Write a notes on neuromuscular monitoring
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from Miller's Anesthesia and Barash's Clinical Anesthesia. Let me compile the notes.
Neuromuscular Monitoring
1. Introduction and Clinical Significance
Neuromuscular monitoring is the assessment of the degree of neuromuscular blockade (NMB) produced by neuromuscular blocking drugs (NMBDs) and the adequacy of its reversal. Its primary clinical purpose is to prevent residual neuromuscular block — incomplete recovery of muscle function at extubation.
- Residual paralysis occurs in 30–40% of patients reversed with neostigmine, and up to 5% even with sugammadex
- With over 230 million surgical procedures annually worldwide, the cumulative impact is substantial
- Neither elapsed time since the last NMBD dose nor clinical tests (head lift, grip strength, tidal volume) are reliable indicators of full recovery — guidelines now mandate quantitative neuromuscular monitoring
"Because of the highly significant interpatient variability and unpredictability of responses to NMBD administration, quantitative neuromuscular monitoring is required." — Miller's Anesthesia, 10e
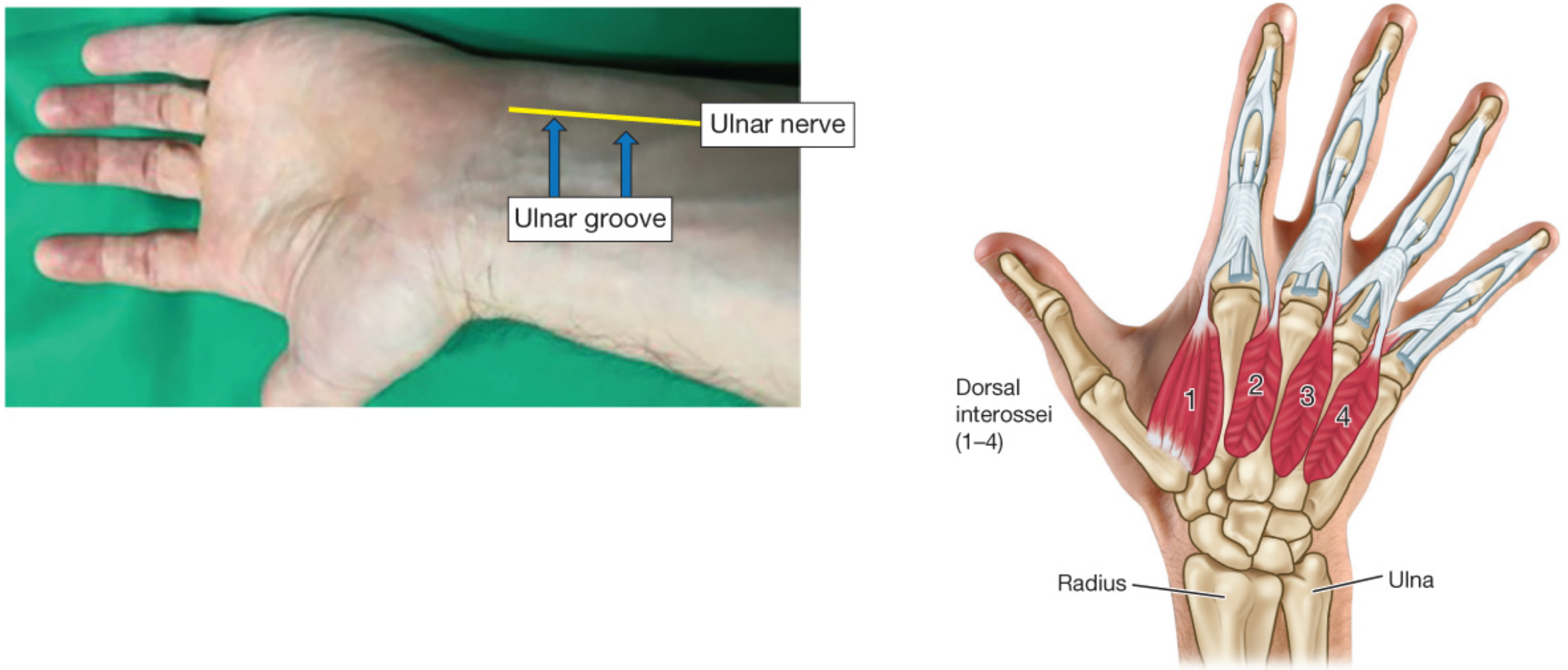
2. Sites of Stimulation
The ulnar nerve at the wrist is the most common monitoring site, with thumb adduction (adductor pollicis) as the measured response.
- Negative (black) stimulating electrode → distal
- Positive (red) electrode → proximal ("red toward the head")
- Other sites: facial nerve (orbicularis oculi), posterior tibial nerve, peroneal nerve
The adductor pollicis is the reference muscle for clinical NMB assessment. Different muscles recover at different rates — the diaphragm and laryngeal muscles are more resistant to block and recover faster than the adductor pollicis.
3. Stimulation Patterns
Single-Twitch Stimulation
- A single supramaximal stimulus (0.1–1 Hz)
- Compares response to a baseline pre-block value
- Requires a baseline measurement before NMBD administration
- Detects moderate to profound block, but not subtle residual paralysis
Train-of-Four (TOF)
- Four supramaximal stimuli at 2 Hz (over 2 seconds)
- The TOF ratio = T4/T1 amplitude (T4 divided by T1)
- Most clinically useful pattern
- Does not require a pre-block baseline
| TOF Ratio | Clinical Significance |
|---|---|
| < 0.4 | Moderate to severe residual block |
| 0.4–0.7 | Clinically detectable weakness; unable to sustain head lift |
| 0.7–0.9 | Subtle weakness; head lift possible but pharyngeal dysfunction present |
| ≥ 0.9 | Recovery threshold; considered adequate for extubation |
| 1.0 | Full recovery |
The 5-second head lift can be accomplished despite a TOF ratio ≤ 0.5 in most patients — it is an unreliable test.
Tetanic Stimulation
- High-frequency stimulation (50 or 100 Hz for 5 seconds)
- Fade during tetanus indicates residual non-depolarizing block
- Post-tetanic facilitation: enhanced response after tetanus (useful for assessing deep block)
- Painful in awake patients; used intraoperatively
Post-Tetanic Count (PTC)
- Used during deep/intense block when TOF count = 0
- 50 Hz tetanus for 5 seconds → 3-second pause → single twitches at 1 Hz
- PTC 1–2 = very deep block; PTC ≥ 10 = moderate block approaching TOF count 1
Double-Burst Stimulation (DBS)
- Two short tetanic bursts (50 Hz, 3 impulses each) separated by 750 ms
- More sensitive than TOF for detecting residual fade subjectively
- Better for tactile assessment of fade than TOF, but still inferior to quantitative monitoring
4. Depths of Neuromuscular Block
| Level | Definition | Receptor Occupancy | Quantitative Finding |
|---|---|---|---|
| Complete | No response to any stimulation | >95% | TOFC 0, PTC 0 |
| Deep | Posttetanic response only | 90–95% | TOFC 0, PTC ≥ 1 |
| Moderate | TOF count 1–3 | 70–90% | TOFC 1–3 |
| Shallow | TOF count 4, ratio < 0.4 | ~60–70% | TOFC 4, TOF ratio < 0.4 |
| Minimal | TOF count 4, ratio 0.4–0.9 | ~60–70% | TOFC 4, TOF ratio 0.4–0.9 |
| Recovered | Full recovery | <70% | TOFC 4, TOF ratio ≥ 0.9 |
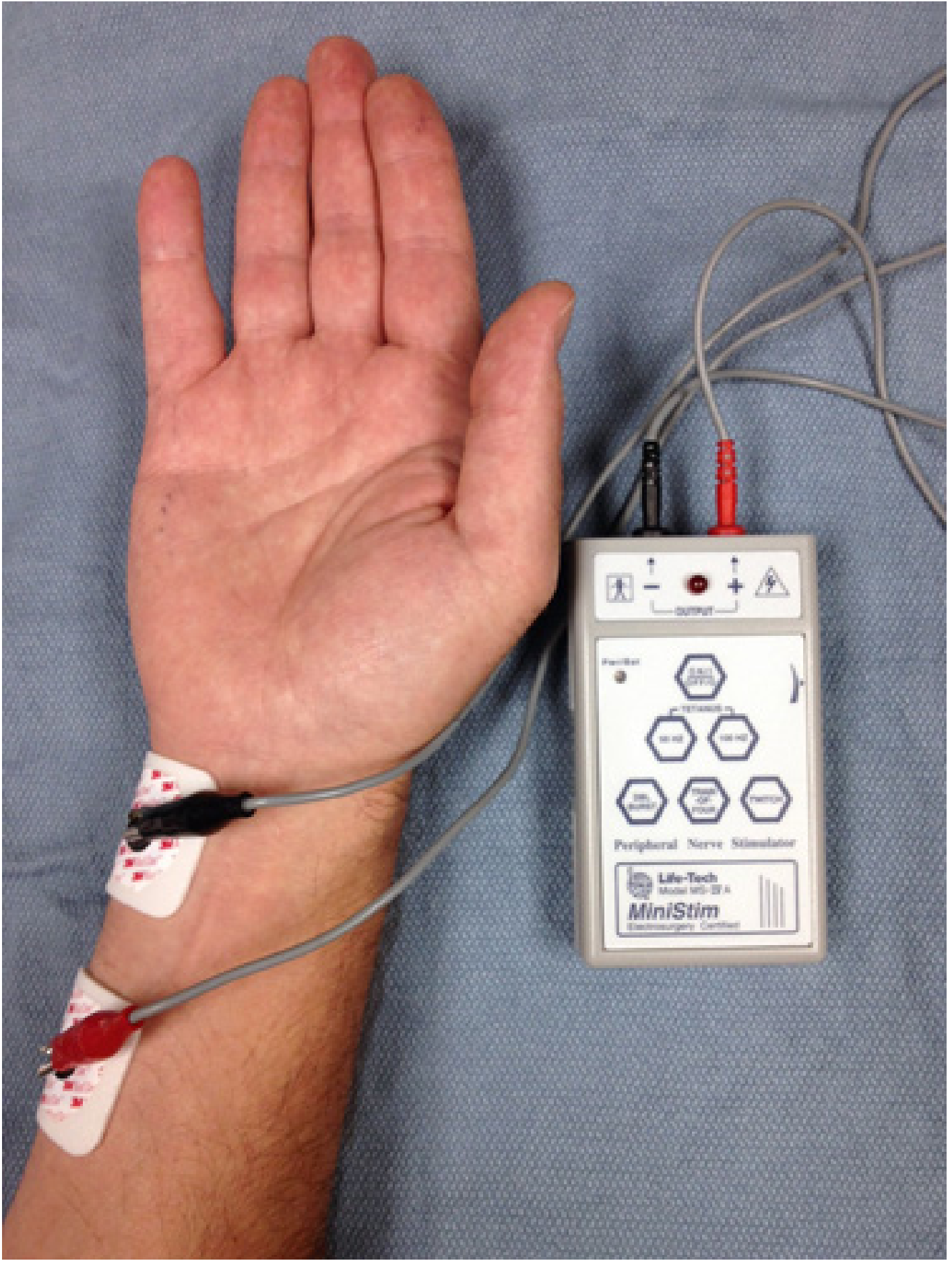
5. Monitoring Methods
Qualitative (Subjective) Monitoring — Peripheral Nerve Stimulator (PNS)
- Battery-operated devices delivering square-wave current (10–80 mA, 100–300 µs duration)
- Response assessed visually or tactilely (feeling thumb movement)
- Major limitation: clinicians cannot detect fade when TOF ratios exceed 0.30–0.40
- Cannot reliably confirm full neuromuscular recovery — therefore insufficient as the sole monitoring tool
Quantitative (Objective) Monitoring — Gold Standard
Three main technologies:
a) Mechanomyography (MMG)
- Reference standard (gold standard) for research
- Measures isometric force of thumb adduction using a force transducer
- Requires the hand to be fixed; impractical for routine clinical use
- TOF ratio bias is minimal (~2%)
b) Electromyography (EMG)
- Records the compound muscle action potential (CMAP) after nerve stimulation
- Does not require thumb movement; suitable when the hand is inaccessible
- EMG values correlate closely with MMG (bias ≈ −4.7% to slightly higher than MMG)
- Examples: NMT module on Datex-Ohmeda monitors
c) Acceleromyography (AMG)
- Measures acceleration of thumb movement (Newton's 2nd law: force = mass × acceleration)
- Most widely available quantitative monitor in clinical practice
- Requires free thumb movement (unconstrained hand)
- TOF ratio may be overestimated by ~5–10% compared to MMG → recommended cutoff is TOF ratio ≥ 1.0 (not 0.9) when using AMG
- Examples: TOF-Watch SX
d) Kinemography (KMG)
- Measures thumb movement using a sensor strip/flexible sensor
- Similar bias to AMG; values slightly higher than MMG
Summary of Bias vs. MMG Reference:
| Technology | Measured Bias | Equivalent Safe Goal |
|---|---|---|
| MMG | ~2% | TOF ≥ 0.92 |
| EMG | −4.7% | TOF ≥ 0.85 |
| AMG | +5 to +10% | TOF ≥ 0.95–1.0 |
| TOFcuff | +4.7% | TOF ≥ 0.95 |
6. Residual Neuromuscular Block
Definition: TOF ratio < 0.90 (by normalized AMG or EMG) with or without clinical signs (dysphagia, diplopia, general weakness, inability to speak).
Clinical consequences at TOF ratio < 0.90:
- Impaired pharyngeal function and upper airway obstruction
- Increased risk of pulmonary aspiration
- Impaired hypoxic ventilatory control
- Prolonged PACU stay and adverse respiratory events
Incidence: In a large cohort receiving a single intubating dose of intermediate-duration NMBD, 37% had a TOF ratio < 0.90 when tested ≥ 2 hours later. Even 4 hours after a single dose of vecuronium, 8.4% of patients had TOF ratios < 0.80.
7. Clinical Decision-Making Based on Monitoring
| Clinical Scenario | Monitoring Finding | Recommended Action |
|---|---|---|
| Assessing adequate reversal | TOF ratio ≥ 0.9 (quantitative) | Extubation safe |
| Guide neostigmine dosing | TOF count = 4 with no fade | Low-dose neostigmine (20 µg/kg) may be used |
| Guide sugammadex dosing | Deep block (PTC ≥ 1) | Sugammadex 4 mg/kg |
| Guide sugammadex dosing | Moderate block (TOFC 1–3) | Sugammadex 2 mg/kg |
| Intraoperative intense block | TOFC = 0, PTC = 0 | Complete block; no reversal yet |
- Neostigmine is most effective for antagonism of minimal block (TOFC 4, TOF ratio approaching 0.9)
- Quantitative monitoring is the only method to confirm TOF ratio ≥ 0.9 and safely avoid reversal or guide dosing
8. Factors Affecting Neuromuscular Recovery
- Drug choice: Intermediate-acting (vecuronium, rocuronium, cisatracurium, atracurium) are preferred over long-acting
- Cholinesterase deficiency: Prolongs effect of succinylcholine and mivacurium (both hydrolyzed by plasma cholinesterase); homozygous atypical gene may cause block lasting 4–8 hours after mivacurium
- Temperature: Hypothermia prolongs block duration
- Drug interactions: Volatile anesthetics potentiate NMBDs; aminoglycosides and other drugs may prolong block
- Age and hepatic/renal function: Affect pharmacokinetics
9. Guidelines and Current Recommendations
International guidelines from Canada, France, Spain, Australia, New Zealand, Czech Republic, Portugal, Japan, and the United States now recommend:
- Quantitative neuromuscular monitoring should be used to guide perioperative dosing of NMBDs and their antagonists
- Subjective assessment alone (PNS + visual/tactile) is insufficient to confirm full recovery
- Extubation should only occur when TOF ratio ≥ 0.9 is confirmed by quantitative monitoring
- Time-based decisions (waiting "long enough") are not acceptable clinical practice given extreme interpatient variability
Sources: Miller's Anesthesia, 2-Volume Set, 10e | Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
This is a shared conversation. Sign in to Orris to start your own chat.