 10 |
| 20 | Regional Head Injuries - types, coup-contrecoup, intracranial hemorrhages, PM findings | Ch. 9 | 15 |
🟡 TIER 3 - IMPORTANT (Frequently Asked as 10-mark Essays)
| # | Topic | Chapter |
|---|---|---|
| 21 | Starvation - stages, clinical features, PM findings, medico-legal importance | Ch. 11 |
| 22 | Drowning - wet vs dry, PM findings, diatom test, Gettler test | Ch. 13 |
| 23 | Firearm Injuries - entry vs exit wound, contact/near/distant range, medico-legal aspects | Ch. 10 |
| 24 | Cut-throat Injuries - suicidal vs homicidal differences, PM findings | Ch. 8 |
| 25 | Blood Stain Examination - confirmatory tests, Kastle-Meyer, precipitin, serological | Ch. 19 |
| 26 | Impotence and Sterility - causes in male and female | Ch. 15 |
| 27 | Anesthetic Deaths - causes, malignant hyperthermia, PM findings | Ch. 14 |
| 28 | Arsenic Poisoning - acute/chronic, Mees' lines, PM findings, treatment | Tox |
| 29 | Alcohol Poisoning - ethyl vs methyl, medico-legal aspects | Tox |
| 30 | Alkali Poisoning - features, PM findings, treatment | Tox |
| 31 | General Management of Acute Poisoning - gastric lavage, antidotes, supportive care | Tox |
| 32 | Expert Witness - vs common witness, conduct in court, examination order | Ch. 2 |
| 33 | Inquest - police vs magistrate, mandatory cases | Ch. 2 |
📌 TOPIC-WISE CHAPTER MAP
SECTION 1: FORENSIC MEDICINE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Ch. 1 Introduction/Ethics
→ Ethical principles (beneficence, autonomy)
Ch. 2 Legal Procedure
→ Courts of Law ★★★
→ Inquest ★★
→ Expert Witness ★★★
→ Dying Declaration vs Deposition ★★
Ch. 3 Medical Jurisprudence
→ Medical Negligence ★★★★★
→ Professional Secrecy ★★★★
→ Professional Misconduct ★★★★
→ Consent ★★★★
→ NMC ★★★
Ch. 4 Identification
→ Identification (bones/teeth/age) ★★★★★
→ Dactylography ★★
→ Gustafson's method ★★
Ch. 5 Autopsy
→ Postmortem Examination ★★★
Ch. 6 Death & Thanatology
→ Brain Death criteria ★★
Ch. 7 Postmortem Changes
→ Rigor Mortis ★★★★★
→ Postmortem Changes/TSD ★★★★★
Ch. 8 Mechanical Injuries
→ Classification of injuries ★★★★★
→ Cut-throat injuries ★★★
→ Firearm injuries ★★★
Ch. 9 Regional Injuries
→ Head injuries ★★★★
Ch. 10 Firearm injuries
→ Entry/exit wounds ★★★
Ch. 11 Starvation
→ Starvation ★★★
Ch. 12 Thermal Injuries
→ Burns/Heat stroke/Hypothermia ★★★★
Ch. 13 Mechanical Asphyxia
→ Asphyxia ★★★★★
→ Hanging/Strangulation ★★★★
→ Drowning ★★★
Ch. 14 Anesthetic Deaths
→ Anesthetic deaths ★★
Ch. 15 Impotence/Sterility
→ Impotence & Sterility ★★
Ch. 16 Sexual Offences
→ Rape ★★★★★
→ POCSO ★★
Ch. 17 Abortion
→ Criminal Abortion ★★★★
Ch. 18 Infanticide
→ Infanticide ★★★★
→ Live birth vs Stillbirth ★★★
Ch. 19 Forensic Biology
→ Blood stain examination ★★
Ch. 20 Postmortem Artefacts
→ PM Artefacts ★★
SECTION 2: TOXICOLOGY
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
General Toxicology
→ Acute poisoning management ★★★★
Specific Poisons
→ OP Poisoning ★★★★★
→ Corrosive Acid ★★★★
→ CO Poisoning ★★★★
→ Arsenic ★★★
→ Alcohol ★★★
→ Alkali ★★★
→ Dhatura/Belladonna ★★
→ Barbiturates ★★
→ Lead ★★
→ Cyanide ★★
→ Snake bite ★★
🎯 TOP 10 TOPICS IF YOU HAVE LIMITED TIME
1. Medical Negligence (Forensic - Ch.3)
2. Rigor Mortis (Forensic - Ch.7)
3. Mechanical Asphyxia (Forensic - Ch.13)
4. Rape - Examination (Forensic - Ch.16)
5. Identification (Forensic - Ch.4)
6. Mechanical Injuries (Forensic - Ch.8)
7. Professional Misconduct (Forensic - Ch.3)
8. OP Compound Poisoning (Toxicology)
9. Corrosive Acid Poisoning (Toxicology)
10. Criminal Abortion (Forensic - Ch.17)
These 10 topics, if prepared thoroughly, will cover approximately 70-80% of the essay marks in any MBBS Forensic Medicine model examination.
Rigor mortis
RIGOR MORTIS
Complete 15-Mark Essay Answer
INTRODUCTION - MUSCULAR CHANGES AFTER DEATH
- Primary Relaxation (Flaccidity) - 1 to 2 hours after death
- Rigor Mortis (Cadaveric Rigidity) - stiffening phase
- Secondary Flaccidity - resolution phase
STAGE 1: PRIMARY FLACCIDITY
- Lasts 1 to 2 hours after somatic death (only cellular death has not occurred yet)
- All muscles begin to relax - lower jaw falls, eyelids lose tension, joints flexible
- Body flattens over areas in contact with surface (contact flattening)
- Muscles are relaxed as long as ATP content is sufficiently high
- Muscular irritability to mechanical/electrical stimuli still persists
- Peristalsis, ciliary movements, WBC movements may continue
- Pupils react to atropine or physostigmine but NOT to light
- Muscle protoplasm is slightly alkaline
STAGE 2: RIGOR MORTIS
Definition
MECHANISM
- Actin filaments (thin)
- Myosin filaments (thick)
- Together they form a loose combination called actomyosin
- ATP energy keeps actin and myosin filaments separated (relaxed state)
- Nerve impulse → ATPase released → actin and myosin interlock → muscle contracts
- ATP is continuously resynthesized via glycogen → lactic acid pathway
- Lactic acid enters blood → reconverted to glycogen in liver
- After somatic death, there is no resynthesis of ATP
- ATP is progressively and irreversibly destroyed (dephosphorylation + deamination)
- Loss of integrity of sarcoplasmic reticulum → calcium ions flood the sarcomeres
- Calcium causes binding of actin and myosin → mimics normal contraction
- Normal relaxation requires ATP-driven calcium pumping back across SR membrane - this FAILS after death
- When ATP is reduced to critical level (85% of normal) → actin and myosin combine as a rigid actomyosin complex → stiffness
- Maximum rigidity when ATP is at 15% and lactic acid is 0.3%
- Actin-myosin complex is trapped in contraction until disrupted by putrefaction
Death → No ATP → Calcium floods sarcomere → Actin-Myosin lock permanently → Rigor Mortis
ORDER OF APPEARANCE (Nysten's Rule)
- Involuntary muscles first - myocardium becomes rigid within 1 hour
- Skeletal muscles - begins in:
- Eyelids → Neck → Lower jaw → Face → Chest → Upper limbs → Abdomen → Lower limbs → Fingers and toes (downward progression)
- Disappears in the same order in which it appeared
Nysten's Rule: Rigor mortis appears first in the muscles of mastication, then descends downward through the body.
FEATURES OF ESTABLISHED RIGOR MORTIS
- Entire body is stiff, hard, opaque
- Muscles are shortened
- Knees, hips, shoulders, elbows are slightly flexed
- Fingers and toes show marked flexion
- Cutis anserina (goose skin) - rigor of erector pili muscles → roughness and elevation of skin hairs
- Rigor of dartos muscle (scrotum) → compresses testes → postmortem extrusion of semen from urethra
- Pupils may be partially contracted
- Rarely, rigor of gravid uterus may expel the fetus (coffin birth)
DEMONSTRATION OF RIGOR MORTIS
- Trying to lift the eyelids
- Depressing the jaw
- Gently bending the neck and various joints
TIME OF ONSET AND DURATION
| Condition | Onset | Duration |
|---|---|---|
| India (summer) | 1-2 hours after death; well-established in 6 hours | 18-36 hours |
| India (winter) | Slower onset | 24-48 hours |
| Temperate countries | 3-6 hours onset | 2-3 days |
Rule of 12 (begins in 12 hrs, complete in 12 hrs, disappears in 12 hrs) is NOT applicable in tropical countries like India.
FACTORS AFFECTING RIGOR MORTIS
| Factor | Early + Short Rigor | Late + Long Rigor |
|---|---|---|
| Age | Children, old people (feeble and rapid) | Healthy adults (slow, well-marked, long) |
| Nature of death | Exhausting diseases (cholera, typhoid, TB, cancer), violent deaths (cut-throat, firearms), OP poisoning | Asphyxia, severe hemorrhage, apoplexy, pneumonia, paralytic disease |
| Exercise before death | Fatigue/exhaustion/convulsions (early, short) | Muscles at rest before death (slow, long) |
| Temperature | Hot environment (early onset, short) | Cold environment (delayed, prolonged) |
| Special poisons | HCN, strychnine - early onset, persists longer | CO poisoning - delays disappearance |
| Infection | Gas gangrene, septicemia - absent or very short | - |
| Stillborn infants | Rigor commonly found at full term | - |
EFFECTS OF RIGOR ON ORGANS (Autopsy significance)
- Heart - rigor causes ventricles to contract → may be mistaken for left ventricular hypertrophy (exclude by measuring weight and wall thickness)
- Secondary flaccidity → atrial/ventricular distension → should NOT be mistaken for antemortem dilatation or myocardial degeneration
- Face - muscle relaxation then fixation → grimacing appearance → does NOT indicate fear or fright at time of death
MEDICOLEGAL IMPORTANCE OF RIGOR MORTIS
- Sign of death - confirms that death has occurred
- Estimation of time of death (not very reliable due to variable factors)
- Indicates position of body at time of death - if body is found with legs raised in the air but rigor is fixed in that position, it indicates the body was moved after full rigor developed elsewhere
- Helps determine whether body was moved after death
- In cadaveric spasm - indicates the last act of the person at death (e.g., weapon in hand)
STAGE 3: SECONDARY RELAXATION (SECONDARY FLACCIDITY)
CONDITIONS SIMULATING RIGOR MORTIS (Differential Diagnosis)
1. Heat Stiffening
- Exposure to temperature above 65°C
- Proteins denatured and coagulated (like cooking)
- Muscles contracted, desiccated or carbonized
- Zone of brownish-pink "cooked meat" under the surface
- CANNOT be broken down by extending limbs (unlike rigor mortis)
- Seen in: burns, high-voltage electrocution, falling into hot liquid
- Normal rigor mortis does NOT occur subsequently
2. Cold Stiffening
- Exposure to -5°C or lower (freezing temperatures)
- Body fluids freeze, subcutaneous fat solidifies → simulates rigor
- When joints forcibly flexed → ice breaks in synovial fluid with sharp sound
- When body placed in warm atmosphere → stiffness disappears → then normal rigor occurs rapidly and passes off quickly
- Hardening of subcutaneous fat in infants may simulate ligature marks
3. Cadaveric Spasm (Instantaneous Rigor)
- Rare condition
- Preserves exact attitude of person at moment of death for several hours
- Usually limited to one group of voluntary muscles (most often the hands)
- Occasionally whole body (soldiers shot in battle)
- Very great force required to overcome stiffness
- Passes without interruption into normal rigor mortis
RIGOR MORTIS vs. CADAVERIC SPASM
| Feature | Rigor Mortis | Cadaveric Spasm |
|---|---|---|
| Onset | After primary flaccidity (1-2 hrs) | Immediately at moment of death |
| Muscles involved | All voluntary + involuntary muscles | One group of voluntary muscles |
| Preceded by | Primary flaccidity | NO primary flaccidity |
| Mechanism | Chemical (ATP depletion) | Possibly neurogenic |
| Can be simulated | No (after death) | Cannot be simulated after death |
| Medicolegal importance | Time of death, position of body | Weapon in hand = suicide evidence |
| Broken by force? | Yes (temporarily, reforms) | Very great force required |
MEDICOLEGAL IMPORTANCE OF CADAVERIC SPASM
- Suicide evidence - weapon (pistol or knife) firmly grasped in victim's hand = strong presumptive evidence of suicide. Murder CANNOT replicate this exact grip
- Assault evidence - clothing, button of assailant, or hair may be firmly grasped in hands
- Drowning evidence - grass, weeds, or leaves found firmly grasped = victim was alive on entering water (not thrown in dead)
SUMMARY DIAGRAM
DEATH
↓
PRIMARY FLACCIDITY (1-2 hrs)
- ATP still present, muscles relaxed
↓
RIGOR MORTIS (begins 1-2 hrs → full in 6 hrs in India)
- ATP depleted → Ca²⁺ floods sarcomere → Actin-Myosin lock
- Order: Involuntary first → Face → Neck → Chest → Arms → Legs
- Duration: 18-36 hrs (summer), 24-48 hrs (winter) in India
↓
SECONDARY FLACCIDITY
- Putrefaction → alkaline products → actomyosin complex breaks down
CONDITIONS SIMULATING RIGOR:
├─ Heat Stiffening (>65°C) - cannot be broken
├─ Cold Stiffening (<-5°C) - freezing of fluids
└─ Cadaveric Spasm - instantaneous, neurogenic, MOST ML important
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) - K.S. Narayan Reddy, Chapter 7 (Postmortem Changes - FM2.5, FM2.7, FM2.8)
Identification
IDENTIFICATION
Complete 15-Mark Essay Answer
DEFINITION
- Complete identification - all characteristics are known
- Partial/incomplete identification - only some facts are determined (e.g., race, age, sex, stature) while others remain unknown
SCOPE OF IDENTIFICATION
- Living people
- Recently dead persons
- Decomposed bodies
- Mutilated and burnt bodies
- Skeletal remains
IMPORTANCE (Civil vs. Criminal)
- Accused in assault, murder, rape cases
- Newborns fraudulently switched in hospitals
- Impersonation
- Missing persons investigations
- Marriage, inheritance, passport
- Insurance claims, disputed sex
- Missing persons
Rule: At least two identification marks must be noted by the doctor in all medicolegal cases. Sex, age, and stature are the primary characteristics of identification.
CORPUS DELICTI
- Latin: "body of the crime"
- Principle that a crime must be proven to have occurred before an individual can be convicted
- The prosecution must have enough evidence showing the essential parts of a crime occurred before charging an individual
IDENTIFICATION DATA (14 Parameters)
- Race and religion
- Sex
- Age
- General development and stature
- Complexion and features
- External peculiarities - moles, birthmarks, malformations, scars, tattoo marks, wounds, occupation marks
- Anthropometric measurements
- Fingerprints and footprints
- Teeth
- Personal effects - clothes, pocket contents, jewellery
- Handwriting
- Speech and voice
- Gait, tricks of manner and habit
- Memory and education
No single feature is reliable alone - a combination of features is always used.
A. DETERMINATION OF RACE
- Complexion - Indians (brown), Europeans (fair), Negroes (black) - limited value
- Skull shape - Caucasoid (oval), Negroid (long), Mongoloid (round)
- Nasal aperture - narrow/high (Caucasoid), broad/low (Negroid)
- Hair - straight/wavy (Caucasoid), tightly curled (Negroid), straight/coarse (Mongoloid)
- Facial features - prognathism, orbital shape, zygomatic arch prominence
B. DETERMINATION OF SEX
From General Physical Features (Table)
| Feature | Male | Female |
|---|---|---|
| Build | Larger, greater muscle | Smaller, less muscle |
| Shoulders | Broader than hips | Narrower than hips |
| Waist | Ill-defined | Well-defined |
| Limbs | Longer | Shorter |
| Thorax | Larger dimensions | Shorter, rounded |
| Gonads | Functioning testis | Functioning ovary |
Sex Chromatin Analysis (Barr Body Test)
- Normal: Males = 46, XY; Females = 46, XX
- Buccal smear test (Barr body):
- Males: 0-4% of nuclei contain chromatin bodies
- Females: 20-80% of nuclei contain chromatin bodies
- Davidson body - drumstick-shaped nuclear attachment in neutrophils in ~3% of nucleated cells in females; absent in males
Sex from Skeletal Remains
- Recognizable sex differences in skeleton appear after puberty (except pelvis)
- Pelvis is the most reliable bone - accuracy 75-80% for sex
- Without pelvis, accuracy drops to ~50%
| Bone | Male | Female |
|---|---|---|
| Skull capacity | 1500-1550 ml | 1350-1400 ml |
| Skull general | Larger, rugged, muscle ridges marked | Smaller, smoother, lighter |
| Forehead | Sloping | Vertical, rounded |
| Supraorbital ridges | Prominent | Less prominent |
| Orbits | Square, lower, smaller | Rounded, higher, larger |
| Skeleton weight | 4.5 kg | 2.75 kg |
| Pelvis | Narrower, heart-shaped inlet | Wider, oval inlet |
| Long bones | 8% longer, ridges prominent | Shorter, smoother |
C. DETERMINATION OF AGE
- General physical features
- Teeth (most reliable)
- Ossification of bones
- Secondary sex characters
- General development (in children)
1. TEETH IN AGE ESTIMATION
Temporary (Deciduous/Milk) Teeth:
- Total: 20 teeth (4 incisors, 2 canines, 4 molars in each jaw)
- All deciduous teeth are complete by about 2.5 years
- Between 7 to 12 years - mixed dentition (24 teeth present, both deciduous falling and permanent erupting)
Permanent Teeth:
- Total: 32 teeth
- First permanent molar ("6-year molar") erupts at 6-7 years
| Tooth | Age (years) |
|---|---|
| 1st molar (6-year molar) | 6-7 |
| Central incisor | 7-8 |
| Lateral incisor | 8-9 |
| Canine | 11-12 |
| 1st premolar | 10-11 |
| 2nd premolar | 11-12 |
| 2nd molar (12-year molar) | 12-13 |
| 3rd molar (Wisdom tooth) | 17-25 |
GUSTAFSON'S METHOD (Age from Teeth in Adults >21 years)
| Letter | Change | Description |
|---|---|---|
| A | Attrition | Wear of occlusal surface - enamel → dentin → pulp exposed in old age |
| P | Periodontosis | Regression of gums, exposure of root necks, loose teeth |
| S | Secondary dentin | Deposition within pulp cavity, reduces cavity size; extends to apex |
| R | Root resorption | Absorption of cementum and dentin from apex upwards |
| T | Transparency of root | Most reliable criterion; begins after 30 years; dentinal canals fill with mineral → translucent |
| C | Cementum apposition | Thickening of cementum especially near the root end |
- Anterior teeth are most suitable (incisors > premolars)
- 3rd molar is unsuitable
- Changes are absent at 15 years of age
- Total score used to calculate age from a regression formula
2. OSSIFICATION OF BONES (Age from Bones)
- Based on appearance of ossification centers and union of epiphyses
| Structure | Age |
|---|---|
| Elbow (capitulum) | 1 year |
| Femoral head | 1 year |
| Triradiate cartilage of pelvis closes | 15-16 years |
| Medial end of clavicle fuses | 22-25 years (last to fuse) |
| Vertebral ring epiphysis fuses | 25 years |
| Coronal suture closes | 30-40 years |
| Sagittal suture closes | 22 years |
| Lambdoid suture closes | 26 years |
| All sutures closed | >50 years |
3. SECONDARY SEX CHARACTERS IN AGE ESTIMATION
- 13-14 years: pubic hair appears, testes enlarge, penis begins to enlarge
- 15 years: axillary hair begins
- 16 years: genitals adult appearance
- 16-18 years: facial hair, voice deepens
- 12-13 years: breast development, pubic hair
- 14-15 years: axillary hair, menstruation starts
4. OTHER AGE-RELATED CHANGES
- Arcus senilis - grey opaque ring around cornea margin; appears after 50 years (if in young adults <40 yrs = hyperlipidaemia = "arcus juveniles")
- Greying of hair - scalp after 40 years; pubic hair NOT grey before 50-55 years
- Loss of collagenous stroma in bone - bone becomes lighter
- Skin changes - loss of elasticity, wrinkling (old age)
- Limitation: Age estimation becomes unreliable after 25 years
MEDICOLEGAL IMPORTANCE OF AGE (Age 18 is the most important)
| Age | Legal significance |
|---|---|
| Under 7 years | NO criminal responsibility (S.20, BNS) |
| 7-12 years | Criminal responsibility if "sufficient maturity" |
| Under 12 years | Cannot give valid consent to harm |
| Under 16 (boys), Under 18 (girls) | Kidnapping from lawful guardianship |
| Under 18 years | Juvenile - no death penalty, no life imprisonment |
| 18 years | Can give valid consent; marriage; voting; rape (sex with girl <18 = rape even with consent) |
| 16-18 yrs (heinous offence) | Tried as adults (no death penalty/life term) |
| 21 years | Can be tried for dowry |
D. STATURE (HEIGHT) ESTIMATION
- Stature varies by 1.5-2 cm at different times of day (less in evening)
- After death, body lengthens by ~2 cm (loss of muscle tone)
- After 30 years - decreases by 0.6 mm/year (disc degeneration)
- Arm span (fingertip to fingertip) ≈ height
- Vertex to symphysis pubis = half of stature (after 14 years)
- Head height = 1/7 of stature; skull length = 1/8 of stature
- Max foot length ÷ 0.15 = stature
E. DACTYLOGRAPHY (Fingerprint System)
- First used in India: Sir William Herschel (1858) in West Bengal
- Systematized by: Sir Francis Galton (1892)
- First fingerprint bureau: Kolkata
- Current system: Galton-Henry System
Principle:
Classification of Fingerprints:
- Loops (60-70%) - radial, ulnar
- Whorls (25-35%) - concentric, spiral, double spiral, almond
- Arches (6-7%) - plain, tented, exceptional
- Composites (1-2%) - central/lateral pocket loops, twinned loops, accidentals
Properties of Fingerprints (Why reliable):
- Permanent - unchanged throughout life
- Individual - 1 in 64 billion chance of two persons having identical fingerprints (Quetlet's rule)
- Ridge patterns develop in utero and never change unless destroyed by deep injury (but they regenerate exactly)
- Minimum 16 points of comparison needed for positive identification (as per Supreme Court ruling)
Poroscopy (Henry Locard):
- Study of pores on fingertip ridges (mouths of sweat gland ducts)
- Each mm of ridge = 9-18 pores
- Pores are permanent, vary in size/shape/position in everyone
- Useful when only fragments of fingerprints are available (no specific pattern)
F. HAIR IN IDENTIFICATION
- Humans: < 0.3
- Animals: > 0.5
| Feature | Human Hair | Animal Hair |
|---|---|---|
| Character | Fine, thin | Coarse, thick |
| Cuticle scales | Short, broad, thin, irregularly annular | Very large, step-like/wavy |
| Cortex | Thick, 4-10× as broad as medulla | Thin, rarely >2× medulla |
| Medulla | Narrow, fragmented or absent | Continuous, wider |
| Pigment | Evenly distributed in cortex | Mostly in medulla |
| Banding | Absent | Present (color changes along shaft) |
G. ANTHROPOMETRY (Bertillon System)
- Principle: After 21 years, skeletal dimensions remain unchanged; ratio of dimensions varies in different individuals
- Records: body appearance, body marks (moles, scars, tattoos), 11 body measurements
- Replaced by dactylography (fingerprints) as it is more reliable
H. SCARS AND TATTOO MARKS
- Scars - permanent; shape, site, color, surface, tenderness noted
- Tattoo marks - permanent; color, design, size, situation noted
- Sydney Shark Arm Case (1935) - arm from shark's stomach identified by tattoo mark - led to solving a murder
SUMMARY TABLE - IDENTIFICATION AT A GLANCE
IDENTIFICATION
├── RACE → Complexion, skull shape, hair, nasal aperture
├── SEX → Physical features, Barr body, Davidson body, Skeleton
├── AGE → Teeth (Gustafson's), Bones (ossification centers),
│ Secondary sex characters, Arcus senilis
├── STATURE → Long bone formulas, arm span, foot length
└── PERSONAL IDENTITY
├── FINGERPRINTS (Dactylography) - Loops/Whorls/Arches/Composites
├── POROSCOPY - Fragment fingerprints
├── HAIR - Medullary index, species identification
├── TEETH - Dental records, bite marks
├── SCARS & TATTOOS
└── ANTHROPOMETRY (Bertillon - replaced by dactylography)
Source: The Essentials of Forensic Medicine and Toxicology, 36th Edition (2026) - K.S. Narayan Reddy, Chapter 4 (FM4.1 to FM4.4)
Rape
Rape
Generate a comprehensive Word document with Rape essay, questions and answers
Rigor mortis easy mechanism of action
RIGOR MORTIS - Mechanism Made Easy
THE SIMPLE CONCEPT
During life, muscles need ATP to RELAX. When ATP runs out after death, muscles get permanently LOCKED in contraction = Rigor Mortis
STEP-BY-STEP MECHANISM
🟢 DURING LIFE (Normal Muscle)
Nerve impulse arrives
↓
ATP is present
↓
Actin + Myosin → SEPARATE (muscle RELAXES)
↓
ATP drives calcium BACK into sarcoplasmic reticulum
↓
Muscle stays relaxed until next contraction signal
🔴 AFTER DEATH (Rigor Mortis)
DEATH occurs
↓
No more blood supply → No oxygen → No ATP production
↓
ATP levels fall progressively
↓
Sarcoplasmic reticulum membrane breaks down
↓
Calcium floods into the sarcomere (muscle unit)
↓
Actin + Myosin LOCK TOGETHER permanently
(form rigid ACTOMYOSIN complex)
↓
No ATP available to break them apart
↓
MUSCLE BECOMES STIFF AND HARD
= RIGOR MORTIS
THE KEY NUMBERS
| Event | Level |
|---|---|
| Rigor begins | When ATP falls to 85% of normal |
| Rigor maximum | When ATP is only 15% remaining; Lactic acid = 0.3% |
| Rigor disappears | When putrefaction breaks down actomyosin complex |
EASY ANALOGY
- ATP = the key that keeps the lock open (muscle relaxed)
- After death, the key is lost
- The lock (actin-myosin) snaps shut permanently
- No key = cannot open = Rigor Mortis
WHAT BREAKS RIGOR?
- Putrefaction begins
- Alkaline products from bacteria dissolve the actomyosin complex
- Actin and myosin proteins decompose → muscle softens
SUMMARY IN ONE LINE
Death → No ATP → Calcium floods sarcomere → Actin-Myosin permanently lock → Stiff muscles (Rigor Mortis) → Putrefaction breaks complex → Secondary flaccidity
3 STAGES OF MUSCLE AFTER DEATH
| Stage | What Happens | Duration (India) |
|---|---|---|
| Primary flaccidity | ATP still present, muscles soft | 1-2 hours |
| Rigor Mortis | ATP gone, muscles STIFF | 18-36 hrs (summer) |
| Secondary flaccidity | Putrefaction, muscles soft again | After rigor ends |
QUICK MEMORY TRICK
A - ATP depleted
C - Calcium floods in
T - acTin + myosin lock
I - Irreversible stiffness
N - No relaxation possible
= ACTIN locked = RIGOR MORTIS
Make easy flow chart to score more
RIGOR MORTIS - Score-Booster Flowcharts
📊 FLOWCHART 1: MECHANISM (Draw this in exam)
╔══════════════════════════════════════╗
║ DEATH OCCURS ║
╚══════════════════════════════════════╝
│
▼
╔══════════════════════════════════════╗
║ No blood supply → No O₂ ║
║ → ATP production STOPS ║
╚══════════════════════════════════════╝
│
▼
╔══════════════════════════════════════╗
║ Sarcoplasmic Reticulum breaks down ║
║ → Ca²⁺ FLOODS into sarcomere ║
╚══════════════════════════════════════╝
│
▼
╔══════════════════════════════════════╗
║ Actin + Myosin → LOCK together ║
║ (form rigid ACTOMYOSIN complex) ║
╚══════════════════════════════════════╝
│
▼
╔══════════════════════════════════════╗
║ No ATP to break them apart ║
║ → MUSCLES BECOME STIFF ║
║ = RIGOR MORTIS ║
╚══════════════════════════════════════╝
│
▼
╔══════════════════════════════════════╗
║ Putrefaction begins ║
║ → Actomyosin complex dissolves ║
║ → SECONDARY FLACCIDITY ║
╚══════════════════════════════════════╝
📊 FLOWCHART 2: 3 STAGES OF MUSCLE AFTER DEATH
DEATH
│
├──► STAGE 1: PRIMARY FLACCIDITY (0–2 hrs)
│ • ATP still present
│ • All muscles SOFT & relaxed
│ • Lower jaw drops, joints flexible
│ • Muscular irritability still present
│
├──► STAGE 2: RIGOR MORTIS (2 hrs → 36 hrs)
│ • ATP depleted → Ca²⁺ floods in
│ • Actin-Myosin LOCK
│ • Body becomes STIFF & HARD
│ • Order: Heart → Face → Neck →
│ Chest → Arms → Legs → Fingers
│ • (Nysten's Rule - descending order)
│
└──► STAGE 3: SECONDARY FLACCIDITY (after 36 hrs)
• Putrefaction → alkaline products
• Actomyosin complex BREAKS DOWN
• Muscles SOFT again
📊 FLOWCHART 3: ORDER OF RIGOR (Nysten's Rule)
RIGOR MORTIS APPEARS IN THIS ORDER ↓
❶ HEART (involuntary) ──── 1 hour
│
❷ EYELIDS & FACE
│
❸ NECK & JAW
│
❹ CHEST & UPPER LIMBS
│
❺ ABDOMEN
│
❻ LOWER LIMBS
│
❼ FINGERS & TOES (LAST)
⚠️ DISAPPEARS IN THE SAME ORDER
📊 FLOWCHART 4: FACTORS AFFECTING RIGOR
EARLY ONSET + SHORT DURATION LATE ONSET + LONG DURATION
│ │
───────┴────── ────────┴──────
• Hot weather • Cold weather
• Exhausting diseases • Muscles at rest
(TB, cholera, cancer) • Healthy adults
• Violent death • Death from asphyxia
(firearms, cut-throat) • Hemorrhage
• OP poisoning • CO poisoning
• Strychnine/HCN poisoning (delays disappearance)
• Exercise before death
• Children/old age
📊 FLOWCHART 5: CONDITIONS SIMULATING RIGOR
STIFFNESS OF BODY AFTER DEATH
│
───────┴─────────────────────────────
│ │ │
▼ ▼ ▼
RIGOR MORTIS HEAT STIFFENING COLD STIFFENING
(1-2 hrs) (>65°C) (<-5°C)
│ │ │
Actin-myosin Proteins Body fluids
lock (chemical) coagulate FREEZE
│ (physical) │
CAN be broken CANNOT be Disappears
temporarily broken in warm room
│ │ │
Returns after Normal rigor Normal rigor
breaking does NOT occur occurs RAPIDLY
after after thawing
📊 FLOWCHART 6: CADAVERIC SPASM (Most ML Important!)
INTENSE PHYSICAL/EMOTIONAL ACTIVITY AT TIME OF DEATH
(fear, pain, exhaustion, drowning, strychnine)
│
▼
Muscles actively contracting
at the MOMENT of death
│
▼
PRIMARY FLACCIDITY SKIPPED
│
▼
IMMEDIATE STIFFNESS after death
(Neurogenic mechanism)
│
─────────┴─────────
│ │
▼ ▼
Usually HANDS Occasionally
(most common) WHOLE BODY
│
▼
Passes into NORMAL RIGOR MORTIS → then disappears
MEDICOLEGAL IMPORTANCE:
Weapon in hand → Evidence of SUICIDE
Hair/button in hand → Evidence of STRUGGLE
Weeds in hand (drowning) → Was ALIVE on entering water
📊 FLOWCHART 7: RIGOR MORTIS vs CADAVERIC SPASM
Feature RIGOR MORTIS CADAVERIC SPASM
─────────────────────────────────────────────────────
Onset After primary flaccidity IMMEDIATE at death
Mechanism Chemical (ATP loss) Neurogenic
Muscles ALL muscles ONE group (hands)
Precedes by Primary flaccidity NO flaccidity
Simulated? Cannot after death CANNOT simulate
ML use Time of death Suicide/Homicide proof
⭐ EXAM SCORE TIPS
┌─────────────────────────────────────────────────────┐
│ TO SCORE FULL MARKS IN RIGOR MORTIS QUESTION: │
│ │
│ ✅ Define rigor mortis (1 mark) │
│ ✅ Mechanism flowchart with ATP/Ca²⁺ (3 marks) │
│ ✅ 3 stages of muscle + timeline (2 marks) │
│ ✅ Nysten's Rule - order of appearance (2 marks) │
│ ✅ Factors affecting - table form (2 marks) │
│ ✅ Medicolegal importance (2 marks) │
│ ✅ Cadaveric spasm + ML importance (3 marks) │
│ ✅ Conditions simulating rigor (1 mark) │
└─────────────────────────────────────────────────────┘
Pro tip for exam: Always draw the ATP depletion → Ca²⁺ → Actin-Myosin lock flowchart in your answer. Examiners love it and it shows conceptual clarity. A well-drawn flowchart = guaranteed extra marks!
Make a flow chart for moa
A clean, professional medical flowchart diagram showing the mechanism of action of Rigor Mortis. The flowchart should flow top to bottom with boxes and arrows. Include these steps in order: 1. "DEATH" (top, red box) 2. "No Blood Supply → No Oxygen" 3. "ATP Production STOPS" 4. "ATP levels fall to 85% of normal" 5. "Sarcoplasmic Reticulum membrane BREAKS DOWN" 6. "Ca²⁺ FLOODS into Sarcomere" 7. "Actin + Myosin LOCK together → Rigid ACTOMYOSIN complex forms" 8. "ATP at 15% + Lactic acid at 0.3% → MAXIMUM RIGOR" 9. "RIGOR MORTIS - Body becomes stiff and hard" (highlighted box) 10. "Putrefaction begins → Alkaline products dissolve actomyosin" 11. "SECONDARY FLACCIDITY - Muscles soft again" (bottom, green box) Use colored boxes: red for death, orange for ATP loss, yellow for calcium step, blue for actin-myosin locking, dark red for rigor mortis, green for secondary flaccidity. Include a side note box: "KEY: ATP needed for RELAXATION not contraction. No ATP = No Relaxation = RIGOR". White background, clear readable font, medical textbook style.
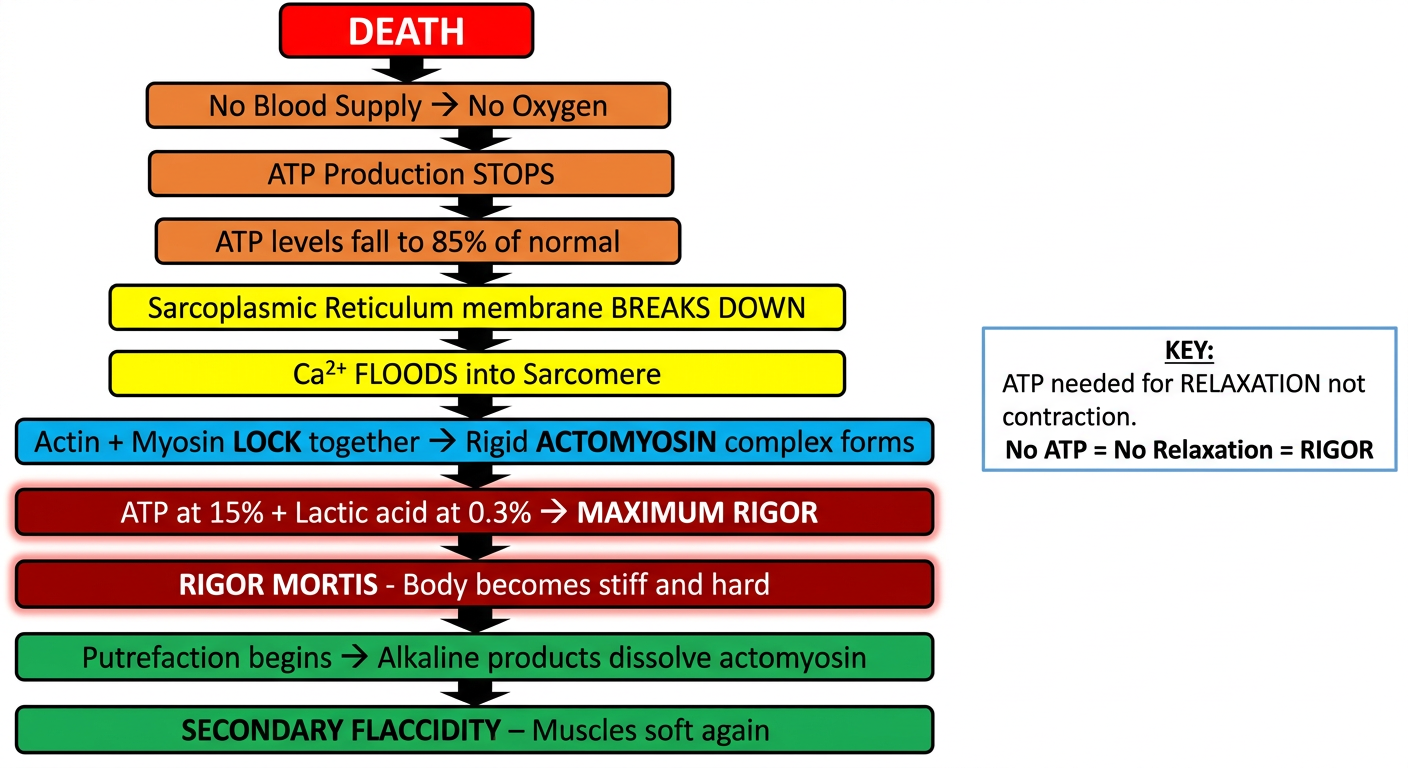
How to use this in your exam answer:
| Color | Step |
|---|---|
| 🔴 Red | Death |
| 🟠 Orange | ATP depletion |
| 🟡 Yellow | Ca²⁺ flooding |
| 🔵 Blue | Actin-Myosin locking |
| 🟤 Dark red | Rigor Mortis (peak) |
| 🟢 Green | Secondary flaccidity |
"ATP is essential for muscle RELAXATION. After death, ATP depletion → Ca²⁺ floods sarcomere → permanent actin-myosin binding → Rigor Mortis. Rigor resolves when putrefaction breaks down the actomyosin complex."
- Rigor begins → ATP at 85%
- Maximum rigor → ATP at 15%, Lactic acid = 0.3%
- Duration in India → 18-36 hrs (summer), 24-48 hrs (winter)
No i need easy exaplaination on moa and to score more
RIGOR MORTIS - MOA Made Super Easy 🎯
🔑 THE ONE THING TO REMEMBER FIRST
ATP = Key for muscle RELAXATION (not contraction) No ATP after death = Muscles CANNOT relax = STAYS STIFF
🧠 UNDERSTAND IT AS A STORY
🟢 DURING LIFE - Normal Muscle
Nerve signal comes
↓
ATP present ✅
↓
Muscle CONTRACTS (actin + myosin join)
↓
Signal stops
↓
ATP pumps Ca²⁺ BACK into sarcoplasmic reticulum
↓
Actin + myosin SEPARATE
↓
Muscle RELAXES 😊
🔴 AFTER DEATH - Rigor Mortis
DEATH
↓
No blood → No O₂ → No food for cells
↓
ATP production COMPLETELY STOPS
↓
ATP levels keep FALLING
↓
Sarcoplasmic reticulum membrane BREAKS
↓
Ca²⁺ POURS OUT freely into sarcomere
↓
Ca²⁺ triggers Actin + Myosin to JOIN
↓
No ATP left to SEPARATE them
↓
They stay LOCKED TOGETHER forever
↓
= RIGID ACTOMYOSIN COMPLEX
↓
= RIGOR MORTIS 💀
📌 KEY NUMBERS (Must Write in Exam)
| When | What happens |
|---|---|
| ATP falls to 85% of normal | Rigor BEGINS |
| ATP falls to 15% of normal | Rigor is MAXIMUM |
| Lactic acid reaches 0.3% | Also at maximum rigor |
🔄 WHAT BREAKS RIGOR? (Secondary Flaccidity)
Putrefaction starts
↓
Bacteria produce ALKALINE products
↓
Alkaline products DISSOLVE actomyosin complex
↓
Actin + myosin SEPARATE again
↓
Muscles become SOFT = Secondary Flaccidity
✍️ HOW TO WRITE MOA IN EXAM (Word for Word)
- Driving Ca²⁺ back into the sarcoplasmic reticulum
- Separating actin and myosin filaments after contraction
🎯 MARKS BREAKDOWN FOR MOA
✅ Define rigor mortis → 1 mark
✅ Role of ATP in life → 1 mark
✅ ATP depletion after death → 1 mark
✅ Ca²⁺ flooding the sarcomere → 1 mark
✅ Actin-myosin locking → 1 mark
✅ Key numbers (85%, 15%, 0.3%) → 1 mark
✅ How rigor resolves → 1 mark
TOTAL = 7 marks 🏆
🧲 EASY MEMORY TRICK
D - Death stops ATP
E - Energy (ATP) depleted
A - Actomyosin forms (actin + myosin lock)
D - Door shut (Ca²⁺ floods in)
C - Ca²⁺ triggers contraction
A - ATP gone = no relaxation
L - Locked muscles = Rigor
M - Maximum at ATP 15%
⚡ ONE-LINE SUMMARY FOR EXAM
"After death, ATP depletion causes Ca²⁺ to flood the sarcomere, permanently locking actin and myosin in a rigid actomyosin complex, producing rigor mortis, which resolves on putrefaction."