Oral uncer treatment
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of oral ulcer (canker sore / aphthous stomatitis) treatment based on authoritative medical textbooks.
Oral Ulcer Treatment
1. Types of Oral Ulcers
| Type | Size | Duration | Features |
|---|---|---|---|
| Minor aphthae | <10 mm | 5–14 days | Most common; self-limiting; flat, shallow |
| Major aphthae | >10 mm | Weeks–months | Deeper, raised borders; may scar |
| Herpetiform aphthae | 1–2 mm (up to 100 lesions) | 10–14 days | Cluster and coalesce; do NOT arise from vesicles |
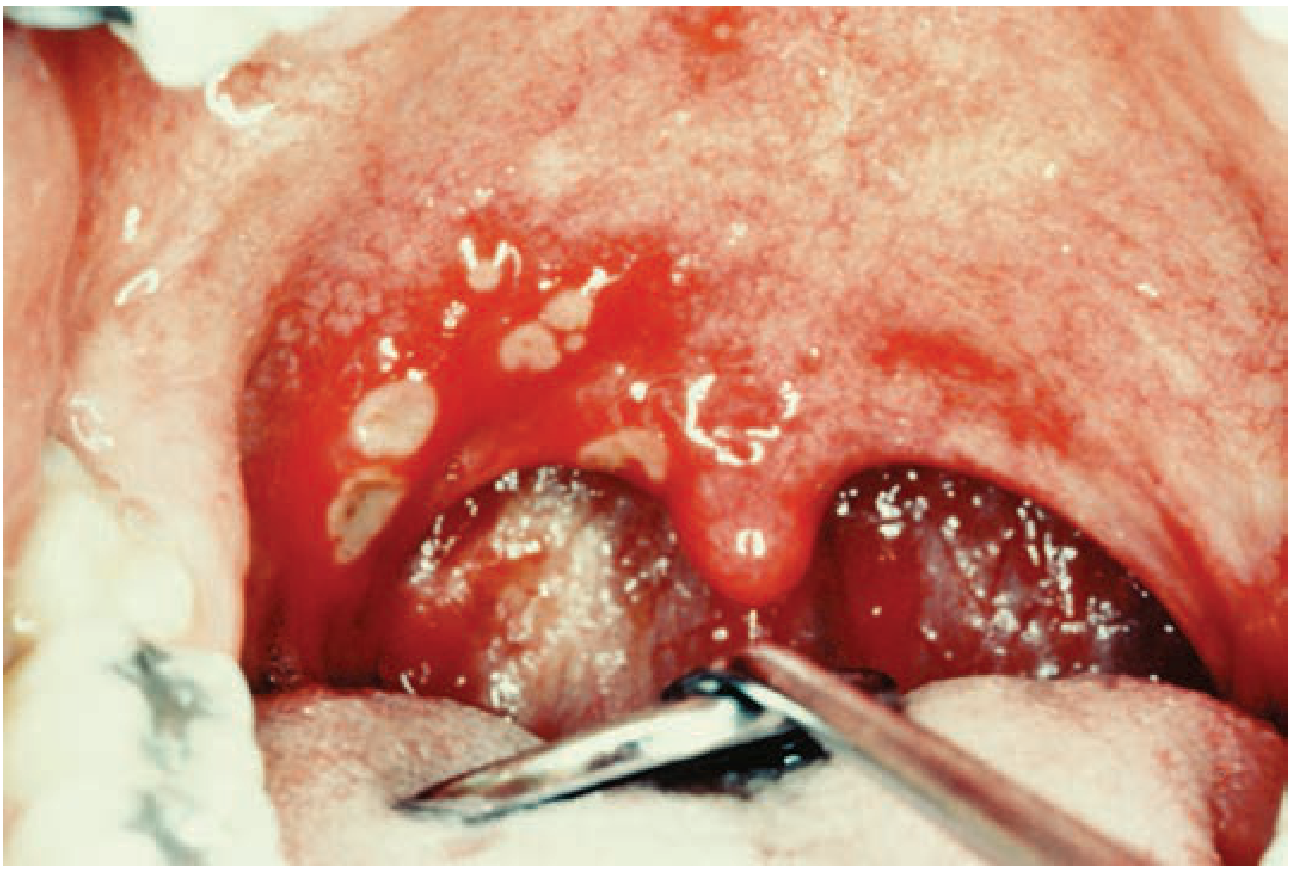
2. Recurrent Aphthous Stomatitis (RAS) — "Canker Sores"
The most common cause of oral ulcers, affecting up to 20% of the population. Etiology is idiopathic/multifactorial (immune, genetic, environmental). Lesions form on non-keratinized mucosa — buccal mucosa, ventral tongue, lips, alveolar mucosa.
Important: No current treatment prevents recurrence. Management goals are pain relief and accelerating healing.
3. Treatment by Severity
Minor / Herpetiform Aphthae
- Often self-limiting — treatment not required unless frequent
- First-line topical agents:
- Topical corticosteroids (e.g., fluocinonide gel/ointment) — reduce severity and duration if applied early (at prodrome or earliest sign)
- Chlorhexidine 0.2% mouthrinse — reduces pain and speeds healing
- Topical anesthetics — symptomatic pain relief
- Bioadhesive pastes (e.g., Orabase containing corticosteroid + anesthetic) — effective; provide a physical barrier
- Tetracycline/doxycycline mouthrinse — a freshly prepared suspension used as a rinse at symptom onset reduces severity and duration
Major Aphthae
- Typically require systemic treatment
- Prednisone (e.g., 40 mg/day for 3 days) — standard approach
- If there is no significant response to steroids → incisional biopsy to exclude malignancy
Refractory / HIV-Associated Ulcers
- Deep, persistent aphthous-like ulcers are more severe in HIV/AIDS
- Treat the underlying condition where possible
- Systemic immunosuppressants may be required in refractory cases
4. Adjunct & Emerging Therapies
- Laser therapy — may promote healing and pain relief in RAS, though clinical trial evidence is not yet definitive — Goldman-Cecil Medicine
5. Cause-Specific Oral Ulcers
When ulcers are secondary to an underlying condition, treat the primary cause:
| Underlying Cause | Management |
|---|---|
| Herpes simplex (HSV) | Topical or oral antivirals (acyclovir); reduces healing time if severe |
| Herpes zoster (VZV) | Oral acyclovir, famciclovir, or valacyclovir |
| Crohn's disease | Corticosteroid solutions; resolve with treatment of CD |
| Behçet syndrome | Systemic immunosuppression (colchicine, corticosteroids, biologics) |
| Celiac disease | Gluten-free diet — aphthae may remit |
| Iron/nutritional deficiency | Correct the deficiency |
| Traumatic ulcers | Remove the source of trauma (sharp tooth edges, ill-fitting dentures) |
| Drug-induced | Discontinue offending drug if possible |
6. Red Flags — Refer / Biopsy
Chronic ulcers lasting >2 weeks, mixed red/white patches (erythroplakia/leukoplakia), or ulcers not responding to steroids require urgent biopsy to exclude:
- Squamous cell carcinoma
- Fungal infection (histoplasmosis, etc.)
- Tuberculosis
- Granulomatosis with polyangiitis
High-risk sites: floor of mouth, ventral/lateral tongue, lower lip, soft palate-tonsillar pillar.
Sources: Goldman-Cecil Medicine, p. 4148–4149; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22E, p. 304–305
This is a shared conversation. Sign in to Orris to start your own chat.