Hydatid cyst Clinical, course, diagnosis, differential diagnosis of methods of surgical treatment. Complications of parasitic diseases of the liver.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching Images
hydatid cyst liver ultrasound CT scan
Reading File
Loading Image
Loading Image
Here is a comprehensive, textbook-based reference on hepatic hydatid cyst disease.
Hydatid Cyst (Hepatic Echinococcosis)
1. Aetiology & Pathology
Hydatid disease is a zoonosis caused by the larval stage of the tapeworm Echinococcus granulosus (most common), with E. multilocularis and E. ligartus accounting for a minority of cases. It is endemic in Mediterranean countries, the Middle East, Far East, South America, Australia, New Zealand, and East Africa. Dogs are the definitive host; sheep are the usual intermediate host; humans are accidental intermediate hosts.
Life cycle: Humans ingest ova shed in dog faeces → oncosphere hatches in the duodenum → penetrates mucosa → enters the portal bloodstream → lodges in the liver (most common, ~75% right lobe) or lungs (20%), kidney, spleen, brain, or elsewhere.
Cyst structure:
- Pericyst (adventitia): outer fibrous host-tissue reaction
- Ectocyst: outer gelatinous (laminated) membrane of the parasite
- Endocyst (germinal layer): inner layer that generates brood capsules containing scoleces ("hydatid sand") and daughter cysts
- Daughter cysts are true replicas of the mother cyst
- Cysts grow ~1–3 cm/year; calcification of the wall does not reliably indicate death of the parasite
About 75% of cysts are solitary and located in the right lobe. Equal sex distribution; mean age ~45 years.
2. Clinical Presentation
The clinical course is largely asymptomatic until complications develop. Symptoms appear once the cyst reaches ~10 cm.
| Feature | Details |
|---|---|
| Symptoms | Right upper quadrant pain, dyspepsia, vomiting |
| Hepatomegaly | Most frequent sign |
| Jaundice | ~8% (biliary communication) |
| Fever | ~8% (secondary infection) |
| Urticaria/pruritus | From minor leakage of cyst fluid |
| Anaphylaxis | From rupture — potentially fatal |
3. Diagnosis
Laboratory
- Routine LFTs — often normal until complications
- Serology (ELISA, indirect haemagglutination, Casoni test): useful but plagued by low sensitivity and specificity; used to confirm imaging findings
Imaging
Ultrasound (first-line — sensitivity 90–95%):
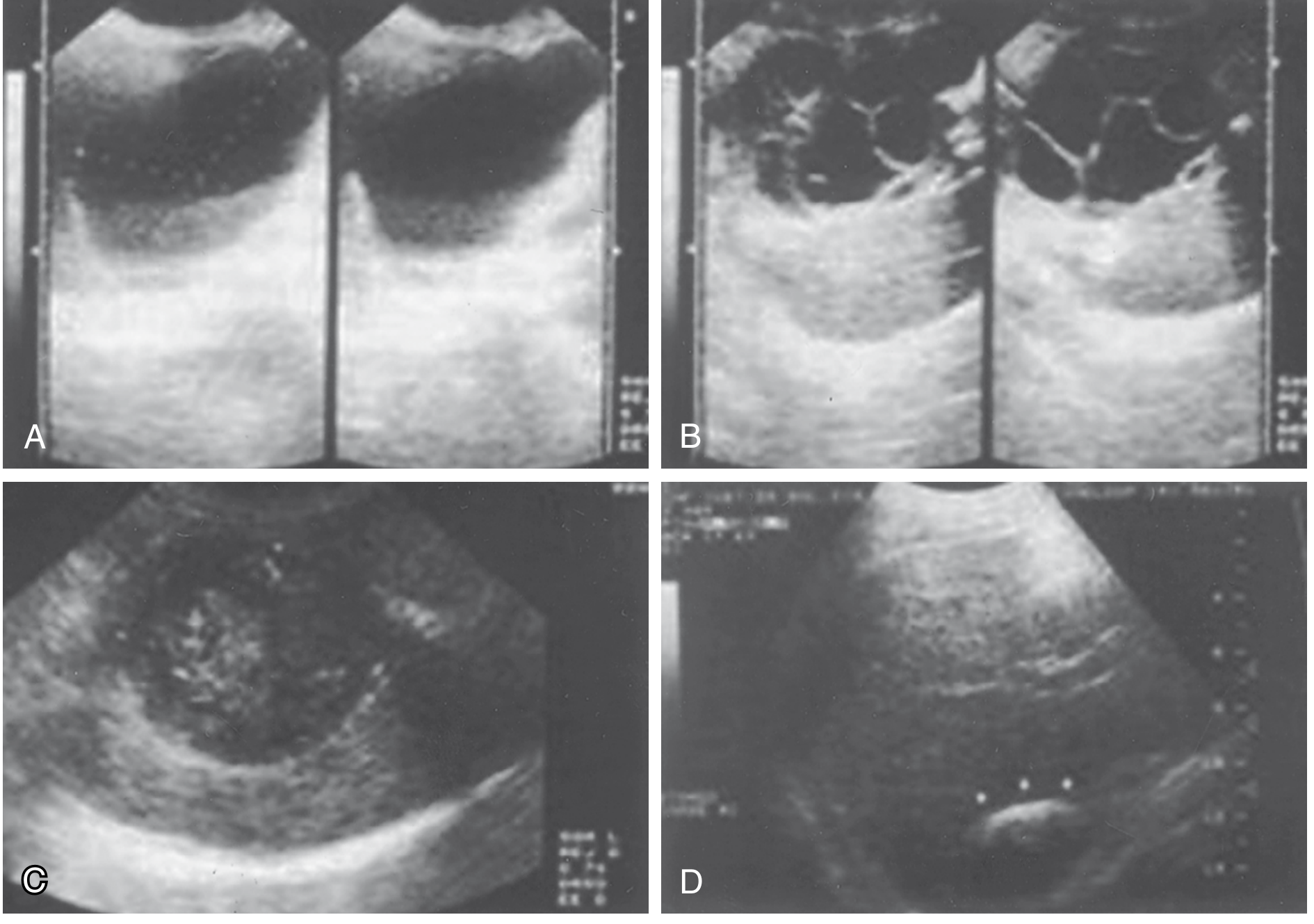
Fig: Ultrasound appearances — (A) Simple cyst with floating hydatid sand. (B) Daughter and granddaughter cysts, rosette sign. (C) Amorphous mass mimicking solid tumour. (D) Calcified "eggshell" wall. — Sabiston Textbook of Surgery
The WHO/Gharbi classification guides treatment choice:
| WHO Type | Gharbi | Description |
|---|---|---|
| CE1 | I | Unilocular cyst, anechoic with hydatid sand |
| CE2 | III | Daughter cysts, rosette pattern |
| CE3 | II | Detached/floating membrane |
| CE4 | IV | Heterogeneous, degenerating |
| CE5 | V | Calcified, inactive |
CT scan (confirmatory): defines extrahepatic disease and anatomical relations to portal/hepatic veins and bile ducts; demonstrates intraperitoneal rupture.

Fig: CT — large, well-circumscribed hypoattenuating hepatic hydatid cyst with significant mass effect.
MRI: best delineates cyst capsule and biliary anatomy.
ERCP/PTC: reserved for suspected biliary communication.
4. Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Simple hepatic cyst | No internal architecture, no calcification, seronegative, non-endemic area |
| Amoebic abscess | Fever, diarrhoea, right shoulder pain, travel history, serology positive for E. histolytica, responds to metronidazole |
| Pyogenic abscess | Fever, leucocytosis, source of infection (biliary/portal), gas on CT, responds to antibiotics + drainage |
| Cystadenoma / cystadenocarcinoma | Septated on imaging, older women, no endemicity, elevated CA19-9/CEA |
| Polycystic liver disease | Multiple bilateral cysts, family history, no serology |
| E. multilocularis (alveolar) | Invasive, infiltrative, irregular calcifications, mimics malignancy, no daughter cysts visible as discrete units |
| Hepatocellular carcinoma | AFP elevated, cirrhotic background, vascular invasion on imaging |
| Metastatic disease | Multiple lesions, known primary tumour |
5. Surgical Treatment — Methods
Surgery remains the primary therapeutic modality. The goal is complete eradication of the parasite with prevention of spillage. Albendazole should be started 4 days preoperatively and continued ≥4 weeks postoperatively to reduce recurrence risk; praziquantel (25 mg/kg/day) combined with albendazole is more effective than albendazole alone.
Preoperatively: epinephrine and steroids must be immediately available for anaphylaxis. The abdomen is thoroughly explored and packed off before cyst manipulation.
A. Conservative (Organ-Preserving) Approaches
1. Open Cyst Evacuation (Marsupialization/Deroofing)
- Cyst is aspirated via closed suction, then flushed with a scolicidal agent (hypertonic saline 20%, 95% ethanol, or cetrimide)
- Caution: never use alcohol if biliary communication is suspected — risk of sclerosing cholangitis
- Cyst is unroofed (deroofed); cavity managed by omentoplasty, external drainage, or left open
- Advantages: lower morbidity (~5% major), technically straightforward
- Disadvantages: ~20% recurrence at 5 years; risk of scolex spillage
2. Minimally Invasive (Laparoscopic) Cyst Evacuation
- Same principle as open evacuation, laparoscopically
- Shorter hospital stay and recovery
- Disadvantages: pneumoperitoneum increases spillage risk; difficulty aspirating thick/large cysts; ~20% recurrence
3. PAIR (Puncture, Aspiration, Injection, Reaspiration)
- Percutaneous ultrasound-guided approach
- Indicated for CE1–CE3 cysts, anterior/peripheral, <5 cm, ≤3 cysts, minimal calcification
- Inject scolicidal agent (95% ethanol or hypertonic saline), then re-aspirate
- Morbidity: 8% minor, 13% major; recurrence ~10%; mortality 0.1%
- Contraindicated in cysts communicating with bile ducts (sclerosing cholangitis risk)
B. Radical Approaches
4. Pericystectomy
- Complete resection of the entire cyst wall including the adventitia (pericyst), either:
- Closed pericystectomy (preferred): without entering the cyst cavity — 0% recurrence at 5–10 years but 19% major morbidity
- Open pericystectomy: after sterilisation and evacuation, pericyst is dissected free
- Best for peripheral cysts; risk of bleeding and biliary injury is higher than simple evacuation
- Vascular and biliary structures controlled with clips/sutures; cavity closed over a drain
5. Liver Resection (Partial Hepatectomy)
- Ranges from wedge resection to formal hemihepatectomy
- Indications:
- Large biliary fistulae not amenable to simpler repair
- Multiple adjacent cysts
- Cysts involving major portal/hepatic veins or bile ducts
- Small peripheral cysts where resection margin is less than pericystectomy area
- Recurrent disease after failed conservative management
- Left lateral segment cysts (segments II/III — safer resection)
- Morbidity ~40–47%, mortality <5%
- Recurrence ~10%
6. Liver Transplantation
- Reserved for massive, unresectable E. multilocularis (alveolar echinococcosis)
- Rarely indicated for E. granulosus
Summary Table of Treatment Options
| Modality | Recurrence | Major Morbidity | Best Indication |
|---|---|---|---|
| Medical therapy alone | 70–80% | Low | Inoperable, disseminated, CE1 <5 cm |
| PAIR | ~10% | 13% | CE1–3, anterior, <5 cm, ≤3 cysts |
| Open cyst evacuation | ~20% | 5% | Endemic settings, uncomplicated |
| Laparoscopic evacuation | ~20% | Low–moderate | Anterior/peripheral, uncomplicated |
| Pericystectomy | ~10% | 19% | Peripheral cysts, specialist centres |
| Liver resection | ~10% | ~40% | Complicated, multiple, central cysts |
All interventions should be accompanied by albendazole ± praziquantel. — Current Surgical Therapy 14e
6. Management of Complicated Disease
Biliary communication (5–15% of cases):
- Diagnosed preoperatively (jaundice/cholangitis) or intraoperatively (bilious aspirate)
- ERCP with sphincterotomy + biliary stenting first, followed by open cyst evacuation
- Intraoperative cholangiogram to confirm bile duct clearance
- Cyst diameter >7.5 cm: 80% likelihood of biliary fistula
- Simple suture closure of fistula is usually sufficient; complex cases may require hepaticojejunostomy
Secondary bacterial infection:
- Treat with systemic antibiotics and adequate cyst drainage
- Presents like pyogenic abscess
Peritoneal/pleural rupture:
- Open surgical exploration mandatory to control dissemination
- Treat anaphylaxis with epinephrine, steroids, antihistamines
- Pleural extension: evacuate both hepatic and pleural cysts; close diaphragm
7. Complications of Parasitic Liver Disease (Hydatid)
| Complication | Notes |
|---|---|
| Biliary rupture (intrabiliary) | Most common; cholangitis, jaundice, biliary colic |
| Secondary bacterial infection | Communicates with biliary tree; presents as abscess |
| Peritoneal rupture | Peritonitis, anaphylactic shock, disseminated echinococcosis |
| Rupture into pleural/pericardial cavity | Transdiaphragmatic extension; hydrothorax, hydropneumothorax |
| Bronchocystic fistula | Cough productive of hydatid membrane ("grape-skin" sputum), hydatid sand |
| Portal hypertension | From venous compression by large cysts |
| Anaphylaxis | From spontaneous or iatrogenic cyst rupture; potentially fatal |
| Disseminated/secondary echinococcosis | Peritoneal seeding from spillage; multiple daughter implants |
| Calcification | Does not reliably indicate cyst death; viable scoleces may persist |
| Recurrence | Post-treatment (ranges 1–27% depending on technique) |
Key References
- Sabiston Textbook of Surgery, Ch. 89 — Hepatic Hydatid Cyst
- Current Surgical Therapy, 14th ed. — Echinococcal Cyst Disease of the Liver
- Mulholland and Greenfield's Surgery, 7th ed. — Treatment of Hepatic Echinococcosis
- Goldman-Cecil Medicine — Echinococcosis and Hydatid Cyst Disease
This is a shared conversation. Sign in to Orris to start your own chat.