Urinary incontinence
Reading File
Finding Sources
Searching PubMed
"urinary incontinence"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from two authoritative textbooks plus EAU algorithm flowcharts. Let me compile the full answer.
Urinary Incontinence
Definition
Urinary incontinence (UI) is the involuntary leakage of urine sufficient to be a health or social problem. It is not a disease in itself but a symptom of underlying dysfunction in the lower urinary tract, or of conditions outside it. - Goldman-Cecil Medicine, p. 1323
Epidemiology
- More than twice as common in women as in men
- Prevalence increases with age: at least some degree of UI is reported by 11% of women aged 22-27 years
- Afflicts 15-30% of community-dwelling older adults, one third of those in acute care settings, and >50% of nursing home residents
- Estimated cost in the United States exceeded $83 billion in 2020, with out-of-pocket costs >$500 per patient
- Predisposes to: perineal rashes, pressure ulcers, UTIs, falls and fractures
- Associated with: embarrassment, stigmatization, isolation, depression, anxiety, sexual dysfunction, and risk for institutionalization
Pathophysiology
Continence depends on:
- Integrity of lower urinary tract function (bladder + sphincter)
- Adequate mentation, mobility, motivation, and manual dexterity
Age-related changes (predispose but do not cause incontinence):
- Bladder capacity unchanged, but bladder sensation and contractility decrease
- Detrusor smooth muscle develops a "dense band pattern" with depleted caveolae
- Incomplete disjunction pattern (protrusion junctions) underlies involuntary detrusor contractions
- Urethral length and sphincter strength decrease in women
- Prostate enlarges in men (obstruction in ~50%)
- Postvoid residual (PVR) increases in both sexes (normally <100 mL)
- Older persons often excrete most fluid at night, compounding nocturia
Classification and Types
1. Urge Incontinence (Overactive Bladder / Detrusor Overactivity)
- Most common type in older adults (~2/3 of elderly cases)
- Leakage follows abrupt onset of urgency; typically moderate to large volume
- Associated with urinary frequency (>8 voids/day) and nocturia
- Caused by involuntary detrusor contractions; usually idiopathic but can be associated with cerebral disease, upper motor neuron lesions, urethral obstruction, bladder calculus, or bladder carcinoma
- Subtype in elderly: Detrusor hyperactivity with impaired contractility (DHIC) - involuntary contractions but weak bladder; can masquerade as stress incontinence or prostatic obstruction
2. Stress Urinary Incontinence (SUI)
- Second most common in older women; dominant cause in middle-aged women
- Leakage coincides instantaneously with onset and cessation of cough, sneeze, or increased abdominal pressure
- Nocturnal leakage is rare
- Caused by urethral hypermobility (descent of bladder neck/urethra) or intrinsic sphincter deficiency (ISD)
- In men: most often follows radical prostatectomy (post-prostatectomy incontinence, PPI)
3. Mixed Incontinence
- Features of both stress and urge incontinence
- Treatment should target the most bothersome component first
4. Overflow Incontinence
- From urinary retention (impaired detrusor contractility or outlet obstruction)
- Presents as continuous dribbling or frequent small-volume leakage
- Common in men with BPH or neurogenic bladder
5. Functional Incontinence
- Leakage due to impaired mobility, cognition, or motivation in a patient whose lower urinary tract may be intrinsically normal
6. Transient Incontinence (DIAPPERS mnemonic)
Up to 1/3 of community-dwelling elderly have transient causes - these are reversible:
| Cause |
|---|
| Delirium |
| Infection (UTI) |
| Atrophic urethritis/vaginitis |
| Pharmaceuticals (diuretics, anticholinergics, sedatives, alpha-blockers) |
| Psychologic (depression, anxiety) |
| Excessive urine output (hyperglycemia, hypercalcemia, excess fluid intake) |
| Restricted mobility |
| Stool impaction |
Diagnosis
History
- Type, frequency, volume, timing of leakage
- Precipitants (cough, urgency, position change)
- Fluid and caffeine intake
- Medications review
Bladder Diary
- Records voiding times, volumes, incontinence episodes, and activities
- Identifies patterns (e.g., morning diuretic timing, nocturnal polyuria)
Physical Examination
- Abdominal exam (palpable bladder), pelvic/rectal exam
- Neurologic exam
- Provocation test (cough stress test): observe for leakage with cough in full bladder
Investigations
- Urinalysis/MSU - exclude infection, hematuria, glucosuria
- Postvoid residual (PVR) - by ultrasound or catheter; >200 mL suggests overflow or DHIC
- Urodynamics - reserved for diagnostic uncertainty or before surgery; not routine in straightforward presentations
- Cystoscopy/imaging - if hematuria, recurrent UTI, pelvic pain, or prior pelvic radiotherapy
Treatment
Treatment is multifactorial. Transient causes should be addressed first. - Goldman-Cecil Medicine, p. 1330
Step 1: Lifestyle Interventions (All Types)
- Fluid optimization (reduce excess intake; avoid restriction that causes UTI)
- Caffeine reduction
- Weight loss in overweight women (strong evidence for SUI)
- Smoking cessation
- Timed/prompted voiding in elderly or cognitively impaired patients
- Bladder diary self-monitoring
- Pessary (for SUI in women with prolapse)
Step 2: Behavioral Therapy
- Pelvic floor muscle training (PFMT / Kegel exercises) - first-line for SUI and urge UI; evidence-based, effective at all ages. A 2024 systematic review in Sports Health (PMID 37688407) confirms efficacy in women.
- Bladder retraining - progressively increasing voiding intervals + urgency-suppression strategies; effective for urge UI
- As effective as pharmacotherapy for urge UI; combining both is more effective than either alone
Step 3: Pharmacotherapy
For Urge Incontinence / Overactive Bladder:
| Drug Class | Examples | Notes |
|---|---|---|
| Antimuscarinics | Oxybutynin, tolterodine, solifenacin, darifenacin, trospium, fesoterodine | Equally effective; side effects: dry mouth, constipation, visual blurring; cognitive risk (use with caution in elderly) |
| β3-adrenergic agonists | Mirabegron, vibegron | Non-anticholinergic; less cognitive risk; mirabegron can raise blood pressure |
- Immediate-release oxybutynin has the quickest onset - useful for predictable leakage episodes
- Patients on cholinesterase inhibitors (dementia): consider a non-anticholinergic agent
For Stress Incontinence:
- Duloxetine (SNRI; off-label in many regions) - modest efficacy via pudendal nerve stimulation of external urethral sphincter
- Topical estrogen in postmenopausal women - improves urethral/vaginal atrophy
- No currently approved oral drugs are consistently effective for SUI
For Overflow Incontinence:
- Treat the underlying cause (alpha-blockers or 5-alpha-reductase inhibitors for BPH; clean intermittent catheterization for neurogenic retention)
Step 4: Surgical Options (after failed conservative/medical therapy)
Pre-surgical workup: urodynamics + cystoscopy + consider lower urinary tract imaging
Women with SUI:
- Mid-urethral sling (MUS) - tension-free vaginal tape (TVT) or transobturator approach; current gold standard for SUI in women
- Colposuspension (Burch) - open or laparoscopic; durable results
- Bulking agents - urethral injection; less durable, suitable for selected patients
Men with SUI (post-prostatectomy):
- Artificial urinary sphincter (AUS) - gold standard for moderate-severe PPI
- Male sub-urethral sling (fixed or adjustable) - for mild-moderate PPI
For Urge Incontinence refractory to medications:
- OnabotulinumtoxinA (Botox) intravesical injection - 100-200 U; effective for 6-12 months; risk of urinary retention
- Sacral neuromodulation (SNM / InterStim) - implantable device; sustained efficacy
- Percutaneous posterior tibial nerve stimulation (P-PTNS) - less invasive neuromodulation option
- Bladder augmentation / urinary diversion - last resort for refractory cases
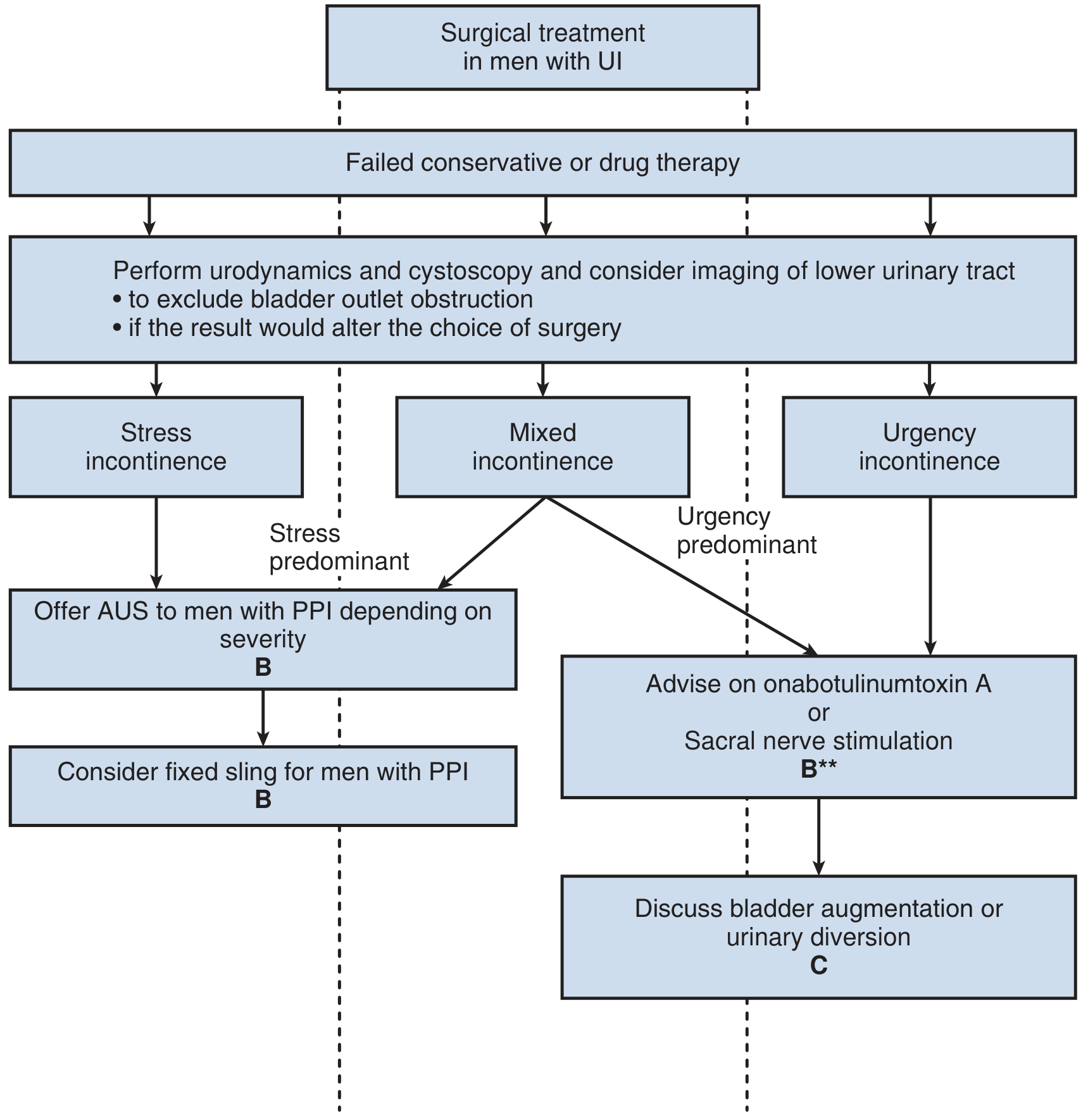
EAU Management Algorithm for Men (Conservative and Surgical)
Conservative pathway:
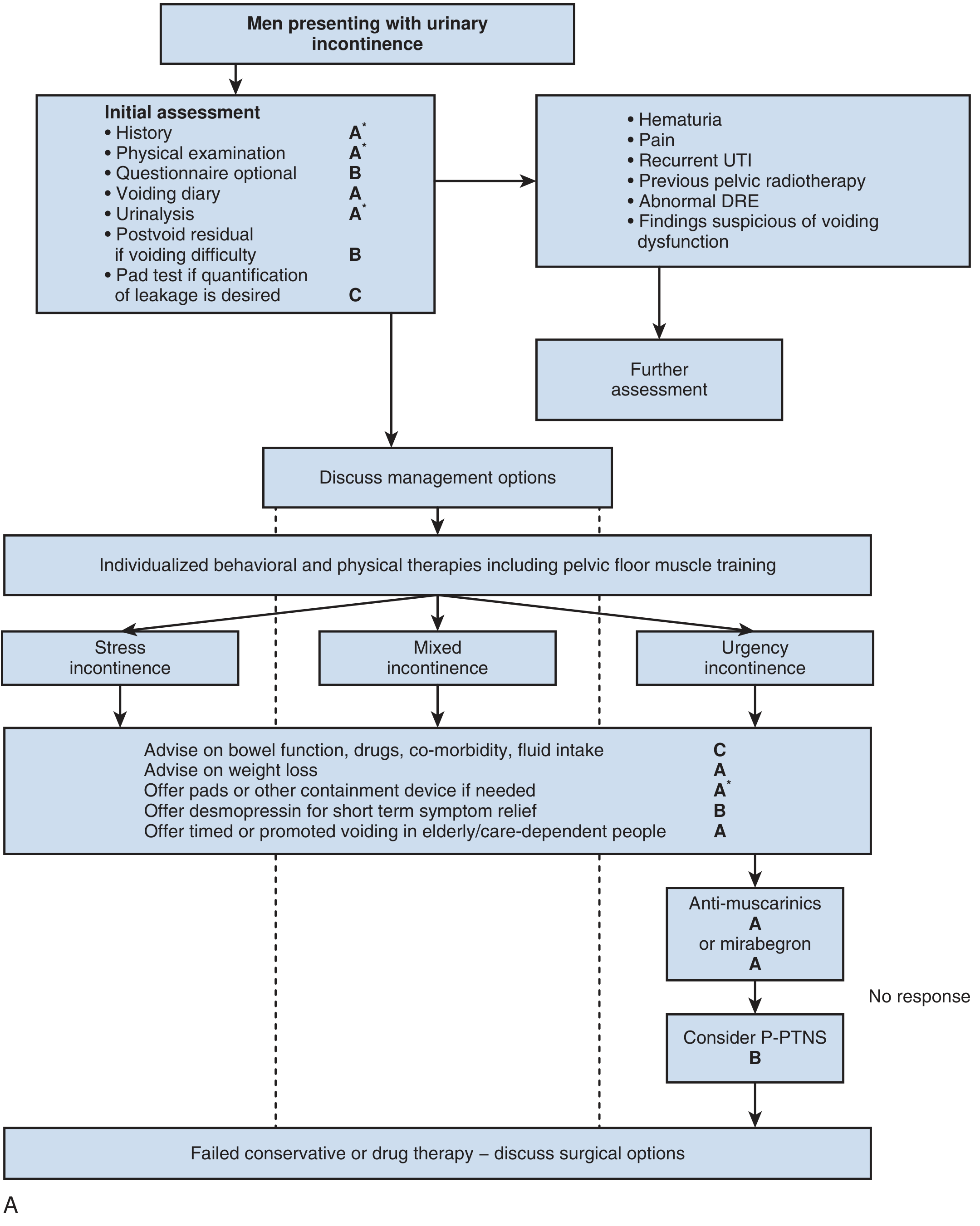
Surgical pathway:
Special Populations
Elderly / Frail Patients
- Incontinence in older patients is more related to comorbid disease and functional impairment than to aging itself
- Treat precipitants first (arthritis, heart failure, medications, delirium)
- Prompted voiding effective for cognitively impaired but partly mobile institutionalized patients
- Use anticholinergics with caution (cognitive effects); prefer beta-3 agonists
- Avoid chronic urinary catheters (high UTI risk)
Men
- Assess for BPH/lower urinary tract obstruction (IPSS, DRE, PVR, uroflowmetry)
- Post-prostatectomy incontinence: pelvic floor exercises initially; AUS or sling if persistent
Women
- Pelvic floor assessment, pelvic organ prolapse evaluation
- Discuss pessary options
- Topical vaginal estrogen post-menopause
- Mid-urethral sling is highly effective surgical option
Key Points
- UI is very common, underreported, and undertreated - always screen in at-risk patients
- Always address reversible/transient causes first (DIAPPERS)
- Behavioral therapy (PFMT + bladder training) is first-line and highly effective
- Urge UI responds to antimuscarinics or mirabegron; behavioral therapy is equally effective
- Stress UI responds best to PFMT and, when refractory, to surgery (mid-urethral sling in women, AUS in men)
- Urodynamics is NOT routinely required before initiating conservative treatment
- Urinary catheters are rarely indicated for chronic UI management
Sources: Goldman-Cecil Medicine International Edition (pp. 1323-1331) | Campbell-Walsh-Wein Urology, 12e | EAU Guidelines on Urinary Incontinence in Adults
This is a shared conversation. Sign in to Orris to start your own chat.