Ectropion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from both textbooks. Let me compile the full answer.
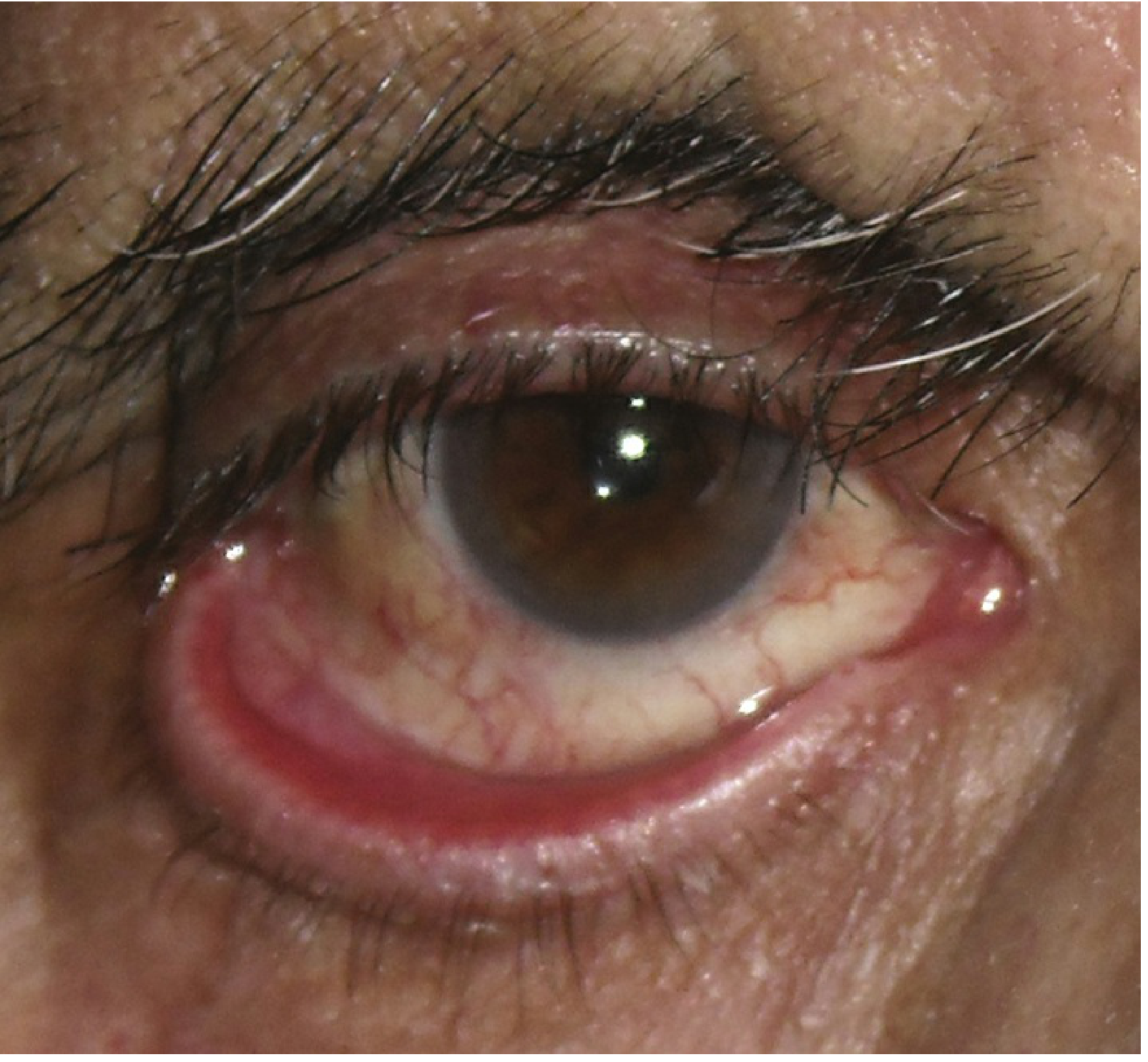
Ectropion
Definition: Ectropion is the outward turning (eversion) of the eyelid margin away from the globe, most commonly affecting the lower lid. The exposed palpebral conjunctiva gives the characteristic red appearance.
Symptoms
- Epiphora (tear overflow / watering)
- Irritation, redness, mucous discharge
- May be asymptomatic in mild cases
Types and Etiology
1. Involutional (Age-related) - Most Common
Affects the lower lid of elderly individuals. Aetiological factors:
- Horizontal lid laxity - pulling the central lid 8 mm or more from the globe, with failure to snap back without blinking
- Lateral canthal tendon laxity - rounded lateral canthus; lower lid displaced >2 mm medially on traction
- Medial canthal tendon laxity - pulling the lid laterally; punctum displaced >1-2 mm (reaches limbus if mild, pupil if severe)
In long-standing cases, the tarsal conjunctiva becomes chronically inflamed, thickened, and keratinized.
2. Cicatricial
Caused by scarring or contracture of the skin and anterior lamella, pulling the eyelid away from the globe. Key test: pushing the skin up over the orbital margin with a finger relieves the ectropion. Opening the mouth accentuates the eversion. Causes include:
- Burns, trauma, prior surgery
- Chronic dermatitis, ichthyosis, actinic damage
- Both lids may be involved; defect may be local or general
3. Paralytic
Caused by ipsilateral CN VII (facial nerve) palsy. Associated with:
- Retraction of both upper and lower lids
- Brow ptosis (which may mimic narrowing of the palpebral aperture)
- Complications: Exposure keratopathy from lagophthalmos, epiphora from punctal malposition, failure of lacrimal pump, reflex hyperlacrimation from corneal exposure
4. Mechanical
Due to herniated orbital fat, eyelid tumor, or other mass effect displacing the lid.
5. Congenital
Associated with facial dysmorphic syndromes (Treacher Collins syndrome), Down syndrome, or as an isolated abnormality.
6. Allergic
Contact dermatitis causing eyelid swelling and eversion.
Signs
- Critical: Outward turning of the eyelid margin
- Superficial punctate keratopathy (SPK) from corneal exposure
- Conjunctival injection, thickening, and eventual keratinization from chronic dryness
- Eyelid scarring (cicatricial cases)
- Facial hemiparesis and lagophthalmos (paralytic cases)
Workup
- History: Prior surgery, trauma, chemical burn, CN VII palsy?
- External examination:
- Orbicularis oculi function
- Horizontal eyelid laxity (snap-back test)
- Punctal position
- Eyelid tumor, scarring, herniated fat
- If CN VII palsy + CN VIII deficit (hearing loss): CT/MRI brain to rule out acoustic neuroma
- Slit lamp examination: Exposure keratopathy, conjunctival inflammation
Treatment
Medical / Temporizing
- Lubricating agents (artificial tears, ointment) for exposure keratopathy
- Warm compresses + antibiotic ointment (bacitracin or erythromycin q.i.d.) for an inflamed, exposed eyelid margin; a short course of antibiotic-steroid ointment (neomycin/polymyxin B/dexamethasone) may help
- Lid taping as a temporizing measure
Surgical - By Type
| Type | Surgical Approach |
|---|---|
| Involutional - generalized | Lateral tarsal strip procedure (shortens and reattaches lower canthal tendon to lateral orbital rim) OR pentagon excision of tarsoconjunctiva |
| Involutional - medial | Medial conjunctival diamond excision (medial spindle procedure); combined with tarsal strip or lateral canthal sling |
| Cicatricial - mild/localized | Excision of scar tissue + Z-plasty to lengthen vertical skin deficiency |
| Cicatricial - severe/generalized | Transposition flaps or free skin grafts (from upper lids, posterior auricular, preauricular, or supraclavicular areas) |
| Paralytic - temporary | High-viscosity lubricants; botulinum toxin into levator to induce temporary ptosis; temporary tarsorrhaphy (especially if poor Bell phenomenon) |
| Paralytic - permanent | Medial canthoplasty (if medial canthal tendon intact); platinum weight implantation in upper lid to correct lagophthalmos; permanent tarsorrhaphy |
Note: In CN VII palsy, surgery is delayed 3-6 months as the ectropion may resolve spontaneously. Corneal exposure may make repair more urgent.
Follow-Up
Patients with corneal/conjunctival exposure are reviewed based on severity. Those using topical steroids need routine monitoring for steroid-induced side effects (raised IOP, cataract).
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 95-101; Wills Eye Manual, 7th ed., pp. 384-386
Entropion
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I have all the information needed. Here is the comprehensive write-up.
Entropion
Definition: Entropion is the inward turning of the eyelid margin, which causes otherwise normal lashes to rub against the globe (pseudotrichiasis). It primarily affects the lower lid and is the opposite of ectropion.
Symptoms
- Irritation and foreign-body sensation (lashes rubbing cornea)
- Tearing
- Redness
- May be asymptomatic in very mild cases
Signs
- Critical: Inward turning of the eyelid margin pushing otherwise normal lashes onto the globe
- Superficial punctate keratopathy (SPK) from lash-cornea contact
- Conjunctival injection
- In severe/long-standing cases: corneal epithelial defect, thinning, ulceration, pannus formation
Types and Etiology
1. Involutional (Age-related) - Most Common
Affects mainly the lower lid of elderly individuals. Four main aetiological factors:
| Factor | Mechanism |
|---|---|
| Horizontal lid laxity | Stretching of canthal tendons and tarsal plate |
| Vertical lid instability | Attenuation, dehiscence, or disinsertion of lower lid retractors (recognized by decreased lower lid excursion in downgaze) |
| Orbicularis override | Pre-tarsal orbicularis is overridden by preseptal orbicularis during lid closure, tipping the tarsal plate inward |
| Orbital septum laxity | Prolapse of orbital fat into the lower lid |
2. Cicatricial
Scarring of the palpebral conjunctiva rotates the upper or lower lid margin towards the globe. Causes:
- Cicatrizing conjunctivitis (mucous membrane pemphigoid, Stevens-Johnson syndrome)
- Trachoma
- Trauma and chemical burns
- Can affect upper or lower lid
3. Spastic
Sustained orbicularis contraction due to surgical trauma, chronic ocular irritation, or blepharospasm. May be acute (post-operative) or subacute.
4. Congenital
Rare; present at birth.
Workup
- History: Previous surgery, trauma, chemical burn, or infection (trachoma, herpes simplex, varicella zoster)?
- Slit lamp examination:
- Corneal involvement (SPK, epithelial defect, ulceration)
- Conjunctival or eyelid scarring (to identify cicatricial type)
- External examination: Assess horizontal laxity, lower lid retractor function (excursion in downgaze), orbicularis function
Treatment
Medical / Temporizing
- Aggressive lubrication + antibiotic ointment (erythromycin or bacitracin q.i.d.) to protect the corneal surface
- Everting the lid and taping with lateral traction - temporizing measure
- Lubricants, soft bandage contact lenses, botulinum toxin into orbicularis - all short-term temporizing options
- Quickert suture (at bedside or in-office) for spastic entropion - tightens lower lid retractors and rotates lid margin anteriorly
Surgical - By Type
Involutional Entropion
| Procedure | Indication / Detail |
|---|---|
| Transverse everting sutures | Quick, easy; typically lasts several months; useful when elaborate surgery is not tolerated (e.g., confused patient) |
| Wies procedure | Durable correction; full-thickness horizontal lid splitting + everting sutures; scar creates barrier between preseptal and pretarsal orbicularis |
| Lower lid retractor reinsertion | Direct exposure and advancement of retractors; more precise than Wies; may be reserved for recurrence |
| Lateral tarsal strip (canthal sling) | Corrects co-existing horizontal lid laxity; retains the lid against the globe, preventing over-correction |
| Pentagon excision | Alternative to tarsal strip for horizontal laxity |
Cicatricial Entropion
| Severity | Procedure |
|---|---|
| Mild | Tarsal fracture (transverse tarsotomy) with anterior rotation of the lid margin |
| Severe | Replace deficient/keratinized conjunctiva + replace scarred, contracted tarsal plate with composite grafts |
| All cases | Horizontal lid laxity corrected with lateral tarsal sling |
Comparison: Entropion vs. Ectropion
| Feature | Entropion | Ectropion |
|---|---|---|
| Direction of lid turning | Inward (toward globe) | Outward (away from globe) |
| Main symptom | Foreign-body sensation, irritation | Epiphora, redness |
| Corneal risk | Direct lash abrasion, ulceration | Exposure keratopathy |
| Most common type | Involutional | Involutional |
| Common surgical repair | Wies procedure, retractor reinsertion | Lateral tarsal strip |
Follow-Up
- If the cornea is uninvolved: no urgent attention required
- If corneal SPK or epithelial defect present: aggressive treatment and close follow-up (see Exposure Keratopathy management)
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 100-102; Wills Eye Manual, 7th ed., pp. 387-388
Presbyopia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have comprehensive information from four authoritative sources. Here is the full write-up.
Presbyopia
Definition: Presbyopia (Greek: "old eye") is the progressive, age-related loss of the eye's ability to accommodate - to focus clearly on near objects - due to increasing rigidity and loss of elasticity of the crystalline lens. It is a universal, physiological phenomenon that affects everyone who lives long enough.
Physiology of Accommodation (Normal)
To understand presbyopia, the normal accommodation mechanism must be understood:
- The lens is a biconvex, elastic structure suspended by zonular fibers (suspensory ligaments) attached to the ciliary body
- At rest, zonules are under tension, keeping the lens relatively flat (suited for distance vision)
- For near vision: parasympathetic stimulation (CN III) causes ciliary muscle contraction (both meridional and circular fibers), which releases zonular tension, allowing the lens to assume a more spherical, convex shape by its own elasticity - increasing refractive power
- In a child, the accommodative range is approximately 14 diopters
Pathophysiology
With age, the lens:
- Grows larger and thicker
- Undergoes progressive denaturation of lens proteins - the lens becomes harder, less elastic, and less pliable
- Loses the ability to change shape even when zonular tension is fully released by ciliary muscle contraction
The result is a progressive decline in accommodative amplitude:
| Age | Accommodative Amplitude |
|---|---|
| Child | ~14 diopters |
| 45-50 years | < 2 diopters |
| 70 years | ~0 diopters (essentially none) |
Once the accommodative amplitude is fully exhausted, each eye remains focused at a fixed distance determined by its individual refractive state.
Epidemiology and Onset
- Typically presents in the 4th to 6th decade of life (symptoms usually noticed around age 40-45)
- Universal - affects all individuals regardless of prior refractive status
- Progressive and irreversible
Symptoms
- Difficulty reading small print (most common presenting complaint)
- Need to hold reading material farther away ("short arm syndrome")
- Eyestrain and headaches after near work
- Blurred near vision, especially in dim light
- Fatigue with sustained reading
Effect by Refractive Status
| Refractive State | Effect of Presbyopia |
|---|---|
| Emmetrope | Requires reading glasses for near work |
| Myope (nearsighted) | May achieve near vision simply by removing distance glasses - the uncorrected myopic eye is naturally focused near; presbyopia may be less symptomatic |
| Hyperope (farsighted) | Symptoms appear earlier and more severely - already using accommodative reserve for distance; loses near vision sooner |
| Post-refractive surgery | Managed the same as emmetropes |
Correction / Treatment
1. Spectacles (Glasses) - First-line
- Reading glasses - single-vision near correction for emmetropes
- Bifocals - distance correction above + near addition below; most common for existing glasses wearers
- Trifocals / Progressive addition lenses (PALs) - graduated correction for distance, intermediate, and near; no visible line
2. Contact Lenses
- Monovision contact lenses - dominant eye corrected for distance, non-dominant for near; relies on neuroadaptation and suppression of blur
- Multifocal contact lenses - simultaneous vision with distance and near zones
3. Surgical Options
| Procedure | Description |
|---|---|
| Monovision LASIK/PRK | Laser refractive surgery targeting one eye for distance, fellow eye for near/intermediate |
| Conductive keratoplasty (CK) | Radiofrequency energy applied to corneal stroma; can impart multifocal functionality |
| PresbyLASIK (corneal multifocality) | Laser alters corneal asphericity to create bifocal/transitional effect; controlled change from centre to periphery; benefit over monofocal ablation not yet clearly established |
| Intracorneal inlays | Implanted in stromal pocket or under LASIK flap; three types: (a) refractive inlays, (b) corneal reshaping inlays, (c) small aperture inlays (pinhole effect); biocompatibility concerns historically limited use |
| Clear/Refractive lens exchange (CLE/RLE) | Removal of the natural lens + IOL implantation; also called PreLEx; eliminates risk of future cataract |
| Multifocal / EDOF IOL | Bifocal diffractive, trifocal, multifocal refractive, or extended depth of focus IOL; restores reading vision but may cause nocturnal glare, halos, reduced contrast sensitivity; contraindicated for pilot licences and military service in some jurisdictions |
| Accommodating IOL | Pseudo-accommodating; attempts to restore dynamic focus; still under development |
| Monovision IOL | One eye targeted for distance, other for near; requires neuroadaptation |
| Scleral expansion surgery | Results inconsistent and unpredictable; not widely adopted |
Note on intracorneal inlay complications: decentration, dry eyes, keratolysis, corneal vascularization, and corneal haze requiring removal.
Key Clinical Points
- The myopic patient is the exception - removing distance glasses may suffice for near vision despite presbyopia
- Pinhole testing improves acuity in refractive errors but does not restore accommodation lost in presbyopia
- Presbyopia is distinct from pathological causes of near vision loss (e.g., cataract, macular disease)
- New-onset presbyopia symptoms in a younger patient should prompt consideration of drug effects (e.g., anticholinergics) or systemic disease
Sources: Guyton & Hall Textbook of Medical Physiology, p. 624; Goldman-Cecil Medicine, 26th ed.; Harrison's Principles of Internal Medicine, 22nd ed., p. 264; Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.
Keratoplasty
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the key content. Let me compile the comprehensive answer.
Keratoplasty (Corneal Transplantation / Corneal Grafting)
Definition: Keratoplasty is the surgical replacement of diseased host corneal tissue with healthy donor cornea. Grafts may be partial-thickness (lamellar - anterior or posterior) or full-thickness (penetrating), depending on which corneal layers are diseased.
General Indications
| Category | Purpose | Examples |
|---|---|---|
| Optical | Improve vision | Keratoconus, corneal scarring, corneal dystrophies, pseudophakic bullous keratopathy, corneal degenerations |
| Tectonic | Restore/preserve structural integrity | Severe thinning, descemetocoele, perforated corneal ulcer |
| Therapeutic | Remove infected tissue unresponsive to antimicrobials | Refractory microbial keratitis |
| Cosmetic | Improve appearance | Rare indication |
Donor Tissue
- Removed within 12-24 hours of death
- Age-matching of donor and recipient is attempted
- Corneas from infants ≤3 years are rarely used even in paediatric transplants - associated with surgical, refractive, and rejection problems
- Stored at eye banks where pre-release evaluation includes:
- Medical history and blood screening (to exclude contraindications)
- Microscopic examination + endothelial cell count
- Storage methods:
- Hypothermic storage: up to 7-10 days
- Organ culture medium: up to 4 weeks (allows more time for evaluation)
Types of Keratoplasty
1. Penetrating Keratoplasty (PK) - Full Thickness
Full-thickness replacement of all corneal layers. Indicated when disease involves all layers of the cornea.
Key surgical points:
- Common graft size: 7.5 mm
- Small grafts → high astigmatism
- Large grafts (>8 mm) → increased risk of peripheral anterior synechiae + raised IOP
- Donor button is ~0.25 mm larger than the host trephination site
- Preparation of donor cornea always precedes host excision (in case donor tissue is unsuitable)
- Trephination: mechanically guided manual or automated (including laser)
- Sutures: continuous, interrupted, or combination (Fig. 8.4)
Postoperative management:
- Topical steroids (prednisolone acetate 1% or dexamethasone 0.1%): initially every 2 hours, gradually tapered; long-term low-dose (once daily for a year or more) is usual
- Other immunosuppressants (oral azathioprine, topical/systemic ciclosporin): reserved for high-risk cases
- Cycloplegia (homatropine 2% b.d.): for 1-2 weeks
- Oral acyclovir: if pre-existing HSV keratitis, to minimize recurrence
- IOP monitoring: non-applanation method preferred (applanation unreliable over graft)
- Endothelial monitoring: central corneal thickness by pachymeter (indirect measure)
- Suture removal: typically at 12-18 months (longer in elderly); broken or loose sutures removed immediately to reduce vascularization and rejection risk
2. Superficial Lamellar Keratoplasty (SLK)
Partial-thickness excision of corneal epithelium and stroma, leaving the endothelium and deep stroma intact as the recipient bed.
Indications:
- Opacification of superficial one-third of corneal stroma (not from recurrent disease)
- Marginal corneal thinning/infiltration (e.g., recurrent pterygium, Terrien marginal degeneration, limbal dermoid/tumour)
- Localized thinning or descemetocoele formation
3. Deep Anterior Lamellar Keratoplasty (DALK)
Corneal tissue is removed almost to the level of Descemet membrane (DM), preserving host endothelium. Removes approximately anterior 95% of corneal thickness.
Indications:
- Anterior corneal disease with normal endothelium and no breaks/scars in Descemet membrane (e.g., keratoconus without history of acute hydrops, superficial trauma)
- Chronic inflammatory disease with high rejection risk (e.g., atopic keratoconjunctivitis)
Advantages over PK:
- No risk of endothelial rejection (epithelial/subepithelial/stromal rejection can still occur)
- Less postoperative astigmatism
- Structurally stronger globe
- Increased availability of donor material (endothelial quality irrelevant)
Disadvantages:
- Technically difficult and time-consuming; high perforation risk
- Interface haze may limit final visual acuity
- Postoperative management similar to PK but lower-intensity steroids; sutures removable after ~6 months
4. Endothelial Keratoplasty (EK)
Selective replacement of the diseased endothelium ± Descemet membrane through a small corneal/corneoscleral incision (2.8-5.0 mm). Folded donor tissue is introduced through this small incision.
Two Main Techniques:
| Feature | DSAEK | DMEK |
|---|---|---|
| Full name | Descemet Stripping (Automated) Endothelial Keratoplasty | Descemet Membrane Endothelial Keratoplasty |
| What is transplanted | DM + endothelium + thin posterior stroma | DM + endothelium only |
| Graft thickness | Thicker (includes stroma) | Very thin (5-10 μm) - difficult to handle |
| Visual outcome | Good | Better (fewer interface irregularities, faster recovery) |
| Rejection rate | Lower than PK | Even lower than DSAEK |
| Intraoperative complications | Lower | Higher |
| Most commonly performed | ✓ (currently) | Less common but preferred for best outcomes |
Indications: Endothelial disease - Fuchs endothelial corneal dystrophy, pseudophakic bullous keratopathy, localized tectonic patching for corneal perforation.
Advantages over PK:
- Minimal refractive change; structurally more intact globe
- Faster visual rehabilitation
- Minimal suturing required
Disadvantages:
- Significant learning curve; specialized equipment required
- Visual outcome often suboptimal due to: graft thickness differences, irregularities, high-order aberrations, donor-recipient interface fibrosis
- Endothelial rejection can still occur
Key Tip: DSAEK results in more rapid visual improvement and less risk of rejection than penetrating keratoplasty.
5. Limbal Stem Cell Grafting
Used when the limbal stem cell population is depleted (limbal stem cell deficiency - LSCD), causing failure of corneal epithelial self-renewal.
Techniques:
- Transplantation of a limited limbal area from the healthy fellow eye
- Complete limbal transplantation of a donor annulus
- Ex vivo expansion/culture of host or donor stem cells + transplantation
Important: In unilateral Stevens-Johnson syndrome or ocular cicatricial pemphigoid, donor tissue must not be taken from the unaffected fellow eye (use allograft, not autograft).
Postoperative Complications
Early Complications (PK)
- Persistent epithelial defects
- Loose or protruding sutures (risk of infection, papillary hypertrophy)
- Wound leak (flat anterior chamber, iris prolapse)
- Uveitis, raised IOP
- Traumatic graft rupture
- Cystoid macular oedema
- Microbial keratitis, endophthalmitis
- Urrets-Zavalía syndrome (fixed dilated pupil) - rare
- Graft rejection
Late Complications
- Astigmatism
- Recurrence of underlying disease
- Late wound dehiscence
- Retrocorneal membrane formation
- Glaucoma
- Graft rejection / failure without rejection
Corneal Graft Rejection
Immunological Privilege of the Cornea
The cornea is immunologically privileged due to:
- Absence of blood vessels and lymphatics
- Few antigen-presenting cells
Inflammation and neovascularization break this privilege and dramatically increase rejection risk.
Predisposing Factors
- Host stromal vascularization (most significant)
- Eccentric or large grafts (>8 mm diameter)
- Infection (especially herpetic)
- Glaucoma
- Previous keratoplasty
- HLA mismatch (HLA matching has small but beneficial effect on graft survival)
- Gender incompatibility: male donor cornea should NOT be given to a female recipient (recently identified as an important risk factor)
Symptoms
Blurred vision, redness, photophobia, pain - but many cases are asymptomatic until rejection is established. Onset: days to years after surgery.
Signs by Rejection Layer
| Type | Timing | Signs |
|---|---|---|
| Epithelial | ~3 months (average) | Elevated line of abnormal epithelium in a quiet/mildly inflamed eye |
| Subepithelial | Variable | Subepithelial infiltrates (Krachmer spots) - resemble adenoviral keratitis; deeper oedema and infiltrative opacification |
| Stromal | Variable | Deeper haze; can be chronic or hyperacute (latter with endothelial rejection) |
| Endothelial | Variable (most serious) | Khodadoust line - linear pattern of keratic precipitates at graft margin with adjacent inflammation; stromal oedema = endothelial failure |
Management of Rejection
Urgency: Endothelial > Stromal > Subepithelial > Epithelial
- Preservative-free topical steroids hourly for 24 hours → gradual taper over weeks; steroid ointment at bedtime
- Topical cycloplegia (homatropine 2% or atropine 1% once/twice daily)
- Topical ciclosporin 0.05-2% (delayed onset)
- Systemic steroids: oral prednisolone 1 mg/kg/day for 1-2 weeks OR IV methylprednisolone 500 mg/day for up to 3 days (if within 8 days of onset - particularly effective)
- IOP monitoring throughout
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 276-298
Blepharitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have all the essential content. Now I'll compile the comprehensive answer.
Blepharitis
Definition: Blepharitis is a common, bilateral, usually symmetrical chronic inflammation of the eyelid margin. It is one of the most frequent causes of ocular discomfort and irritation in clinical practice. Poor correlation between symptoms and signs makes management difficult, and a permanent cure is unlikely - the goal is symptom control.

Classification
Blepharitis is divided into anterior and posterior forms, though significant overlap exists and mixed blepharitis is the most common presentation.
Types, Aetiology and Pathophysiology
1. Anterior Blepharitis
Affects the area around the bases of eyelashes.
a) Staphylococcal Blepharitis
- Causative agent: Staphylococcus aureus
- Mechanism: Abnormal cell-mediated immune response to components of S. aureus cell wall
- More common and severe in patients with atopic dermatitis
- Responsible for peripheral corneal infiltrates and red eyes in some patients
- More amenable to treatment and remission than posterior disease
b) Seborrhoeic Blepharitis
- Strongly associated with seborrhoeic dermatitis (scalp, nasolabial folds, skin behind ears, sternum)
- Characterized by greasy, waxy scales (scurf) clinging to lashes
- Less inflammatory than staphylococcal
2. Posterior Blepharitis (Meibomian Gland Dysfunction - MGD)
- Caused by dysfunction and altered secretions of meibomian glands
- Bacterial lipases → formation of free fatty acids → raises melting point of meibum → inspissation of glands → obstructed orifices
- Loss of tear film phospholipids (surfactants) → increased tear evaporation and osmolarity → unstable tear film
- Promotes growth of S. aureus
- More persistent and chronic than anterior blepharitis
- Strongly associated with acne rosacea
3. Demodex Blepharitis
- Caused by the hair follicle/sebaceous gland mite Demodex:
- D. folliculorum longus → anterior blepharitis
- D. folliculorum brevis → posterior blepharitis
- Collarettes (partially digested epithelial cells, keratin, waste, and mite eggs around lash bases) are considered pathognomonic
- Found normally in most older adults; symptomatic disease may relate to overpopulation or hypersensitivity to a commensal Bacillus carried by the mite
- Detection: under ×16 slit lamp magnification, rotating an epilated lash reveals mites (0.2-0.4 mm); slide microscopy for confirmation
4. Angular Blepharitis
- Inflammation localized to the medial and/or lateral canthal angles
- Associated with Moraxella spp.
Symptoms
- Burning, grittiness, mild photophobia, crusting on waking
- Stinging - more common in posterior disease
- Itching, tearing, foreign body sensation
- Eyelid erythema
- Usually no visual disturbance
- Symptoms often worse in the morning (distinguishes from dry eye, where symptoms worsen later in the day)
- Bilateral and symmetrical involvement
Signs
Critical:
- Crusty, red, thickened eyelid margins with prominent blood vessels
- Inspissated (blocked) meibomian gland orifices
- Crusting and collarettes around lash bases (Demodex)
- Cylindrical sleeves on lashes (Demodex)
Staphylococcal-specific signs:
- Hard, fibrinous crusts adherent to lash bases (leave a bleeding ulcer when removed)
- Madarosis (lash loss), trichiasis, poliosis (whitening of lashes)
Seborrhoeic-specific signs:
- Soft, greasy, easily removed scales (scurf)
- Oily lid margins; no ulceration
Posterior/MGD-specific signs:
- Capping of meibomian orifices by oil globules
- Plugged, inspissated meibomian gland orifices
- Expressed toothpaste-like or frothy material at lid margin
- Froth on lid margin
Other signs (all types):
- Conjunctival injection, mild mucous discharge, SPK
- Papillary conjunctivitis
- Inferior corneal punctate epithelial erosions
- Marginal keratitis, phlyctenules, corneal vascularization/scarring
- Rosacea (face/nose)
Characteristics Comparison Table
| Feature | Staphylococcal | Seborrhoeic | Posterior (MGD) |
|---|---|---|---|
| Scales | Hard, fibrinous, adherent | Soft, greasy, scurf | Meibomian plugging |
| Lash changes | Madarosis, trichiasis, poliosis | Minimal | Minimal |
| Corneal changes | Marginal infiltrates, inferior SPK | Minimal | Inferior SPK |
| Associated condition | Atopic dermatitis | Seborrhoeic dermatitis | Acne rosacea |
| Organism | S. aureus | Not primarily infective | Altered meibum + bacteria |
Secondary / Chronic Complications
- Papillary conjunctivitis
- Inferior corneal punctate erosions
- Corneal scarring and vascularization
- Salzmann nodular degeneration
- Stye (hordeolum) formation
- Marginal keratitis
- Bacterial keratitis (especially in contact lens wearers)
- Phlyctenular eye disease
- Blepharoconjunctivitis (if becomes chronic)
Differential Diagnosis
- Pediculosis (eyelash lice)
- Demodicosis (cylindrical sleeves + microscopy)
- Sebaceous carcinoma - must be considered in intractable, unilateral, or asymmetric blepharitis (upper vs. lower lid asymmetry); warrants formal clinical workup
Treatment
Patients should be counselled that blepharitis is a chronic condition - permanent cure is unlikely but symptom control is achievable with consistent lid hygiene.
Step 1 - Lid Hygiene (All Types - First-line)
- Warm compresses for 5-10 minutes b.i.d. to q.i.d. (softens crusts and meibum)
- Lid margin scrubbing with wet cotton bud, clean wet face-cloth, or commercial soap/alcohol-impregnated eyelid scrub pads
Note: Baby shampoo is NOT recommended - it destabilizes the tear film and is a common cause of contact dermatitis
- For significant MGD: express accumulated meibum by rolling a finger anteriorly over the lid margin
- Frequency: twice daily initially, reduce as symptoms improve; may need to be maintained indefinitely
Step 2 - Topical Antibiotics (Anterior Disease)
- Sodium fusidic acid, erythromycin, bacitracin, azithromycin, or chloramphenicol ointment
- Applied to anterior lid margin with cotton bud after lid hygiene, at bedtime (q.h.s.)
Step 3 - Dry Eye Management
- Preservative-free artificial tears 4-8 times per day if associated dry eyes
Step 4 - Oral Antibiotics (Moderate-Severe / Posterior Disease)
Tetracyclines reduce bacterial colonization and staphylococcal lipase production:
| Drug | Regimen |
|---|---|
| Doxycycline | 50-100 mg b.d. for 1 week → 50-100 mg daily for 6-24 weeks |
| Lymecycline | 408 mg once daily for up to 3 months |
| Azithromycin | 500 mg daily × 3 days, repeated for 3 cycles at 1-week intervals |
| Minocycline | 50-100 mg once daily |
| Tetracycline | 250 mg twice daily |
⚠️ Tetracyclines are contraindicated in pregnant women, nursing mothers, and children ≤8 years old. Use erythromycin 200 mg p.o. b.i.d. as an alternative.
Step 5 - Anti-inflammatory Agents
- Cyclosporine 0.05% or 0.09% eye drops b.i.d.
- Lifitegrast 5% drops b.i.d.
- Omega-3 fatty acid supplementation (oral)
- Topical antibiotic-steroid combinations (e.g., tobramycin/dexamethasone b.i.d.-t.i.d.) for unresponsive meibomitis
- Systemic steroids: for severe refractory cases
Step 6 - Demodex-Specific Treatment
- Tea-tree oil eyelid scrubs or hypochlorous acid eyelid cleansing agent once or twice daily for ≥6 weeks
- Mechanism: prevention of Demodex reproduction
Step 7 - Procedural (Refractory MGD)
- Thermal treatment to meibomian glands with expression
- Intense pulsed light (IPL) laser therapy
- Microblepharoexfoliation
- Probing of meibomian glands
Follow-Up
- 2-4 weeks initially, depending on severity
- Eyelid scrubs and warm compresses may be reduced to once daily as the condition improves, but often need to be maintained indefinitely
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 70-74 & 86-88; Wills Eye Manual, 7th ed., pp. 348-350; Goldman-Cecil Medicine, 26th ed., p. 4125
Blepharitis; Clinical features and management of Blepharitis, Differences between squamous and ulcerative
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Good - I have all the needed information from Kanski. The "squamous" and "ulcerative" terminology is the older classification for anterior blepharitis - squamous = seborrhoeic (non-ulcerative), ulcerative = staphylococcal. Let me compile the answer now integrating all the data including the classic comparison table.
Blepharitis: Clinical Features, Management, and Squamous vs. Ulcerative Differences
Overview
Blepharitis is a chronic, bilateral, symmetrical inflammation of the eyelid margin - one of the most common causes of ocular discomfort. It is subdivided into anterior (around lash bases) and posterior (meibomian gland dysfunction) forms, though mixed blepharitis is most common.
The classic older classification of anterior blepharitis (still used in many exams) distinguishes two sub-types:
- Squamous blepharitis = Seborrhoeic / non-ulcerative anterior blepharitis
- Ulcerative blepharitis = Staphylococcal / infective anterior blepharitis
Squamous vs. Ulcerative Blepharitis - Detailed Comparison
| Feature | Squamous (Seborrhoeic) | Ulcerative (Staphylococcal) |
|---|---|---|
| Aetiology | Seborrhoeic dermatitis; not primarily infective | Staphylococcus aureus (abnormal cell-mediated immune response to bacterial cell wall components) |
| Associated systemic condition | Seborrhoeic dermatitis (scalp, nasolabial folds, behind ears, sternum) | Atopic dermatitis |
| Scales / crusts | Soft, greasy, oily, scurf - easily removed; adhere lashes together | Hard, fibrinous, dry crusts firmly adherent to lash bases |
| Collarettes | Absent | Present - cylindrical collections around lash bases |
| Ulceration of lid margin | Absent - no ulceration | Present - removing hard crusts leaves small bleeding ulcers |
| Lash changes | Minimal lash loss (+) | Marked madarosis (lash loss ++); trichiasis; poliosis (whitening) |
| Lid margin distortion/trichiasis | Mild (+) | More severe (++) |
| Lid margin notching | Absent | Present (+) |
| Conjunctival involvement | Mild papillary conjunctivitis | Papillary conjunctivitis; phlyctenules (+) |
| Corneal changes | Inferior punctate erosions (+), vascularization (+), infiltrates (+) | Peripheral marginal infiltrates (+); more marked corneal changes |
| Hordeolum (stye) formation | Absent | Common (++) |
| Meibomian cysts | Absent | Absent |
| Tear film | Minimal foaming; dry eye (+) | Dry eye (+) |
| Red eyes | Less prominent | More prominent (immune-mediated) |
| Course | Chronic; persistent | Chronic with acute exacerbations |
| Amenability to treatment | Moderate | More amenable to treatment and remission |
Full Clinical Features
Symptoms (Common to Both)
- Burning, grittiness, mild photophobia
- Crusting and redness of lid margins, worse on waking
- Itching, tearing, foreign body sensation
- Symptoms typically worse in the morning (contrast with dry eye: worse later in day)
- No visual disturbance
- Poor tolerance of contact lenses
- Stinging more prominent in posterior disease
Signs - Staphylococcal (Ulcerative)
- Hard, fibrinous crusts firmly adherent to lash bases
- Collarettes (cylindrical collections around individual lash bases)
- Small lid margin ulcers at lash bases when crusts are removed (hence "ulcerative")
- Madarosis (loss of lashes) - marked
- Trichiasis (misdirected lashes), poliosis (whitened lashes) in long-standing cases
- Notching and scarring of lid margin
- Papillary conjunctivitis, phlyctenules
- Marginal corneal infiltrates (peripheral)
- Inferior corneal punctate epithelial erosions
- Hordeolum (stye) formation
Signs - Seborrhoeic (Squamous)
- Soft, greasy, oily scales (scurf) on lid margins
- Hyperaemic, greasy anterior lid margins
- Lashes adherent to each other (not to lid margin)
- Mild papillary conjunctivitis
- Minimal lash loss; no true ulceration
- Associated generalized seborrhoeic dermatitis of scalp, face
Signs - Posterior (Meibomian Gland Dysfunction)
- Capping of meibomian orifices with oil globules
- Pouting, recession, or plugging of meibomian gland orifices
- Hyperaemia and telangiectasis of posterior lid margin
- Expressed meibum: turbid or toothpaste-like material; in severe cases, expression impossible
- Foamy, unstable tear film; froth at lid margins or inner canthi
- Lid transillumination: gland loss and cystic ductal dilation
- Associated with acne rosacea
Signs - Demodex
- Collarettes (pathognomonic) - partially digested epithelial cells + mite eggs around lash bases
- Cylindrical dandruff-like scaling
- Confirmed by epilating a lash and examining under slit lamp (mites 0.2-0.4 mm)
Kanski's Summary Table (Table 2.4)
| Structure | Feature | Staphylococcal | Seborrhoeic | Posterior (MGD) |
|---|---|---|---|---|
| Lashes | Deposit | Hard (++) | Soft (+) | - |
| Loss/Madarosis | ++ | + | - | |
| Distortion/Trichiasis | ++ | + | - | |
| Lid margin | Ulceration | + | - | - |
| Notching | + | - | ++ | |
| Cyst | Hordeolum | ++ | - | - |
| Meibomian cyst | - | - | ++ | |
| Conjunctiva | Phlyctenule | + | - | - |
| Tear film | Foaming | - | - | ++ |
| Dry eye | + | + | ++ | |
| Cornea | Punctate erosions | + | + | ++ |
| Vascularization | + | + | ++ | |
| Infiltrates | + | + | ++ | |
| Skin association | Atopic dermatitis | Seborrhoeic dermatitis | Acne rosacea |
Secondary Complications (All Types)
- Papillary conjunctivitis
- Inferior corneal punctate erosions → scarring and vascularization
- Salzmann nodular degeneration
- Stye (hordeolum) formation
- Marginal keratitis; bacterial keratitis (especially in contact lens wearers)
- Phlyctenular eye disease
- Blepharoconjunctivitis if chronic
⚠️ Red flag: Intractable, unilateral, or asymmetric blepharitis (particularly upper vs. lower lid asymmetry) is rarely a manifestation of sebaceous carcinoma of the eyelid and requires appropriate clinical workup.
Management
Patients must understand that permanent cure is unlikely - the goal is symptom control. Treatment of anterior and posterior disease follows similar principles as both commonly co-exist.
Step 1 - Lid Hygiene (All Types - First-line, Indefinite)
- Warm compresses for 5-10 minutes b.i.d. to q.i.d. - softens inspissated crusts and meibum
- Lid margin scrubbing - using wet cotton bud, clean face-cloth, or commercial eyelid scrub pads
- For MGD: add meibomian expression by rolling finger anteriorly over lid margin
Note: Baby shampoo is NOT recommended - destabilizes the tear film and causes contact dermatitis - Perform twice daily initially; reduce frequency as condition improves but may need to be continued indefinitely
Step 2 - Topical Antibiotics (Anterior Disease)
- Sodium fusidic acid, erythromycin, bacitracin, azithromycin, or chloramphenicol ointment
- Applied to anterior lid margin after lid hygiene, at bedtime (q.h.s.)
- Used for active folliculitis; may be extended long-term
Step 3 - Artificial Tears
- Preservative-free artificial tears 4-8 times per day for associated dry eye and tear film instability
Step 4 - Oral Antibiotics (Moderate-Severe / Posterior / Refractory)
Tetracyclines reduce bacterial colonization and staphylococcal lipase production, and have anti-inflammatory effects:
| Drug | Regimen |
|---|---|
| Doxycycline | 50-100 mg b.d. × 1 week, then 50-100 mg daily × 6-24 weeks |
| Lymecycline | 408 mg once daily for up to 3 months |
| Azithromycin | 500 mg/day × 3 days, × 3 cycles with 7-day intervals |
| Minocycline | 50-100 mg once daily |
| Tetracycline | 250 mg twice daily |
⚠️ Tetracyclines are contraindicated in pregnancy, nursing mothers, and children ≤8 years. Use erythromycin 200 mg p.o. b.i.d. as the alternative.
Step 5 - Anti-inflammatory / Immunomodulatory Agents
- Cyclosporine 0.05% or 0.09% eye drops b.i.d.
- Lifitegrast 5% drops b.i.d.
- Omega-3 fatty acid oral supplementation
- Topical antibiotic-steroid combinations (e.g., tobramycin 0.3%/dexamethasone 0.1% b.i.d.-t.i.d.) for unresponsive meibomitis
Step 6 - Demodex-Specific Treatment
- Tea-tree oil eyelid scrubs or hypochlorous acid eyelid cleansing once or twice daily for ≥6 weeks
Step 7 - Procedural (Refractory MGD)
- Thermal treatment to meibomian glands with expression
- Intense pulsed light (IPL) therapy
- Microblepharoexfoliation
- Meibomian gland probing
Follow-Up
- Review at 2-4 weeks based on severity
- Lid hygiene may be reduced to once daily as condition improves but often needs indefinite maintenance
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 70-74 & 85-88 (Table 2.4); Wills Eye Manual, 7th ed., pp. 348-350; Goldman-Cecil Medicine, 26th ed., p. 4125
Tear film – structure, function, secretion and elimination
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have all the content needed for a comprehensive answer. Let me compile it.
Tear Film: Structure, Function, Secretion and Elimination
Overview
The tear film is a thin (~7-8 μm total), complex fluid layer covering the entire exposed ocular surface between blinks. It has three distinct layers, contains over 100 distinct proteins, and is constantly renewed through secretion and drained through the lacrimal drainage system.
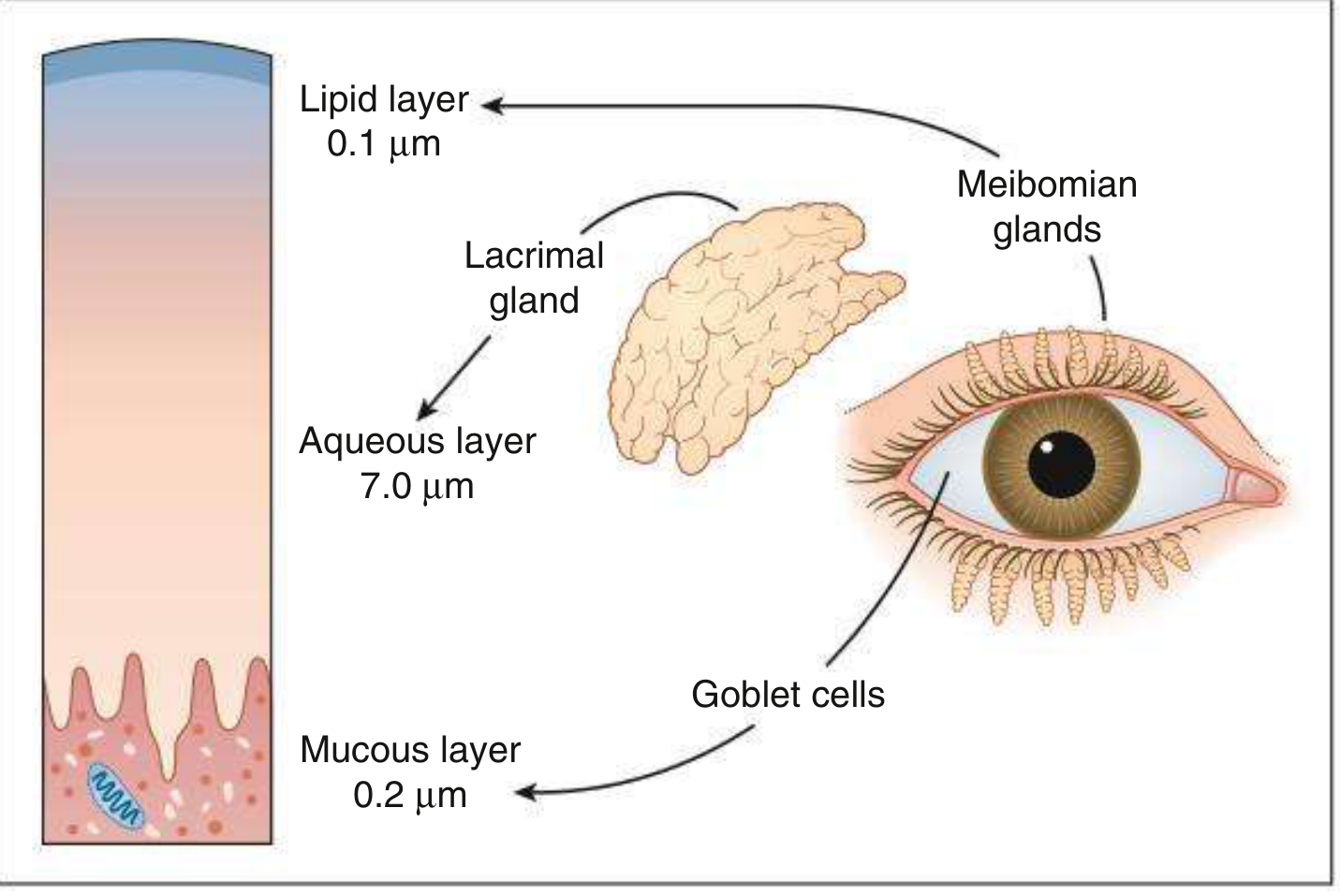
Structure: The Three Layers
Layer 1 - Lipid Layer (Outermost) - 0.1 μm
Secreted by: Meibomian glands (tarsal glands) of the eyelids; minor contribution from glands of Zeis and Moll
Composition:
- Outer non-polar phase: waxes, cholesterol esters, triglycerides
- Inner polar phase: phospholipids adjacent to the aqueous-mucin interface
- Polar lipids are bound to lipocalins within the aqueous layer - small proteins that bind hydrophobic molecules and contribute to tear viscosity
Physical notes:
- Thickness increases with forced blinking; decreases with infrequent blinking
- Lid movement during blinking is important in releasing lipids from meibomian glands
Functions:
- Prevents evaporation of the aqueous layer - maintains tear film thickness
- Acts as a surfactant allowing spread of the tear film over the ocular surface
- Provides a smooth optical interface
- Deficiency → evaporative dry eye (most common form of dry eye)
Layer 2 - Aqueous Layer (Middle) - 7.0 μm (Thickest)
Secreted by:
- Main lacrimal gland (orbital and palpebral lobes) - reflex tearing and emotional tearing
- Accessory lacrimal glands (Krause and Wolfring) - basal tear secretion; essential for maintaining the resting tear film
Composition:
- Water (~98%)
- Electrolytes (Na⁺, K⁺, Cl⁻, HCO₃⁻)
- Proteins: IgA (secretory), lysozyme, lactoferrin, lipocalin, albumin, growth factors
- Over 100 distinct proteins have been identified
Functions:
- Provides atmospheric oxygen to the avascular corneal epithelium
- Antibacterial activity via IgA, lysozyme, lactoferrin
- Washes away debris and noxious stimuli; transports leukocytes to injury sites
- Optically enhances the corneal surface by abolishing minute surface irregularities
- Maintains hydration of the ocular surface
- Deficiency → aqueous-deficient dry eye (Sjögren and non-Sjögren types)
Layer 3 - Mucous Layer (Innermost) - 0.2 μm
Secreted by:
- Conjunctival goblet cells (principal source) - secretory mucins
- Accessory lacrimal glands (minor contribution)
- Surface epithelial cells of cornea and conjunctiva - produce transmembrane mucins that form the glycocalyx (extracellular cell coat)
Composition - Two types of mucins:
| Type | Origin | Subtypes |
|---|---|---|
| Secretory mucins | Goblet cells, lacrimal gland | Gel-forming (viscous) or soluble |
| Transmembrane mucins | Corneal & conjunctival epithelial cells | Form the glycocalyx on cell surfaces |
Functions:
- Converts the hydrophobic corneal epithelium to a hydrophilic surface - essential for aqueous adherence (without mucin, aqueous tears cannot wet the corneal surface)
- Lubrication - reduces friction during blinking
- Traps and removes debris and microorganisms
Clinical significance:
- Rose Bengal staining of diseased epithelium indicates absence of transmembrane and gel mucous layers, leaving the cell surface exposed
- Goblet cell loss → mucin deficiency → tear film instability
- Causes of goblet cell loss: cicatrizing conjunctivitis, vitamin A deficiency, chemical burns, medication toxicity
Spread of the Tear Film
The tear film is mechanically distributed over the ocular surface by a neuronally controlled blinking mechanism. Three factors are required for effective resurfacing:
- Normal blink reflex
- Contact between the external ocular surface and the eyelids
- Normal corneal epithelium
At each blink, the upper eyelid sweeps downward, spreading the lipid layer, then on opening, draws the tears upward, redistributing all three layers uniformly across the cornea and conjunctiva.
Secretion
Basal Tear Secretion
- Produced continuously by the accessory lacrimal glands of Krause and Wolfring
- Rate: approximately 1-2 μL/minute under normal resting conditions
- Maintains the resting tear film without reflex stimulation
Reflex Tear Secretion
- Produced by the main lacrimal gland in response to:
- Corneal/conjunctival stimulation (noxious, tactile, chemical)
- Emotional stimuli (crying)
- Bright light
Neural Control of Secretion
Parasympathetic (main pathway):
- Preganglionic neurons arise from the lacrimal nucleus of the pons (nervus intermedius)
- Axons travel via CN VII (facial nerve) → greater superficial petrosal nerve → vidian nerve → sphenopalatine (pterygopalatine) ganglion (synapse)
- Postganglionic fibres travel via zygomatic branch of CN V₂ → anastomosis with lacrimal branch of CN V₁ → lacrimal gland
- Stimulation causes aqueous and mucus secretion
Sympathetic: Minor role; modulates rather than drives secretion
Sensory (reflex arc): Corneal stimulation → CN V₁ (ophthalmic) afferents → brainstem → parasympathetic efferents → lacrimal gland
Hormonal Regulation
- Androgens - prime hormones responsible for regulating lipid (meibomian) production; androgen deficiency is implicated in dry eye
- Oestrogens and progesterone receptors in conjunctiva and lacrimal gland - essential for normal tissue function
- Strong association between dry eye and reduced systemic androsterone sulphate and epiandrosterone sulphate
Elimination (Drainage)
Tears drain through the lacrimal drainage system as follows:
Drainage Pathway
Tear lake (lacus lacrimalis) at medial canthus
↓
Upper and lower lacrimal puncta (on lid margins, ~6 mm from medial canthus)
↓
Upper and lower canaliculi
↓
Common canaliculus (present in ~90% of people)
↓
Valve of Rosenmuller (one-way valve - prevents reflux into canaliculi)
↓
Lacrimal sac (in lacrimal fossa, medial orbital wall)
↓
Nasolacrimal duct
↓
Valve of Hasner (inferior meatus of nasal cavity, last part to canalize)
↓
Inferior nasal meatus
Physiology of Drainage (Lacrimal Pump Mechanism)
Drainage is active, not passive, driven by the lacrimal pump:
- Tears flow along the marginal tear strips medially, pooling in the lacus lacrimalis
- With each blink (orbicularis oculi contraction): canaliculi and lacrimal sac are compressed → tears are forced down the nasolacrimal duct
- When eyes open: canaliculus and sac expand → negative pressure (suction) draws tears from the conjunctival sac into the canaliculi
Causes of Drainage Failure (Epiphora)
| Mechanism | Examples |
|---|---|
| Punctal malposition | Ectropion, punctal stenosis |
| Canalicular obstruction | Scarring, infection, dacryocanaliculitis |
| Lacrimal sac/duct obstruction | Dacryocystitis, NLDO, nasal pathology |
| Lacrimal pump failure | Lower lid laxity, facial nerve (CN VII) palsy, orbicularis weakness |
| Hypersecretion (paradoxical) | Dry eye causing reflex tearing, corneal/conjunctival inflammation |
Tear Film Break-Up Time (BUT)
A key measure of tear film stability:
- Normal BUT: >10 seconds
- Abnormal (dry eye): ≤10 seconds
- Measured by instilling fluorescein and timing from a complete blink to the first random dry spot appearing in the tear film under cobalt blue slit lamp illumination
Marginal Tear Meniscus (Strip)
- A crude measure of aqueous tear volume
- Normal: 0.2-0.4 mm in height
- Dry eye: <0.25 mm or absent
Tear Film Regulation Summary
| Component | Regulated By |
|---|---|
| Lipid layer thickness | Meibomian gland function; blink frequency; androgens |
| Aqueous secretion | Parasympathetic (CN VII), reflex afferents (CN V), emotional state |
| Basal secretion | Accessory lacrimal glands (Krause & Wolfring) |
| Mucin production | Goblet cells; vitamin A; conjunctival health |
| Drainage | Lacrimal pump (orbicularis, CN VII), drainage system patency |
Mechanism of Dry Eye Disease (Integration)
The four core interrelated mechanisms responsible for dry eye are:
- Tear instability
- Tear hyperosmolarity
- Inflammation (present in 80% of KCS patients; both cause and consequence; rationale for steroid therapy)
- Ocular surface damage
These create a self-perpetuating cycle of ocular surface disease.
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 171-178 (Fig. 5.1); Localization in Clinical Neurology, 8th ed., p. 777; K.J. Lee's Essential Otolaryngology, p. 4115
Bell's palay
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from Adams & Victor, Harrison's 22nd Ed, and Scott-Brown's. Let me now compile the full answer.
Bell's Palsy
Definition
Bell's palsy is an acute, idiopathic, unilateral lower motor neuron (LMN) facial nerve (CN VII) palsy diagnosed by exclusion of all other known causes. It is the most common disease of the facial nerve and the most common cause of acute facial paralysis overall.
Epidemiology
- Annual incidence: 23-40 per 100,000 (~1 in 60 persons in a lifetime)
- Affects men and women approximately equally
- Occurs at all ages and all times of the year
- Risk factors:
- Pregnancy (particularly 3rd trimester and first 2 weeks postpartum; up to 3x increased risk cited)
- Diabetes mellitus
- Hypertension
- Recurrence reported in ~7% of cases
Aetiology and Pathophysiology
The aetiology is idiopathic by definition, but a viral cause is the dominant theory:
- Herpes simplex virus type 1 (HSV-1): HSV-1 DNA has been identified in endoneurial fluid surrounding CN VII in surgical specimens from Bell's palsy patients; animal studies replicated facial paralysis by HSV inoculation. HSV-1 reactivation in the geniculate ganglion is the most widely accepted mechanism.
- Varicella-zoster virus (VZV): Implicated in up to one-third of cases and may be the second most common cause (when VZV is the cause with vesicular eruption, it becomes Ramsay Hunt syndrome, a separate diagnosis).
- Other viruses: HHV-6 (higher DNA copies in saliva of Bell's patients vs. controls), SARS-CoV-2, HIV seroconversion, and others have been implicated less commonly.
- Pathology: Inflammation and oedema → entrapment of the swollen nerve in the narrow labyrinthine segment of the facial canal → ischaemia and demyelination or axonal degeneration
Note: A recent Cochrane review showed antivirals against HSV are no more effective than placebo for complete recovery alone - this has cast some doubt on HSV as the sole causative agent.
Anatomy Relevant to Bell's Palsy
The facial nerve (CN VII) exits the brainstem at the pontomedullary junction, passes through the cerebellopontine angle, enters the internal auditory meatus, then travels through the facial canal in the petrous temporal bone (with the geniculate ganglion at its genu), before exiting through the stylomastoid foramen. The narrowest portion is the labyrinthine segment - this is where entrapment most commonly occurs.
The nerve supplies:
- All muscles of facial expression
- Stapedius muscle (middle ear)
- Taste to anterior 2/3 of tongue (via chorda tympani)
- Secretomotor to lacrimal, submandibular, and sublingual glands
- Cutaneous sensation to small area behind the ear
Clinical Features
Onset
- Acute - maximal weakness attained in 48 hours as a general rule; practically all cases reach maximum paralysis within 3-4 days
Symptoms
| Symptom | Explanation |
|---|---|
| Unilateral LMN facial weakness | All ipsilateral facial muscles including forehead (distinguishes LMN from UMN) |
| Pain behind the ear | May precede paralysis by 1-2 days; occasionally intense and persistent |
| Impaired taste (anterior 2/3 tongue) | Present in most; indicates lesion proximal to where chorda tympani joins CN VII; rarely persists beyond 2nd week |
| Hyperacusis / sound distortion | Ipsilateral ear; indicates paralysis of stapedius muscle |
| Facial fullness or numbness | Common subjective complaint; in a minority, true hypoaesthesia in trigeminal distribution |
| Inability to close eye | Risk of exposure keratopathy; lagophthalmos |
| Bell's phenomenon | On attempted eyelid closure, the globe reflexly rotates upward and outward - protective reflex |
Signs
- Complete ipsilateral LMN facial palsy: weakness of upper and lower face (forehead involved - key distinction from UMN palsy)
- Inability to wrinkle forehead, raise eyebrow, close eye, show teeth, purse lips, inflate cheeks
- Loss of nasolabial fold; drooping of mouth corner
- Ectropion of lower lid, epiphora
- Normal otoscopy (essential - abnormal otoscopy = not Bell's palsy)
- Normal hearing (abnormal hearing = consider Ramsay Hunt or other cause)
LMN vs. UMN Facial Palsy: Key Distinction
| Feature | LMN (Bell's palsy) | UMN (e.g., stroke) |
|---|---|---|
| Forehead involvement | Yes - forehead weak (cannot wrinkle) | Spared - forehead wrinkles normally |
| Mechanism | Forehead muscles have only contralateral cortical input | Forehead muscles have bilateral cortical input |
| Emotional vs. voluntary movement | Both equally affected | Dissociation possible (emotional preserved, voluntary lost) |
| Associated findings | Isolated, taste/hyperacusis may be present | Hemiplegia, aphasia may co-exist |
Investigations
Clinical diagnosis in typical cases - no investigations required if:
- Typical acute presentation
- No risk factors for other causes
- No vesicular eruption in external ear canal (excludes Ramsay Hunt)
- Normal neurological examination except facial nerve
In atypical or uncertain cases:
- MRI with gadolinium: swelling and enhancement of the geniculate ganglion and facial nerve in the temporal bone (Fig. 452-4 Harrison's); enhancement in the labyrinthine, tympanic, and mastoid segments. Note: similar enhancement seen in Lyme disease, sarcoidosis, perineural malignancy
- ESR / CRP
- Fasting glucose / HbA1c (diabetes)
- Lyme serology (in endemic areas; Lyme may cause bilateral facial palsy)
- HIV serology
- ACE level + chest imaging (sarcoidosis)
- Lumbar puncture (Guillain-Barré consideration - may cause bilateral facial palsy)
- EMG/nerve conduction studies: useful prognostically after 10 days - evidence of denervation = axonal degeneration, indicates prolonged recovery
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Ramsay Hunt syndrome (VZV reactivation) | Vesicular eruption in external auditory canal, pinna, palate; sensorineural hearing loss; more severe palsy; worse prognosis |
| Lyme disease (Borrelia burgdorferi) | Endemic area exposure; may be bilateral; systemic features; Lyme serology positive |
| Otitis media / mastoiditis | Abnormal otoscopy, ear pain, fever |
| Parotid tumour | Slow onset; palpable mass; no taste/hyperacusis involvement |
| Acoustic neuroma | CN VIII involvement; progressive hearing loss; MRI shows mass |
| Sarcoidosis | Bilateral facial palsy; systemic features; raised ACE; hilar lymphadenopathy |
| Guillain-Barré syndrome | Bilateral; ascending weakness; areflexia; CSF albuminocytological dissociation |
| Cholesteatoma / middle ear disease | Abnormal otoscopy |
| Melkersson-Rosenthal syndrome | Recurrent facial palsy + facial oedema + fissured tongue |
| Leprosy | In endemic regions; skin lesions; thickened peripheral nerves |
Prognosis
- 70% recover completely within 1-2 months
- 85% achieve near-normal function overall
- Incomplete paralysis in first 5-7 days = most favourable prognostic sign
- Return of taste within first week = good prognostic sign (recovery of taste precedes motor recovery)
- EMG after 10 days: evidence of denervation → axonal degeneration → delay of ~3 months before regeneration; may be incomplete
- MRI: pronounced contrast enhancement of facial nerve = worse prognosis
- Children: recovery rate ~90% regardless of treatment
Complications of incomplete recovery:
- Synkinesis (aberrant nerve regeneration - eye blinks when mouth moves, "crocodile tears" on eating)
- Hemifacial spasm
- Persistent facial weakness and asymmetry
Treatment
1. Eye Protection (Immediate - Prevent Corneal Damage)
- Paper tape to depress upper eyelid during sleep
- Lubricating eye drops (artificial tears) during the day
- Lubricating ointment at night
- Moisture chamber / eye patch if lagophthalmos is severe
- If Bell's phenomenon is absent (cornea not protected on attempted closure): more aggressive corneal protection required
2. Corticosteroids (Strong Evidence - First-line)
- Prednisone 60-80 mg daily for the first 5 days, then tapered over the next 5 days (total 10-day course)
- Start as early as possible (ideally within 72 hours of onset)
- Modestly shortens recovery and improves functional outcome
- Supported by large randomized controlled trials
- Children: recovery rate so high (90%) that steroids may not be necessary
3. Antiviral Therapy (Selective Use)
- Valacyclovir 1000 mg daily for 5-7 days OR acyclovir 400 mg five times daily for 10 days
- Large randomized trials found no added benefit of antivirals over steroids alone in typical Bell's palsy
- Use antivirals if: vesicular lesions in palate or external auditory canal (suggests VZV - Ramsay Hunt); severe/complete palsy; immunocompromised patient
- Cochrane review: antivirals alone no more effective than placebo
4. Physiotherapy
- Massage of weakened muscles
- Facial exercises
5. Surgical Decompression
- Controversial and rarely performed
- Transmastoid decompression considered in:
- Severe complete palsy with EMG evidence of degeneration
- No recovery by 3-4 months
- Selected cases with complete denervation
6. Cosmetic / Rehabilitative Surgery (Permanent Paralysis)
- Various procedures to restore facial symmetry
- Gold weight implantation in upper lid for lagophthalmos
- Facial nerve grafting, muscle transfer
Ophthalmic Complications and Management
| Complication | Management |
|---|---|
| Lagophthalmos (incomplete eye closure) | Tape at night, lubricants, moisture chamber |
| Exposure keratopathy | Lubricants, bandage contact lens, tarsorrhaphy if severe |
| Ectropion (lower lid) | Surgical correction if permanent |
| Epiphora | Treat underlying lid malposition |
| Absent Bell's phenomenon | Especially aggressive corneal protection |
Sources: Adams & Victor's Principles of Neurology, 12th ed., p. 1371; Harrison's Principles of Internal Medicine, 22nd ed., p. 3598; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Bradley & Daroff's Neurology in Clinical Practice
Proptosis Orbital cellulitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have all the content needed. Now let me compile the comprehensive answer covering both topics.
Proptosis
Definition
Proptosis = abnormal anterior protrusion of the eyeball out of the orbit. The term exophthalmos is used specifically for proptosis of the eyeball (the two terms are often used interchangeably in clinical practice).
- The intraorbital optic nerve is 25 mm long vs. only 18 mm distance from the back of the globe to the optic canal - this slack allows significant forward globe displacement before the nerve is stretched
Measurement
- Hertel exophthalmometer (most common) - uses the lateral orbital rim as a reference point; measures corneal apex protrusion
- Luedde exophthalmometer - simpler, single-eye measurement
- Normal value: ≤20 mm
- Proptosis: readings >20 mm OR ≥2-3 mm asymmetry between the two eyes (even if both values are within normal range)
- Measurements taken at rest and during Valsalva (to detect venous anomalies)
Direction of Proptosis and Implied Pathology
| Direction | Name | Likely Cause |
|---|---|---|
| Straight forward | Axial proptosis | Intraconal (within muscle cone) lesion - cavernous haemangioma, optic nerve tumour (glioma, meningioma) |
| Forward + sideways | Proptosis + dystopia | Extraconal lesion - lacrimal gland tumour (down and in), frontal sinus mucocele (down and out) |
| Pulsatile | Pulsating proptosis | Arteriovenous fistula (carotid-cavernous), orbital roof defect (transmits CSF pulsations from brain) |
| Positional/intermittent | Variable proptosis | Orbital venous anomaly, capillary haemangioma (increases with Valsalva, dependent head position, jugular compression) |
Dystopia = displacement of the globe in the coronal plane (horizontal or vertical), measured from the midline to the centre of the pupil.
Pseudoproptosis (False Impression of Proptosis)
- Facial asymmetry
- Enlarged globe (high myopia, buphthalmos)
- Eyelid retraction (making eye appear to bulge)
- Contralateral enophthalmos (the normal eye appears proptotic by comparison)
Causes of Proptosis
Classified by Aetiology
| Category | Examples |
|---|---|
| Inflammatory / Infective | Orbital cellulitis (most common cause in children), idiopathic orbital inflammatory disease (orbital pseudotumour), thyroid eye disease (most common cause in adults), orbital myositis, dacryoadenitis |
| Vascular | Cavernous haemangioma (most common benign orbital tumour in adults), lymphangioma, carotid-cavernous fistula, acute orbital haemorrhage, orbital varix |
| Neoplastic - Primary | Optic nerve glioma (children), optic nerve sheath meningioma, lacrimal gland tumours, lymphoma, rhabdomyosarcoma (most common primary orbital malignancy in children) |
| Neoplastic - Secondary | Metastases (breast, lung, prostate), neuroblastoma (children), leukaemia |
| Endocrine | Thyroid eye disease (Graves' orbitopathy) - commonest cause of bilateral proptosis in adults |
| Traumatic | Orbital haemorrhage (retrobulbar haematoma), orbital emphysema, orbital fracture |
| Cystic | Dermoid cyst (most common orbital cyst), mucocele of paranasal sinus |
| Structural | Shallow orbit (craniofacial syndromes - Crouzon, Apert) |
Key Clinical Mnemonics for Causes
SPINE (common causes):
- Sinusitis → orbital cellulitis
- Pseudotumour (idiopathic orbital inflammation)
- Infection (orbital cellulitis)
- Neoplasm
- Endocrine (thyroid eye disease)
Clinical Assessment of Proptosis
Symptoms
- Protrusion of the eye
- Diplopia (double vision)
- Reduced vision (compressive optic neuropathy)
- Periorbital pain
- Exposure symptoms (dryness, grittiness)
Signs to Elicit
- Degree - Hertel exophthalmometer
- Direction - axial vs. dystopia
- Reducibility - retropulsion; non-reducible suggests fixed or rapidly expanding mass
- Pulsation + bruit (auscultate over closed lids) - AV fistula
- Positional change with Valsalva - venous lesion
- Lid retraction vs. true proptosis
- Ophthalmoplegia - restrictive vs. neurological (forced duction test; differential IOP test)
- Optic nerve function - VA, colour vision, RAPD, visual fields
- Fundus - disc swelling, optic atrophy, opticociliary collaterals, choroidal folds
Investigations for Proptosis
- CT orbit - bone detail, sinuses, calcification (optic nerve meningioma - "tram-track" sign)
- MRI orbit - soft tissue definition, optic nerve
- Thyroid function tests (TFTs), thyroid antibodies
- CXR / chest CT - sarcoid, lymphoma
- Biopsy if neoplasm suspected
Orbital Cellulitis
Definition
Orbital cellulitis is a serious bacterial infection of the soft tissues posterior to the orbital septum (postseptal). It is potentially sight- and life-threatening and represents a true ophthalmological emergency.

Preseptal vs. Postseptal (Orbital) Cellulitis - Critical Distinction
| Feature | Preseptal (Periorbital) Cellulitis | Orbital (Postseptal) Cellulitis |
|---|---|---|
| Location | Anterior to orbital septum | Posterior to orbital septum |
| Proptosis | Absent | Present |
| Ophthalmoplegia | Absent | Present (painful) |
| Visual loss | Absent | May be present |
| RAPD | Absent | May be present |
| Fever | Mild | Often marked |
| Severity | Less serious | Sight- and life-threatening |
| Treatment | Oral antibiotics (outpatient in mild cases) | IV antibiotics + hospital admission |
| CT changes | Preseptal soft tissue swelling only | Fat stranding, subperiosteal collection, intraconal changes |
The orbital septum is the critical anatomical barrier - a fibrous membrane extending from the orbital rim to the tarsal plates. Infection posterior to this = true orbital cellulitis.
Epidemiology
- Can occur at any age but more common in children
- Most common source: paranasal sinusitis (especially ethmoid sinusitis)
- Perforation of the thin lamina papyracea (medial orbital wall) is the usual route from the ethmoid sinus
Aetiology / Sources of Infection
| Source | Notes |
|---|---|
| Paranasal sinusitis | Most common - especially ethmoiditis; ethmoid sinus separated from orbit by thin lamina papyracea |
| Preseptal cellulitis extension | Direct spread posteriorly through septum |
| Dacryocystitis | Via nasolacrimal system |
| Dacryoadenitis | Lacrimal gland infection |
| Dental abscess | Aggressive mixed aerobes and anaerobes |
| Facial/periorbital skin infection | Via venous anastomoses |
| Orbital/ocular trauma | Orbital fracture, retained foreign body, penetrating trauma |
| Post-surgical | Eyelid, orbital, sinus, or ocular surgery |
| Haematogenous spread | Systemic bacteraemia (less common) |
| Cavernous sinus thrombosis | Retrograde spread |
Causative Organisms
| Patient Group | Organisms |
|---|---|
| Adults | Staphylococcus aureus, Streptococcus spp., Bacteroides spp. |
| Children | Haemophilus influenzae (rare in vaccinated); S. aureus, S. pneumoniae |
| Post-trauma | Gram-negative rods |
| Dental source | Mixed aggressive aerobes + anaerobes |
| Diabetic / immunocompromised | Fungi - Mucor (zygomycosis/mucormycosis), Aspergillus |
| General | Often polymicrobial; MRSA must be considered |
| Unimmunized children | H. influenzae type b |
⚠️ Zygomycosis (Mucormycosis): Rapidly progressive, life-threatening sino-orbital infection in diabetics (especially ketoacidotic) or immunocompromised. Presents with severe pain, ophthalmoplegia, rapid visual loss, nasal eschar. Emergency surgical debridement + antifungals required.
Clinical Features
Symptoms
- Rapid onset of periorbital pain, worsened by eye movement
- Swelling of the eye/lids
- Malaise, fever
- Visual impairment, double vision
- Recent history of nasal, sinus, or respiratory symptoms
- Headache (raised concern for intracranial extension)
Signs
| Sign | Detail |
|---|---|
| Pyrexia | Often marked |
| Eyelid oedema | Tender, firm, erythematous, warm - may spread to contralateral lids |
| Proptosis | Common; may be obscured by lid swelling; non-axial if abscess present |
| Painful ophthalmoplegia | Restriction of extraocular movements with pain - key distinguishing feature from preseptal |
| Chemosis | Conjunctival oedema and injection |
| Subconjunctival haemorrhage | May be present |
| Reduced VA + colour vision | Suggests optic nerve compression |
| RAPD | "Almost certain" evidence of optic nerve compression when present in a previously normal eye |
| Choroidal folds + disc swelling | On fundoscopy - orbital congestion |
| Raised IOP | Orbital compartment syndrome |
Investigations
- CT orbits, sinuses, and brain with contrast - mandatory; confirms diagnosis; identifies:
- Adjacent sinusitis (typically at least ethmoiditis)
- Subperiosteal abscess (SPA) - most common on medial orbital wall
- Orbital abscess (intraconal)
- Intracranial extension
- Retained foreign body
- Full blood count (FBC/CBC) with differential
- Blood cultures (before antibiotics)
- Culture of nasal discharge
- MRI - sometimes used additionally for soft tissue detail
- Lumbar puncture if meningeal/cerebral signs
- Tetanus immunization status (if traumatic)
- Gram stain and culture of any wound drainage
Complications
Ocular Complications
- Optic neuropathy (compressive - most feared vision-threatening complication)
- Exposure keratopathy
- Raised IOP / orbital compartment syndrome
- Central retinal artery or vein occlusion
- Endophthalmitis
Orbital Complications
- Subperiosteal abscess (SPA) - most commonly on medial orbital wall; requires drainage
- Orbital abscess - intraconal; requires urgent surgical drainage
Intracranial Complications (uncommon - 3-4% - but life-threatening)
- Cavernous sinus thrombosis (headache + CN III, IV, VI palsies → bilateral involvement)
- Meningitis
- Brain abscess
- Subdural empyema
- Epidural abscess
- Frontal bone osteomyelitis
Differential Diagnosis of an Acutely Inflamed Orbit (Kanski Table 4.1)
| Category | Conditions |
|---|---|
| Infection | Bacterial orbital cellulitis, fungal orbital infection, dacryocystitis, dacryoadenitis |
| Vascular | Acute orbital haemorrhage, cavernous sinus thrombosis, carotid-cavernous fistula |
| Neoplasia | Rhabdomyosarcoma, retinoblastoma, lacrimal gland tumour, lymphoma, neuroblastoma, leukaemia |
| Endocrine | Thyroid eye disease (rapid onset) |
| Non-neoplastic inflammation | Idiopathic orbital inflammation (pseudotumour), Tolosa-Hunt syndrome, orbital myositis, HZO, sarcoidosis, vasculitides, scleritis, ruptured dermoid cyst |
Treatment
1. Immediate Admission + Specialist Consultation (Mandatory)
- Hospital admission in all cases of true orbital cellulitis
- Urgent ophthalmology review (at minimum 4-hourly monitoring of optic nerve function)
- ENT/otolaryngology consultation (sinus disease management)
- Paediatric specialist input for children
- Infectious disease consultation in atypical, severe, or unresponsive cases
- Neurosurgery if meningeal signs or intracranial extension suspected
- Oral maxillofacial surgery if dental source (aggressive spread, cavernous sinus risk)
2. Optic Nerve Monitoring (Every 4 Hours Minimum)
- Visual acuity
- Colour vision
- Light brightness appreciation
- Pupillary reactions (RAPD)
- Deterioration → consider emergency surgical intervention
3. Intravenous Antibiotics (First-line)
Broad-spectrum covering Gram-positive, Gram-negative, and anaerobic organisms:
| Drug | Role |
|---|---|
| Ceftazidime (3rd-gen cephalosporin) | Typical first choice (Kanski) |
| Vancomycin | MRSA coverage |
| Piperacillin-tazobactam | Broad spectrum |
| Ticarcillin-clavulanate / Imipenem / Meropenem | Severe/polymicrobial cases |
| Metronidazole or clindamycin | Added for anaerobic coverage (dental source) |
- IV antibiotics until apyrexial for 4 days, then 1-3 weeks oral completion
- Mark extent of skin erythema with a surgical pen - to monitor progression or regression
4. Adjuvant Measures
- Topical nasal decongestant (e.g., oxymetazoline) for sinus drainage
- Nasal steroids (consider)
5. Surgery (Indications)
| Procedure | Indication |
|---|---|
| Drainage of subperiosteal/orbital abscess | Early consideration; failure to improve on IV antibiotics |
| Surgical sinus drainage | Very severe sinus disease; failure to respond |
| Emergency lateral canthotomy and cantholysis | Raised IOP or optic neuropathy (orbital compartment syndrome) |
| Biopsy | Atypical clinical picture |
| Debridement | Mucormycosis/fungal infection (aggressive - combined with IV antifungals) |
Follow-Up
- Close review based on optic nerve monitoring every 4 hours initially
- Oral antibiotics continued for 1-3 weeks after discharge
- ENT follow-up for underlying sinus disease
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 129-131 & 140-141; Wills Eye Manual, 7th ed., pp. 437-441; Tintinalli's Emergency Medicine, 9th ed., p. 1581
This is a shared conversation. Sign in to Orris to start your own chat.