Treatment kf aplenic abscess with 975 cc
Reading File
Finding Sources
Searching PubMed
"splenic abscess" treatment management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a thorough answer. Here is a comprehensive summary on the treatment of splenic abscess.
Treatment of Splenic Abscess
(Note: I interpret "975 cc" in your query as likely a typo for "975 cc" as an abscess size, or possibly a dictation artifact. The treatment approach below covers all sizes and clinical scenarios.)
Background
Splenic abscess is uncommon (incidence 0.14-0.76%) but carries significant mortality if untreated. It arises most often from:
- Hematogenous spread - infective endocarditis, IV drug use, bacteremia
- Contiguous infection - pancreatic necrosis, bowel perforation
- Hemoglobinopathy (e.g., sickle cell disease)
- Immunosuppression - HIV, chemotherapy, chronic steroids
- Trauma
CT scan with IV contrast (95% sensitivity/specificity) is the gold-standard imaging and also characterizes the abscess as unilocular vs. multilocular.
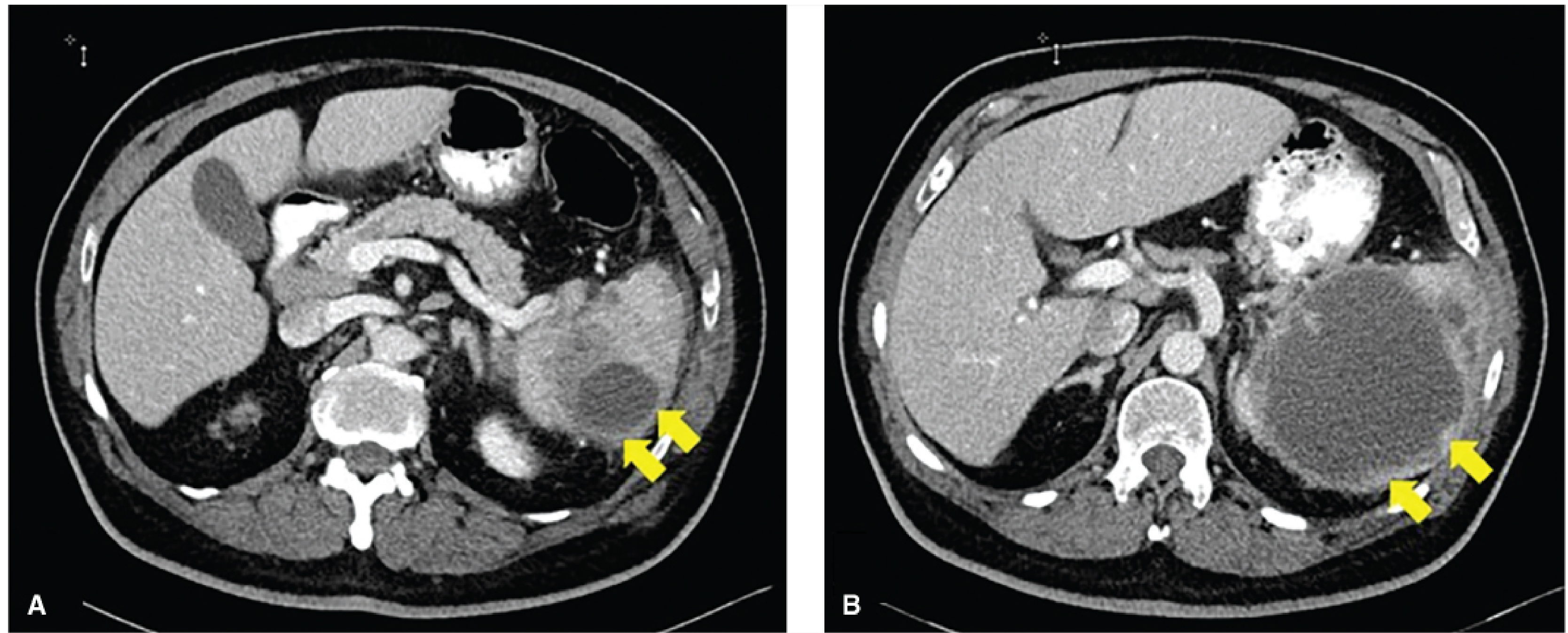
Splenic abscess on contrast CT - Fischer's Mastery of Surgery, 8th ed.
Treatment Principles
Treatment rests on three pillars:
1. Antibiotics
- Start empiric broad-spectrum antibiotics within 1 hour for septic patients (Surviving Sepsis Guidelines)
- Most abscesses are polymicrobial, so broad initial coverage is essential
- Common organisms: Streptococcus spp., Staphylococcus aureus, E. coli, Salmonella, Klebsiella, Proteus, Bacteroides, Candida spp.
- In immunocompromised patients, add coverage for Candida and Mycobacterium
- Continue antibiotics for a minimum of 14 days; continue until percutaneous drains are removed
- Narrow therapy once culture/sensitivity results available
2. Percutaneous Drainage (Preferred First-Line for Unilocular Abscess)
- Performed under CT or ultrasound guidance by interventional radiology
- Success rate: 67-100% in reported series
- Indications: Unilocular abscess, hemodynamically stable patient
- Contraindication to note: Avoid transpleural drainage (risk of empyema/seeding)
- Send drain cultures for microbiologic identification
- If unilocular - most likely to achieve complete resolution with this approach
- If multilocular - often requires multiple drains and may ultimately still need splenectomy
3. Splenectomy (Definitive/Salvage)
| Situation | Role of Splenectomy |
|---|---|
| Failure of percutaneous drainage | Recommended |
| Multiloculated abscess | Often required; open or laparoscopic |
| Hemodynamically unstable (unable to tolerate IR) | Emergent open splenectomy |
| Multiple abscesses throughout spleen | Preferred (spleen is part of overwhelming sepsis) |
| Pediatric patients | Percutaneous drainage preferred to preserve splenic function |
- Laparoscopic splenectomy is safe and feasible for splenic abscess and is the gold standard for elective/stable cases
- Open splenectomy is used for hemodynamic instability or when laparoscopic approach fails
- All patients undergoing splenectomy should receive vaccinations for encapsulated organisms (pneumococcus, H. influenzae type B, meningococcus, seasonal flu) - ideally at least 2 weeks pre-operatively
Treatment Algorithm (Summary)
Splenic Abscess Confirmed (CT/US)
│
▼
Broad-spectrum antibiotics + Blood cultures + Source control work-up
│
├── Hemodynamically UNSTABLE ──► Emergent open splenectomy
│
└── Hemodynamically STABLE
│
├── Unilocular ──► Percutaneous image-guided drainage
│ │
│ Success ──► Continue abx × ≥14 days
│ Failure ──► Splenectomy
│
└── Multilocular / Multiple abscesses ──► Splenectomy (lap or open)
Post-Splenectomy Care
- Monitor for early complications: intra-abdominal abscess, pleural effusion, empyema (treat with image-guided drainage)
- Long-term: risk of overwhelming post-splenectomy sepsis (OPSS) - mitigated by vaccination
Sources:
- [Fischer's Mastery of Surgery, 8th ed.](Fischer's Mastery of Surgery, 8th ed.) - Chapter 186
- Schwartz's Principles of Surgery, 11th ed. - p. 1557
- Mulholland & Greenfield's Surgery, 7th ed. - p. 3840
- [Current Surgical Therapy, 14th ed.](Current Surgical Therapy) - Chapter on Splenic Abscess
- Maingot's Abdominal Operations - p. 1267
- [Bailey & Love's Short Practice of Surgery, 28th ed.](Bailey & Love's) - p. 1246
This is a shared conversation. Sign in to Orris to start your own chat.