Connection of bile salt and blood cholesterol
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive account of the connection between bile salts and blood cholesterol, drawn from authoritative textbooks.
Bile Salts and Blood Cholesterol: The Core Connection
1. Bile Acids Are Made From Cholesterol
The liver converts cholesterol into bile acids — this is the principal route of cholesterol elimination from the body. Cholesterol, a lipophilic molecule, is converted into water-soluble bile acids in pericentral hepatocytes via two major pathways:
- Classical (neutral) pathway — initiated by cholesterol 7α-hydroxylase (CYP7A1), the rate-limiting enzyme; favours cholic acid (CA)
- Alternative (acidic) pathway — initiated by sterol 27-hydroxylase (CYP27A1); favours chenodeoxycholic acid (CDCA)
Under normal physiology, about 0.2–0.6 g/day of bile acids are synthesised, consuming cholesterol as substrate. This can be upregulated to 4–6 g/day after intestinal resection.
"Total body cholesterol metabolism is managed predominantly by the liver; the two principal pathways by which cholesterol is eliminated are cholesterol excretion and bile acid synthesis from cholesterol." — Yamada's Textbook of Gastroenterology
2. The Hepatocyte Is the Central Hub
The diagram below shows how cholesterol flows in the hepatocyte:
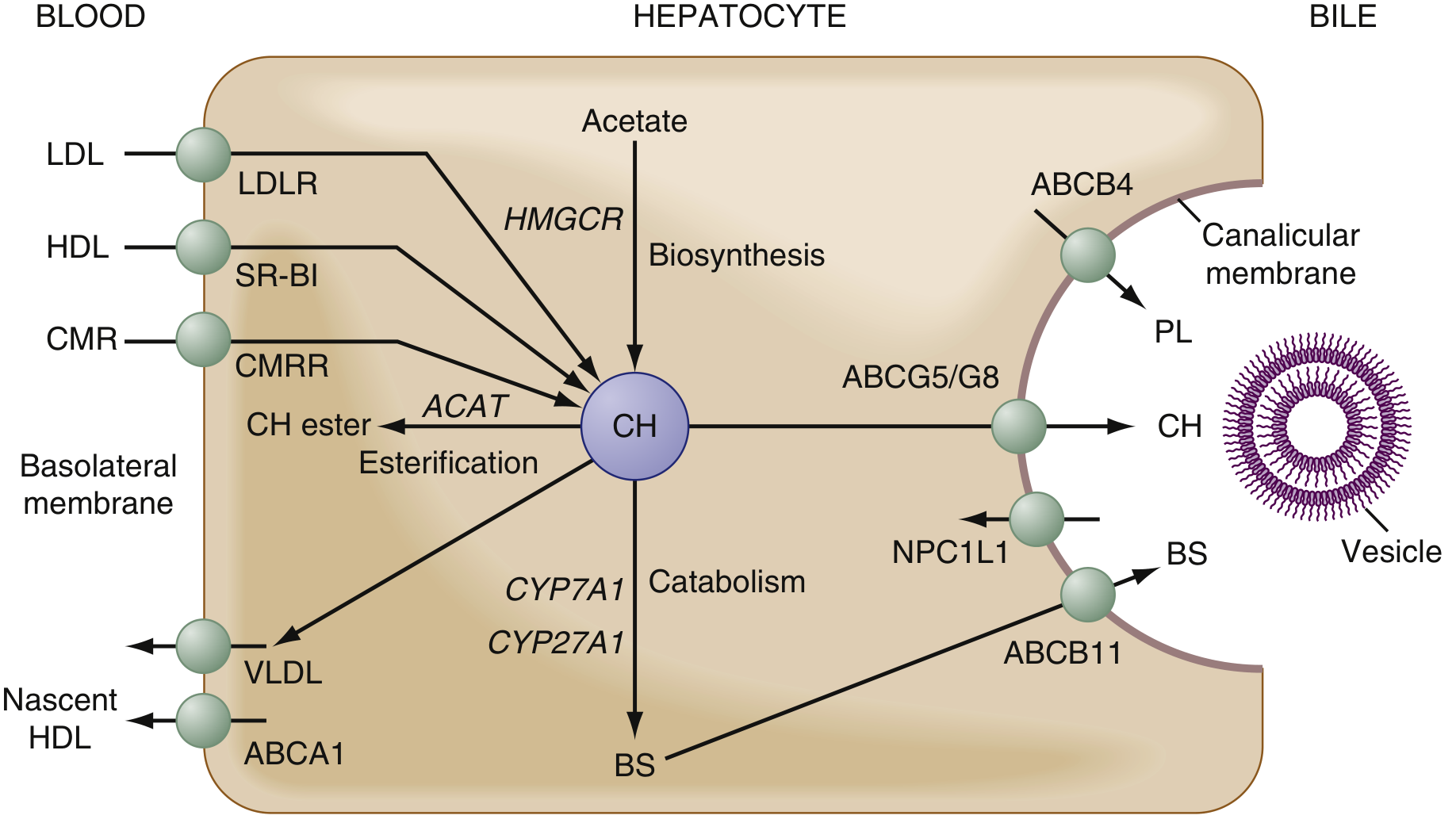
Cholesterol (CH) enters the hepatocyte from blood via LDL receptors (LDLR), HDL via SR-BI, and chylomicron remnants via CMRR. It is then biosynthesised (via HMGCR from acetate), esterified for storage (ACAT), used to form VLDL/HDL, or catabolised into bile salts (BS) by CYP7A1/CYP27A1 — and secreted into bile via ABCB11.
— Sleisenger and Fordtran's Gastrointestinal and Liver Disease
3. The Enterohepatic Circulation: A Feedback Loop That Regulates Blood Cholesterol
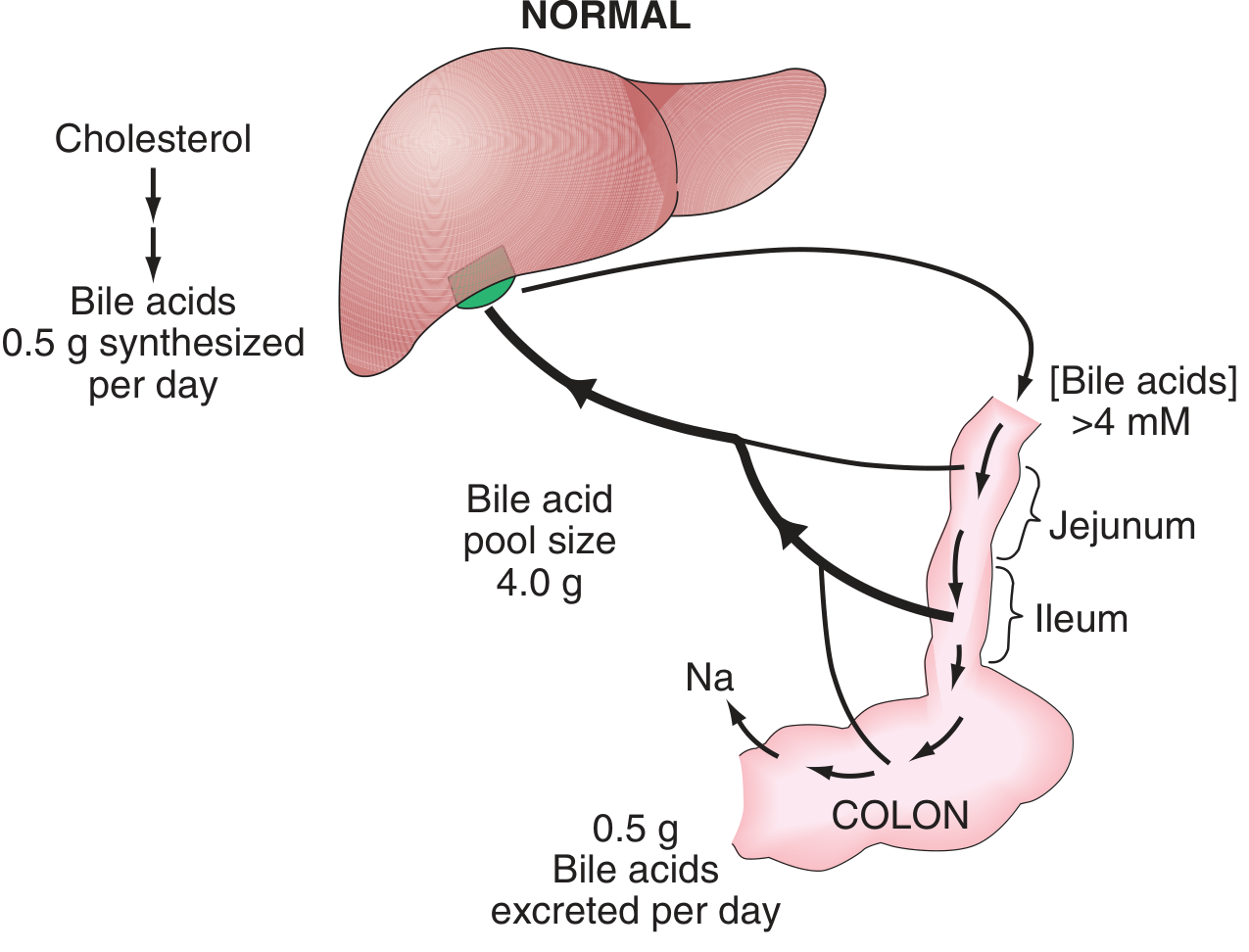
0.5 g bile acids synthesised/day from cholesterol; total pool ~4 g cycling 6–8 times per day. Ileal Na-dependent active transport returns >95% to the liver; ~0.5 g lost in stool daily.
— Harrison's Principles of Internal Medicine 22E
Key features:
- >95% of bile salts are reabsorbed in the terminal ileum via the apical sodium-dependent bile acid transporter (ASBT) and returned to the liver via portal blood.
- The liver extracts them efficiently → newly synthesised bile acids contribute <5% to biliary secretion under normal conditions.
- When the enterohepatic circulation is interrupted (e.g., by disease, ileal resection, or bile acid–binding resins like cholestyramine), fecal bile acid loss rises. This forces the liver to upregulate CYP7A1 and consume more cholesterol to replenish the pool → blood LDL cholesterol falls.
4. How This is Exploited Therapeutically
Bile acid sequestrants (cholestyramine, colesevelam) bind bile salts in the gut, prevent their reabsorption, and increase fecal excretion. The liver responds by:
- Upregulating CYP7A1 → more cholesterol converted to bile acids
- Upregulating LDL receptors (LDLR) → more LDL cleared from blood
Net result: lower serum LDL cholesterol.
5. Feedback Regulation of Bile Acid Synthesis (FXR–FGF19 Axis)
Bile acids themselves suppress their own synthesis. When ileal bile acid concentrations rise:
- Bile acids activate the nuclear receptor FXR (farnesoid X receptor) in enterocytes
- FXR stimulates release of fibroblast growth factor 19 (FGF19)
- FGF19 signals the liver to inhibit CYP7A1 → less bile acid synthesis from cholesterol
"Bile acids in the intestine stimulate the release of fibroblast growth factor 19 (FGF19), which suppresses the hepatic synthesis of bile acids from cholesterol by inhibiting the rate-limiting enzyme cytochrome P450 7A1." — Harrison's Principles of Internal Medicine 22E
6. Biliary Cholesterol Secretion and Gallstones
Beyond being a substrate, cholesterol is also secreted directly into bile (via ABCG5/G8 transporters). Bile salts keep cholesterol soluble in bile by forming mixed micelles with phosphatidylcholine. The ratio of bile acids : phosphatidylcholine : cholesterol in canalicular bile is approximately 10 : 3 : 1.
- When bile salt secretion is low or biliary cholesterol is high, cholesterol supersaturates and crystallises → cholesterol gallstones
- The relationship between bile salt secretion rate and cholesterol secretion is curvilinear: at low bile salt secretion rates, more cholesterol is secreted per bile salt molecule than at higher rates.
Summary Table
| Relationship | Mechanism |
|---|---|
| Bile salts are synthesised from cholesterol | CYP7A1 (classical) and CYP27A1 (alternative) pathways |
| Bile acid loss → lower blood cholesterol | ↑ CYP7A1 activity + ↑ LDL receptor expression |
| Bile acid reabsorption → suppresses synthesis | FXR → FGF19 → inhibits CYP7A1 |
| Bile salt sequestrants lower LDL | Same as bile acid loss mechanism |
| Low bile salt pool → cholesterol gallstones | Loss of micellar solubilisation of biliary cholesterol |
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Harrison's Principles of Internal Medicine 22E; Yamada's Textbook of Gastroenterology; Ganong's Review of Medical Physiology
Name of bile salts
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete classification of bile salts, drawn from the textbooks.
Names of Bile Salts
Bile salts are the ionised (salt) forms of bile acids. They are classified as primary, secondary, and tertiary, and further as conjugated or unconjugated.
Primary Bile Salts
Synthesised directly from cholesterol in the liver:
| Bile Acid | Type | Hydroxyl groups |
|---|---|---|
| Cholic acid (cholate) | Trihydroxy | C-3, C-7, C-12 |
| Chenodeoxycholic acid (chenodeoxycholate) | Dihydroxy | C-3, C-7 |
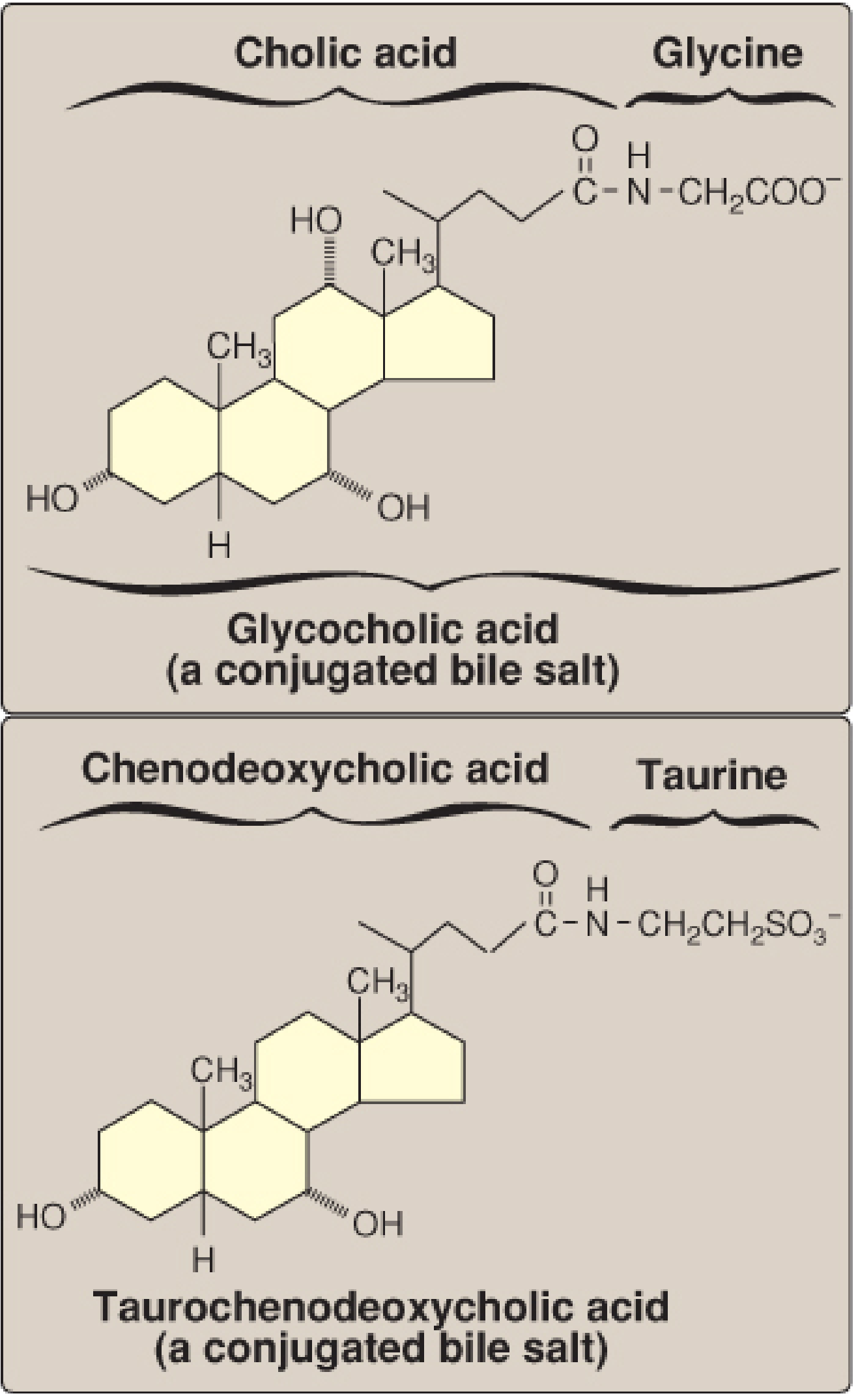
Conjugated Bile Salts
Before secretion into bile, the liver conjugates primary (and some secondary) bile acids with glycine or taurine to form the actual bile salts. This increases water solubility and prevents passive reabsorption in the small intestine.
| Conjugate | Name |
|---|---|
| Cholic acid + glycine | Glycocholic acid (glycocholate) |
| Cholic acid + taurine | Taurocholic acid (taurocholate) |
| Chenodeoxycholic acid + glycine | Glycochenodeoxycholic acid (glycochenodeoxycholate) |
| Chenodeoxycholic acid + taurine | Taurochenodeoxycholic acid (taurochenodeoxycholate) |
Most bile acids are conjugated to glycine (majority) with a smaller proportion conjugated to taurine.
Secondary Bile Salts
Formed by bacterial action (7α-dehydroxylation) on primary bile acids in the ileum and colon:
| Derived from | Secondary Bile Acid |
|---|---|
| Cholic acid | Deoxycholic acid (deoxycholate) |
| Chenodeoxycholic acid | Lithocholic acid (lithocholate) |
| Chenodeoxycholic acid | 7α-oxo-lithocholic acid (intermediate) |
These can also be conjugated by the liver upon reabsorption:
- Glycodeoxycholic acid, Taurodeoxycholic acid
- Glycolithocholic acid, Taurolithocholic acid
Note: Lithocholic acid is only poorly absorbed from the colon.
Tertiary Bile Salts
Formed by further bacterial or hepatic transformation of secondary bile acids:
| Derived from | Tertiary Bile Acid |
|---|---|
| 7α-oxo-lithocholic acid (hepatic reduction) | Chenodeoxycholic acid (reformed) |
| 7α-oxo-lithocholic acid (bacterial 7β-reduction in colon) | Ursodeoxycholic acid (ursodeoxycholate / UDCA) |
Ursodeoxycholic acid (UDCA) is used therapeutically to dissolve cholesterol gallstones and treat primary biliary cholangitis.
Summary Tree
Cholesterol
│
├── Cholic acid (primary)
│ ├── Glycocholic acid ┐ conjugated
│ ├── Taurocholic acid ┘
│ └── → Deoxycholic acid (secondary, by gut bacteria)
│ ├── Glycodeoxycholic acid ┐ conjugated
│ └── Taurodeoxycholic acid ┘
│
└── Chenodeoxycholic acid (primary)
├── Glycochenodeoxycholic acid ┐ conjugated
├── Taurochenodeoxycholic acid ┘
└── → Lithocholic acid (secondary, by gut bacteria)
└── → Ursodeoxycholic acid (tertiary / UDCA)
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; Lippincott's Illustrated Reviews: Biochemistry 8th ed; Harrison's Principles of Internal Medicine 22E
What does insoluble fibre do in body
Finding Sources
Reading File
Reading File
Here is what insoluble fibre does in the body, based on the textbooks.
What Insoluble Fibre Does in the Body
What It Is
Insoluble fibre consists of three main components — cellulose, hemicellulose, and lignin — found in whole grains, bran, nuts, seeds, and mature vegetables. Unlike soluble fibre, it does not dissolve in water and is poorly fermented in the colon.
— Basic Medical Biochemistry: A Clinical Approach 6e; Yamada's Textbook of Gastroenterology
1. Accelerates Gut Transit (Laxative Effect)
- Insoluble fibre causes rapid gastric emptying and decreased intestinal transit time.
- Coarser insoluble fibre mechanically stimulates the colonic mucosa, triggering mucus secretion and increasing stool bulk, making defecation easier.
- This "softens" stool and reduces pressure on the colonic wall.
"Some larger coarse fiber has a mechanical stimulating effect on the colonic mucosa, triggering mucus secretion, resulting in increased stool bulk." — Yamada's Textbook of Gastroenterology
Caution: Small-particle insoluble fibre does NOT have this irritating/stimulating effect and may actually cause a constipating effect by adding dry stool mass.
2. Reduces Risk of Diverticular Disease
By softening stool and reducing intraluminal pressure in the colon, insoluble fibre is thought to prevent the formation of diverticula (pouches in the colonic wall caused by weakness in muscle and submucosal structures).
— Basic Medical Biochemistry: A Clinical Approach 6e
3. Reduces Risk of Colorectal Cancer
Increased stool bulk and faster transit time reduces the time that potential carcinogens remain in contact with the colonic mucosa.
4. Cardiovascular Protection (Reduced CHD/CVD Risk)
Despite not forming gels (unlike soluble fibre), insoluble fibre intake is still inversely associated with risk of coronary heart disease (CHD) and cardiovascular disease (CVD) in multiple meta-analyses. The mechanism is likely multifactorial and not solely dependent on viscosity.
"Soluble and insoluble fibers both appear effective in lowering the risk [of CHD and CVD]." — Yamada's Textbook of Gastroenterology
5. Reduced Risk of Type 2 Diabetes
A meta-analysis pooling 17 prospective cohorts found that higher intake of insoluble fibre (≥25 g/day total fibre) is inversely associated with the risk of developing type 2 diabetes — suggesting mechanisms beyond viscosity (which is a property of soluble fibre) are involved.
— Yamada's Textbook of Gastroenterology
6. Partial Fermentation → Short-Chain Fatty Acids (Minor Role)
While insoluble fibre is poorly fermented compared to soluble fibre, any bacterial fermentation that does occur produces short-chain fatty acids (SCFAs) and gases. SCFAs can be used as energy by colonic epithelial cells, and some travel to the liver via the portal vein.
— Basic Medical Biochemistry: A Clinical Approach 6e
How Insoluble vs. Soluble Fibre Compare
| Property | Insoluble Fibre | Soluble Fibre |
|---|---|---|
| Examples | Cellulose, hemicellulose, lignin | Pectin, gums, mucilages (e.g., psyllium) |
| Water interaction | Does not dissolve | Dissolves / forms gel |
| Gut transit | Speeds up (bulking) | Slows down (gel delays emptying) |
| Colonic fermentation | Poor | Good |
| Lowers LDL cholesterol | Indirect/less direct | Yes (traps bile acids) |
| Lowers blood glucose | Some evidence | Yes (slows carb absorption) |
| Stool bulk | Increases | Increases (via water retention) |
| Diverticular disease | Protective | Protective |
Recommended intake: 22–34 g/day total fibre for adults (no distinction between soluble and insoluble in current guidelines), varying by age and sex.
— Basic Medical Biochemistry: A Clinical Approach 6e (2015 Dietary Guidelines Advisory Committee)
Do we need solvable fibre more or insoluble fibre more in our diet
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
The honest answer from the medical literature is: current dietary guidelines make no distinction between the two — both are needed, and together they are more important than either alone.
Here is what the textbooks say in detail:
Soluble vs. Insoluble Fibre: Which Do You Need More?
Official Guidelines: No Ratio Specified
"The 2015 Dietary Guideline Advisory Committee issued guidelines for fiber ingestion — anywhere from 22 to 34 g/day in adults, depending on age and sex. No distinction was made between soluble and insoluble fibers." — Basic Medical Biochemistry: A Clinical Approach 6e
So the recommendation is simply to eat enough total fibre, ideally from a variety of whole foods that naturally provide both types.
What Each Type Does Better
| Function | Soluble Fibre | Insoluble Fibre |
|---|---|---|
| Lowers LDL cholesterol | ✅ Strong (traps bile acids) | Weak/indirect |
| Lowers blood glucose / glycaemic index | ✅ Yes (slows carb absorption) | Less so |
| Feeds gut bacteria (prebiotic) | ✅ Fermented well | Poorly fermented |
| Produces butyrate (anti-cancer) | ✅ | Less so |
| Speeds bowel transit / stool bulk | Less so | ✅ Strong |
| Prevents diverticular disease | ✅ | ✅ |
| Reduces colorectal cancer risk | ✅ | ✅ |
| Reduces CVD/CHD risk | ✅ | ✅ (both independently protective) |
| Reduces type 2 diabetes risk | ✅ | ✅ (both inversely associated) |
| Constipation relief | ✅ (e.g., psyllium) | ✅ (coarse fibre) |
What the Evidence Shows
- Soluble fibre has more directly proven metabolic benefits — lowering cholesterol, improving blood sugar, and reducing CVD risk through measurable mechanisms (gel formation, bile acid trapping).
- Insoluble fibre is equally protective for colorectal cancer, CVD, and type 2 diabetes through mechanisms that are less well understood but confirmed in large population studies.
- Both types together are more beneficial than either alone. Mixed fibre (e.g., psyllium, which is uniquely soluble yet resistant to fermentation) is often recommended clinically.
"The combination of soluble and insoluble fiber has been proposed to be as effective as soluble fiber alone and perhaps slightly better tolerated." — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Practical Answer
In a typical Western diet, people tend to be low in both, but the greater gap is usually in insoluble fibre (whole grains, bran, vegetables), because processed foods strip it out. In reality:
- ~75% of fibre intake in a balanced diet is insoluble (from grains and vegetables)
- ~25% is soluble (from fruits, oats, legumes)
This natural ratio from whole foods is considered adequate — no separate supplementation of one type over the other is recommended for healthy individuals. However, for specific conditions:
| Condition | Fibre Preferred |
|---|---|
| High LDL cholesterol | Soluble (psyllium, oats, pectin) |
| Constipation | Soluble (psyllium) or coarse insoluble |
| IBS | Soluble (insoluble may worsen bloating/cramping) |
| Diabetes / blood sugar control | Soluble (viscous types) |
| Diverticular disease prevention | Both |
| General gut health / microbiome | Both |
Bottom line: Focus on eating enough total fibre (22–34 g/day) from diverse whole foods. You will naturally get both types. If you have a specific condition (high cholesterol, IBS, constipation), soluble fibre is preferentially recommended by current gastroenterology guidelines.
This is a shared conversation. Sign in to Orris to start your own chat.