Cyberknife surgery full details for md exams 10 marks answer
Reading File
Finding Sources
Searching the Web
CyberKnife radiosurgery complete details mechanism principles clinical applications MD exam
Searching PubMed
CyberKnife stereotactic radiosurgery clinical applications
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the comprehensive MD exam answer on CyberKnife surgery:
CyberKnife Stereotactic Radiosurgery - 10 Marks Answer
Definition
CyberKnife is a frameless robotic radiosurgery system (manufactured by Accuray, Sunnyvale, CA) that delivers precisely targeted, high-dose radiation to tumors anywhere in the body - both intracranial and extracranial. The term "surgery" is a misnomer; it involves no incision and is a non-invasive radiation technique. It is classified as a form of Stereotactic Body Radiation Therapy (SBRT) or Stereotactic Radiosurgery (SRS).
Historical Background
- The concept of stereotactic irradiation was introduced in 1951 by Lars Leksell, who coupled a stereotactic device to an orthovoltage x-ray tube to treat trigeminal neuralgia.
- Leksell subsequently developed the Gamma Knife (1968) using 60Co sources.
- The CyberKnife system was developed as the next evolution - replacing frame-based localization with robotic, image-guided, frameless delivery.
- Accuracy of the first-generation CyberKnife (Murphy and Cox, 1996): ~1.6 mm - comparable to frame-based systems. Modern systems achieve ~1.1 mm accuracy.
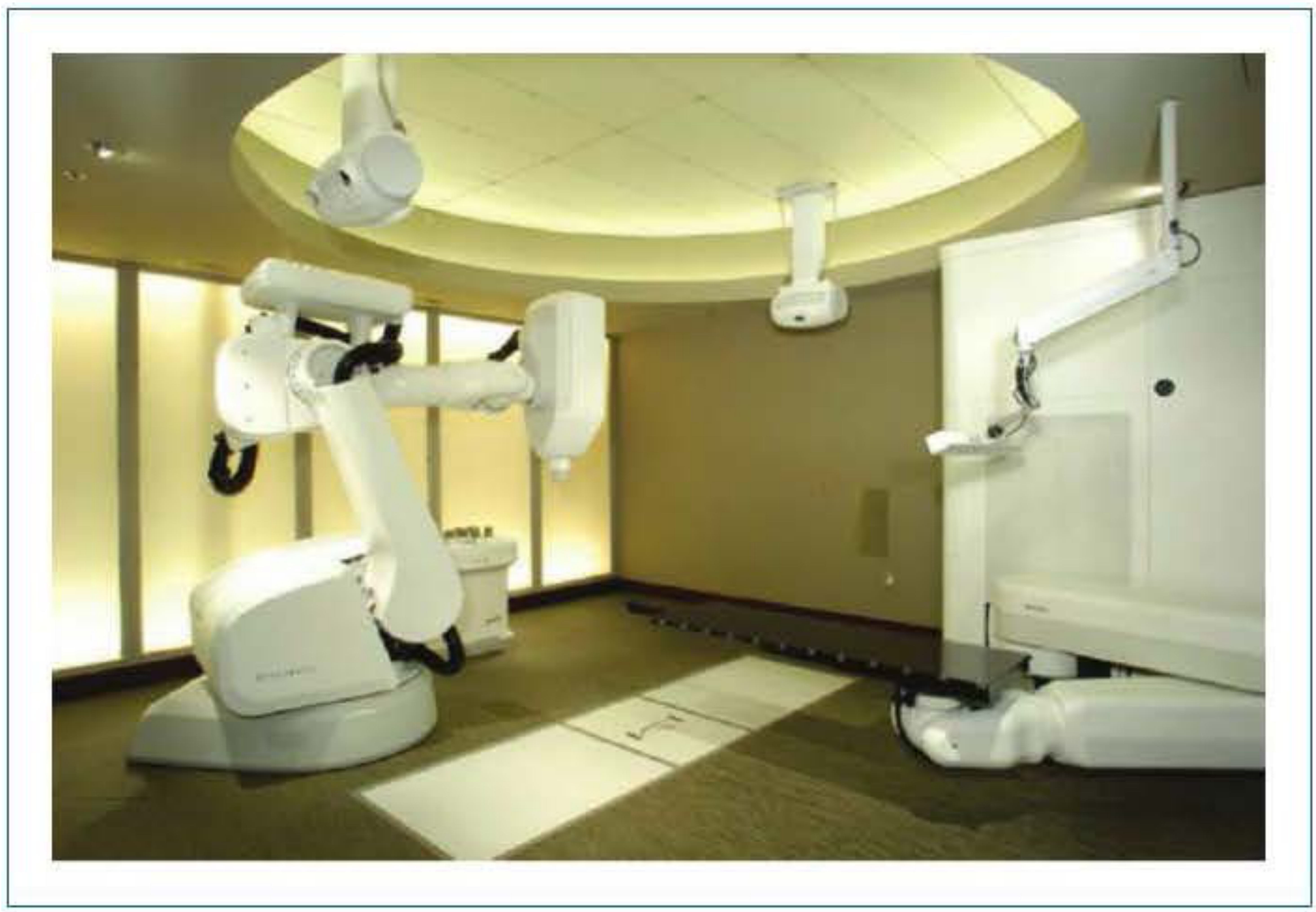
Components of the CyberKnife System
The system consists of three integrated components:
| Component | Details |
|---|---|
| Compact 6-MeV LINAC | X-band linear accelerator (compact design for mobility), delivers pencil beams of megavoltage radiation |
| Computer-controlled Robotic Arm | 6 degrees of freedom; can position the LINAC at >100 nodes, each with 12 possible approach angles = >1,200 beam positions |
| Real-time Image Guidance System | Orthogonal kV x-ray sources mounted to ceiling; amorphous silicon detectors capture live radiographs during treatment |
Principle of Operation
1. Radiation Source
Unlike the Gamma Knife (which uses 179-201 fixed ^60Co sources), the CyberKnife uses a single LINAC mounted on a robotic arm that delivers radiation from hundreds of potential angles sequentially. This creates the same effect - convergence of multiple beams at a focal target - but with far greater flexibility.
2. Frameless Localization
The CyberKnife does not require a stereotactic head frame. Instead:
- Uses the skeletal structure of the body as a reference frame
- Co-registers digitally reconstructed radiographs (DRRs) generated from pre-treatment CT scans with live x-ray projections captured during treatment
- This allows scanning, planning, and QA to happen at any time before treatment
3. Real-Time Tracking
- Orthogonal kV x-ray images are acquired before and during treatment
- The operating system correlates live radiographs with preoperative CT to determine patient/tumor position repeatedly throughout treatment
- The robot compensates for patient movement by repositioning the LINAC - total time from imaging to robot compensation: ~7-10 seconds
- Using this tracking, CyberKnife can also adjust for respiratory motion (synchrony tracking), enabling treatment of lung and liver lesions
Treatment Planning
Imaging
- CT-based (unlike most Gamma Knife procedures which are MRI-based)
- MRI can be fused with CT for optimal soft tissue + skeletal anatomy information
- CT angiography used for vascular lesions (AVMs, glomus tumors)
Planning Options
- Forward planning - radiation oncologist specifies dose from each targeting position; software calculates total dose
- Inverse planning - oncologist specifies total tumor dose and critical structure boundaries; software determines targeting positions and beam weights
- Nonisocentric delivery - beams originate from arbitrary points, creating asymmetric irradiation that conforms to irregular tumor shapes (advantage over Gamma Knife)
- Isocentric/multi-isocentric delivery - spherical dose distributions; better for spherical tumors
Dose Fractionation Options
- Single fraction (radiosurgery): 8-24 Gy in one session
- Hypofractionation: 2-5 sessions (typical for larger or critical structure-adjacent tumors)
- Conventional fractionation: traditional fractionated regimen also possible (unlike Gamma Knife, where rigid frame fixation prevents fractionation)
- Each session: 30-90 minutes; total course: 1-5 days vs. 30-35 sessions in conventional RT
Dose Distribution Advantage
- Nonisocentric plans allow beams from arbitrary directions to concentrate within irregular lesions
- Creates asymmetric irradiation - avoids critical structures while ensuring complete coverage
- Results in a rapid dose fall-off outside the target - sparing surrounding healthy tissue
- Sub-millimeter precision with accuracy on the order of ±1.1 mm
Key Advantages Over Other Systems
| Feature | CyberKnife | Gamma Knife | Conventional LINAC-SRS |
|---|---|---|---|
| Frame required | No (frameless) | Yes (rigid frame) | Usually yes |
| Fractionation | Yes | No | Limited |
| Extracranial treatment | Yes | No | Limited |
| Real-time motion tracking | Yes | No | No |
| Degrees of freedom | 6 | Fixed | Limited |
| Accuracy | ~1.1 mm | ~1.2-1.3 mm | ~2 mm |
| Treatment positions | >1,200 | Fixed | Limited arcs |
Clinical Indications
Intracranial
- Brain tumors: Primary and metastatic (glioma, meningioma, acoustic neuroma / vestibular schwannoma)
- Arteriovenous malformations (AVMs)
- Trigeminal neuralgia
- Pituitary adenoma
- Skull base tumors: Lower posterior fossa, foramen magnum (unreachable by Gamma Knife)
Extracranial (unique to CyberKnife)
- Spine and spinal cord tumors (spinal cord cannot be treated with Gamma Knife)
- Lung cancer (with synchrony tracking for respiratory motion)
- Prostate cancer (5-session treatment possible instead of weeks)
- Liver tumors / hepatocellular carcinoma
- Pancreatic cancer (fiducial markers placed by EUS guidance)
- Kidney (renal cell carcinoma)
- Gynecologic tumors
Special Advantage - Multiple Simultaneous Targets
CyberKnife can treat multiple tumors at different locations during a single session (e.g., skull base + neck nodal disease simultaneously).
Contraindications / Limitations
- Large tumor size (>3-4 cm diameter is relative contraindication for single fraction)
- Tumors diffusely infiltrating around critical structures (e.g., brainstem)
- Poor patient compliance (patient must remain still, though motion is compensated)
- Pregnancy
- Previous radiation to the same field may limit total deliverable dose
Comparison with Gamma Knife (High-Yield Exam Table)
| Parameter | CyberKnife | Gamma Knife |
|---|---|---|
| Source | Single LINAC on robotic arm | 179-201 fixed ^60Co sources |
| Manufacturer | Accuray Inc. | Elekta |
| Frame | Frameless | Rigid stereotactic frame |
| Fractionation | Possible | Not possible |
| Treatment sites | Whole body (intra + extracranial) | Intracranial only |
| Motion compensation | Real-time (synchrony system) | None |
| Collimator helmets | Variable collimators | Fixed helmet sizes (4,8,14,18 mm) |
| Radiobiology | SBRT/SRS | Single-fraction SRS |
Radiobiological Basis
The rationale for high-dose-per-fraction delivery (hypofractionation/radiosurgery) rests on the linear-quadratic model. At higher doses per fraction:
- Greater double-strand DNA breaks occur that exceed repair capacity
- Tumors with low alpha/beta ratios (e.g., prostate, melanoma, sarcoma) are particularly sensitive to high-dose fractions
- The ablative dose destroys not just tumor cells but also damages tumor vasculature
- Fractionation allows healthy tissue to repair between sessions while maintaining tumoricidal effect
Complications / Side Effects
- Acute: Fatigue, skin erythema at beam entry points (minimal due to distributed beams), headache
- Brain tumors: Radiation necrosis (~2-5%), cerebral edema (managed with dexamethasone), radionecrosis
- Acoustic neuroma: Facial nerve dysfunction, hearing loss, vestibular paresis (stabilizes by 6-18 months)
- Spine: Radiation myelopathy (rare, dose-dependent)
- Lung: Radiation pneumonitis
- Optic apparatus: Risk of optic neuropathy <2% if maximum dose to chiasm/optic nerves is kept <8 Gy in single fraction
Summary - High-Yield Points for MD Exam
- CyberKnife = compact 6-MeV LINAC + 6-DOF robotic arm + real-time image guidance
- Frameless stereotactic radiosurgery - no rigid head frame required
- Accuracy: ~1.1 mm (comparable to frame-based systems)
- Can treat >1,200 beam positions (>100 nodes × 12 angles)
- Unique ability to treat extracranial sites and compensate for breathing motion
- Fractionation is possible (unlike Gamma Knife)
- CT-based planning with MRI fusion; EUS-guided fiducials for pancreatic tumors
- Sessions: 1-5 days (vs. 30-35 sessions conventional RT)
- Per-session duration: 30-90 minutes
- Treatment of multiple simultaneous tumor sites in one session is possible
Sources: Shambaugh Surgery of the Ear; Cummings Otolaryngology Head and Neck Surgery; Schwartz's Principles of Surgery, 11th Ed.; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.