Ulnar never course it's anatomy it's supply its branches what all plasy is found features it's investigation causes it's treatment what's ulnar paradox
Reading File
Finding Sources
Finding Sources
Searching Images
ulnar nerve course anatomy branches
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Ulnar Nerve — Complete Overview
1. Origin & Root Value
- Roots: C8, T1
- Cord: Medial cord of the brachial plexus
- Associated with the medial brachial and medial antebrachial cutaneous nerves at its origin.
2. Course
Axilla / Arm
- Enters the arm with the median nerve and axillary artery, lying medial to the axillary artery.
- No branches in the arm.
- At the mid-arm, pierces the medial intermuscular septum and enters the posterior compartment, running anterior to the medial head of triceps brachii.
Elbow
- Passes posterior to the medial epicondyle of the humerus in the ulnar groove (bony sulcus between medial epicondyle and olecranon). This is where the nerve is superficial and palpable.
- Enters the forearm by passing between the two heads of flexor carpi ulnaris (the humeral-ulnar aponeurosis), forming the roof of the cubital tunnel.
Forearm
- Runs in the plane between flexor carpi ulnaris (medially) and flexor digitorum profundus (laterally/deep).
- Ulnar artery lies lateral to the nerve in the distal two-thirds of the forearm.
- About 5–8 cm proximal to the wrist, the dorsal cutaneous branch exits and passes posteriorly deep to the FCU tendon.
Wrist / Hand
- Enters the hand superficial to the flexor retinaculum, lateral to the pisiform — through Guyon's canal (ulnar tunnel), bounded by the pisiform and hook of hamate, roofed by the volar carpal ligament/palmaris brevis.
- Divides into a superficial (sensory) branch and a deep (motor) branch.
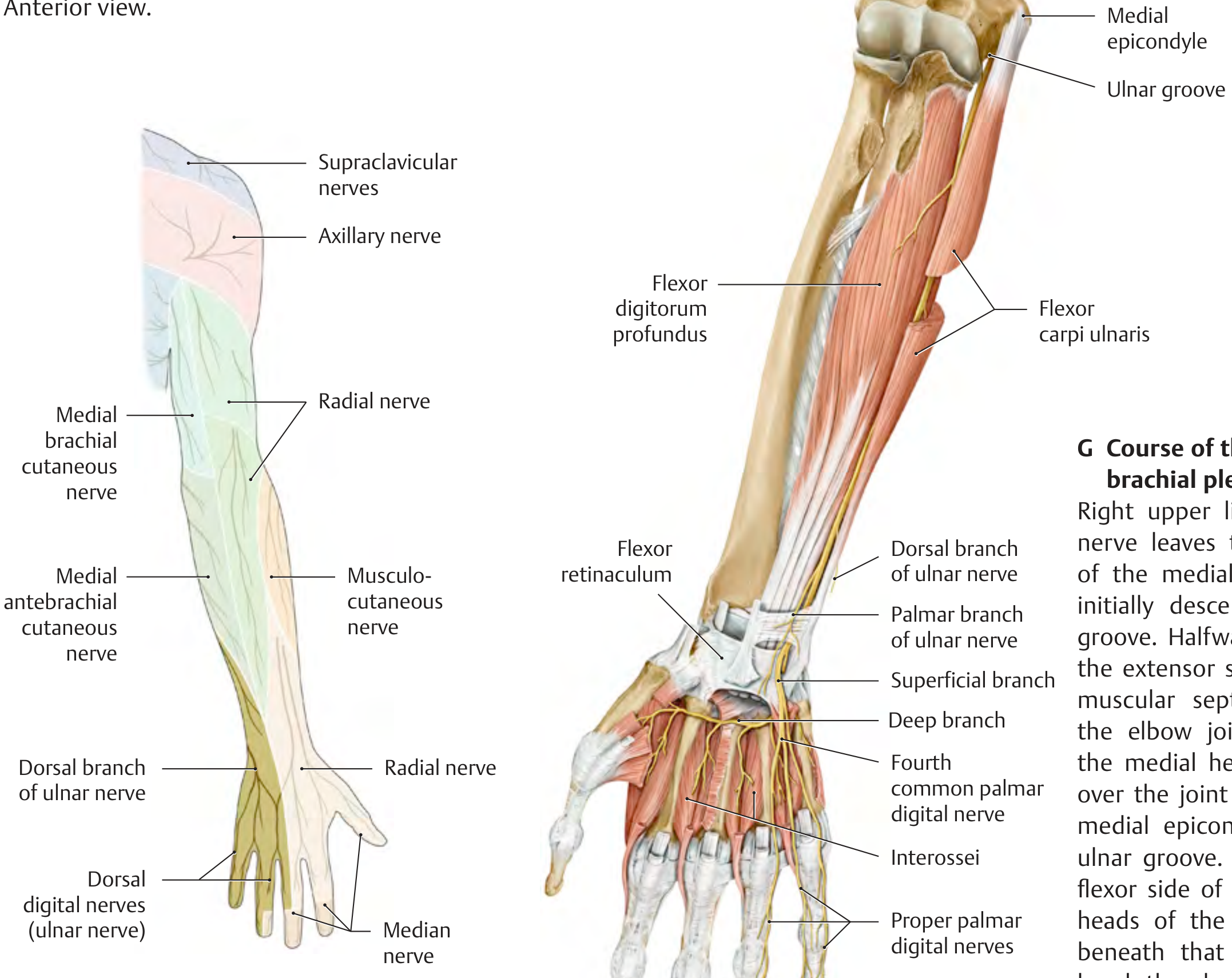
Course of the ulnar nerve — showing dorsal branch, palmar branch, deep motor branch, superficial branch, interossei, and digital branches. — General Anatomy and Musculoskeletal System (THIEME Atlas)
3. Branches
| Region | Branch | Function |
|---|---|---|
| Arm | None | — |
| Elbow/proximal forearm | Muscular branch to flexor carpi ulnaris | Motor |
| Muscular branch to medial half of FDP (ring & little fingers) | Motor | |
| Mid-forearm | Palmar cutaneous branch | Sensory — medial palm |
| Distal forearm (~5–8 cm proximal to wrist) | Dorsal cutaneous branch | Sensory — dorsum of medial hand, dorsal little finger and ulnar half of ring finger |
| Guyon's canal | Divides into: | |
| Superficial branch | Sensory — palmar surface of little finger and ulnar half of ring finger; motor to palmaris brevis | |
| Deep motor branch | Motor — hypothenar muscles (abductor digiti minimi, flexor digiti minimi, opponens digiti minimi), all interossei (4 dorsal, 3 palmar), 3rd and 4th lumbricals, adductor pollicis, deep head of flexor pollicis brevis |
4. Motor Supply (Summary)
Forearm:
- Flexor carpi ulnaris (FCU)
- Flexor digitorum profundus — medial half (ring & little fingers)
Hand (via deep branch):
- Hypothenar muscles: abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi
- All 4 dorsal interossei
- All 3 palmar interossei
- 3rd and 4th lumbricals
- Adductor pollicis
- Deep head of flexor pollicis brevis
Mnemonic — "LOAF" is for the median nerve; ulnar nerve controls all the other intrinsics.
5. Sensory Supply
| Area | Branch |
|---|---|
| Dorsum of medial hand, dorsal little & ring finger | Dorsal cutaneous branch (exits forearm) |
| Medial palm (proximal) | Palmar cutaneous branch (exits mid-forearm) |
| Palmar little finger + ulnar half of ring finger | Superficial terminal branch (via Guyon's canal) |
Key point: Because the palmar and dorsal cutaneous branches leave the nerve proximal to Guyon's canal, a wrist lesion spares dorsal hand sensation and medial palm sensation.
6. Ulnar Nerve Palsies
A. Elbow Palsy (Cubital Tunnel Syndrome / Ulnar Groove Syndrome)
Causes:
- Compression of nerve by thickened humeral-ulnar aponeurosis (cubital tunnel syndrome)
- External pressure from resting a flexed elbow on a hard surface
- Nerve subluxation over medial epicondyle
- Fracture/dislocation of elbow
- Tardy ulnar palsy — delayed palsy from old elbow fracture causing cubitus valgus deformity
- Osteophytes from elbow arthritis
- Ganglion, lipoma, Charcot elbow
- Occupations with repeated elbow flexion
Features:
- Sensory: numbness/tingling of little finger and ring finger (ulnar 1½ digits); sensory loss includes dorsum of hand (dorsal branch intact)
- Weakness of FCU and FDP to ring/little (forearm muscles affected)
- Intrinsic hand muscle weakness + wasting (especially 1st dorsal interosseous)
- Ulnar claw hand (4th and 5th fingers) — but less pronounced than wrist lesion (ulnar paradox — see below)
- Froment's sign — when pinching paper between thumb and index finger, distal phalanx of thumb flexes involuntarily (flexor pollicis longus compensates for weak adductor pollicis)
- Wartenberg's sign — little finger abducted due to weakness of 3rd palmar interosseous
- Pain around elbow; Tinel's sign at elbow
- Sensory loss does NOT extend above the wrist
B. Wrist Palsy (Guyon's Canal Syndrome)
Causes:
- Ganglion cyst (most common)
- Chronic pressure: hand tools, bicycle handlebars, canes, excessive push-ups
- Fracture of pisiform or hook of hamate
- Rheumatoid arthritis
- Distal vascular anomalies
Features (depend on level within canal):
- If superficial + deep branches compressed: motor + sensory loss confined to palmar surface of ulnar 1½ digits only (dorsal hand sensation SPARED)
- If only deep motor branch: purely motor — interossei and hypothenar weakness, NO sensory loss
- Distal compression at pisohamate hiatus: selective deep branch — hypothenar muscles relatively spared, interossei weak
- More pronounced claw (see ulnar paradox)
7. The Ulnar Paradox
Ulnar Paradox: A lesion of the ulnar nerve at the wrist produces a more severe claw deformity than a lesion at the elbow — even though the elbow lesion is at a higher level and causes more functional loss.
Explanation:
Clawing results from:
- Loss of lumbrical function → loss of MCP flexion
- Unopposed long flexors (FDP) → IP joint flexion
- Unopposed extensors → MCP hyperextension
At the elbow, the nerve is cut proximal to the FDP branches. So FDP to ring and little fingers is also paralysed. With both FDP and the lumbricals non-functional, the FDP cannot contribute to IP flexion — so clawing is less visible (the fingers lie relatively flat).
At the wrist, the nerve is cut distal to the FDP branches. The FDP is intact and actively flexes the IP joints, while lumbricals are still paralysed. Unopposed FDP action + MCP hyperextension from extensor dominance = more pronounced claw.
Simple rule: The more distal the lesion, the worse the claw — this is the paradox.
— Gray's Anatomy for Students, p. 936-937; Bradley and Daroff's Neurology in Clinical Practice
8. Important Clinical Signs
| Sign | Test | Interpretation |
|---|---|---|
| Froment's sign | Ask patient to hold paper between thumb & index finger | Thumb IP flexes (FPL compensates for weak adductor pollicis) |
| Wartenberg's sign | Little finger abducted at rest | Weak 3rd palmar interosseous |
| Tinel's sign | Percussion over cubital tunnel/Guyon's | Tingling in ulnar distribution |
| Elbow flexion compression test | Sustained elbow flexion + pressure on nerve | Reproduces symptoms |
| Card test | Hold card between fingers | Weak interossei |
9. Investigations
Electrodiagnostic (EDX) studies — mainstay:
- Nerve conduction study (NCS):
- Focal slowing of motor conduction velocity (>10–15 m/sec) across the elbow
- Conduction block (reduction in CMAP amplitude/area >20–30%) across elbow
- Elbow segment should be studied with elbow flexed 70–90° (reduces measurement error)
- Additional recording from 1st dorsal interosseous (in addition to abductor digiti minimi) increases yield
- Ulnar SNAP — abnormal in wrist lesions affecting sensory fibers; can be normal in purely motor wrist lesions
- EMG (needle):
- Denervation in FCU, FDP (4th/5th) — indicates elbow or higher lesion
- Denervation confined to hand muscles — indicates wrist lesion
- Spare dorsal cutaneous territory on EMG = wrist lesion
- Neuromuscular ultrasound:
- Identifies nerve thickening, subluxation, structural lesions (ganglion, lipoma)
- Nerve cross-sectional area >10 mm² suggests entrapment
- MRI:
- Identifies ganglia, soft tissue masses, post-traumatic changes
- Plain radiograph:
- Assess for fractures (pisiform, hook of hamate, medial epicondyle), cubitus valgus, osteophytes
10. Treatment
Conservative
- Avoid provocative positions (prolonged elbow flexion, pressure on elbow/wrist)
- Elbow extension splint at night (cubital tunnel)
- NSAIDs for pain
- Occupational therapy / nerve gliding exercises
- Remove offending cause (bicycle handlebars, hand tools)
Surgical (when conservative fails or severe/progressive deficit)
For elbow entrapment:
- In situ decompression (ulnar neurolysis) — division of the humeral-ulnar aponeurosis; lower complication rate
- Medial epicondylectomy
- Anterior transposition (subcutaneous, intramuscular, or submuscular) — higher complication rate but preferred when subluxation is present
- Best outcomes if symptoms < 1 year; ~60% benefit from surgery
- Patients with significant conduction block (>50%) have more favourable prognosis
For wrist (Guyon's canal):
- Surgical decompression and exploration
- Ganglion excision if present
- Fracture fixation if applicable
- Prognosis generally good after surgical decompression
Key References:
- Gray's Anatomy for Students, pp. 881, 905, 936–937
- Bradley and Daroff's Neurology in Clinical Practice, pp. 2638–2641
- General Anatomy and Musculoskeletal System (THIEME Atlas), p. 392
This is a shared conversation. Sign in to Orris to start your own chat.