Sjogren syndrome
Reading File
Finding Sources
Finding Sources
Searching Images
Sjogren syndrome histology salivary gland
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Sjögren syndrome based on authoritative textbook sources.
Sjögren Syndrome
Definition & Overview
Sjögren syndrome (SS) is a chronic systemic autoimmune disorder primarily targeting the exocrine glands — most notably the salivary and lacrimal glands. It is characterized by a dense lymphoplasmacytic infiltration leading to glandular hypofunction, with the hallmark symptoms of dry mouth (xerostomia) and dry eyes (keratoconjunctivitis sicca).
- Primary SS: disease confined to the exocrine glands
- Secondary SS: characteristic SS features occurring alongside another autoimmune disease (rheumatoid arthritis, SLE, scleroderma, polymyositis, primary biliary cirrhosis)
— Cummings Otolaryngology Head and Neck Surgery; Textbook of Family Medicine 9e
Epidemiology
- Estimated prevalence: 1–3% of the population
- Predominantly affects women (>90% of patients)
- Peak incidence: 4th–5th decade of life
Pathogenesis
The etiology involves a complex interplay of genetic, immune, and environmental factors:
- Genetic predisposition: HLA alleles B8 and DR3 increase susceptibility
- Environmental trigger: likely a viral infection that initiates an aberrant autoimmune response
- B-cell overstimulation: leads to excess immunoglobulins, autoantibody production, and formation of germinal centers within glandular tissue — autoreactive B-cell clones escape tolerance checkpoints
- Elevated follicular helper T-cells also contribute to disease progression
Key autoantibodies:
- Anti-Ro (SS-A) and Anti-La (SS-B) — ribonuclear proteins; used to support diagnosis
- Elevated RF (>1:320) and ANA (>1:320) also seen
— Cummings Otolaryngology
Clinical Features
Oral (Xerostomia)
- Difficulty chewing, swallowing, and speaking
- Multiple dental caries
- Food adherence to buccal mucosa
- Intolerance to acidic/spicy foods
- Smooth, fissured tongue with atrophic filiform papillae
- Oral Candida albicans overgrowth (common)
- Scant or cloudy saliva from ducts
- Bilateral parotid gland enlargement in 25–66% of patients (may be episodic or chronic)
Ocular (Keratoconjunctivitis Sicca)
- "Gritty" or "sandy" foreign body sensation
- Bulbar conjunctival vessel dilation, perilimbal injection
- Irregular corneal image
- Lacrimal gland enlargement (occasionally)
Systemic
- Fatigue, dry skin, vaginal dryness
- Upper respiratory tract dryness
- Dysphagia (from reduced saliva)
- Constitutional symptoms
Diagnosis
San Diego Criteria (Fox & Saito)
| Criterion | Details |
|---|---|
| IA | Objective ocular dryness: Schirmer test <8 mm/5 min + positive Rose Bengal staining |
| IB | Objective dry mouth: decreased parotid flow + minor salivary gland biopsy with focus score ≥1 |
| IC | Serologic evidence: elevated RF/ANA or positive anti-SS-A/SS-B |
| Definite SS | All three criteria (IA + IB + IC) |
| Probable SS | IA + IB-1 + IC (biopsy not required) |
Exclusions: HIV, sarcoidosis, pre-existing lymphoma, hepatitis B or C, primary fibromyalgia, keratitis sicca from other causes
Key Diagnostic Tests
- Schirmer test: tear flow measurement (<8 mm/5 min = abnormal)
- Rose Bengal staining: identifies corneal/conjunctival epithelial damage
- Minor salivary gland biopsy: definitive; shows focal lymphocytic infiltration (focus score ≥1)
- Sialography: demonstrates sialectasis in 85–97% of patients
- Lashley cups: quantify parotid flow rate
— Textbook of Family Medicine 9e
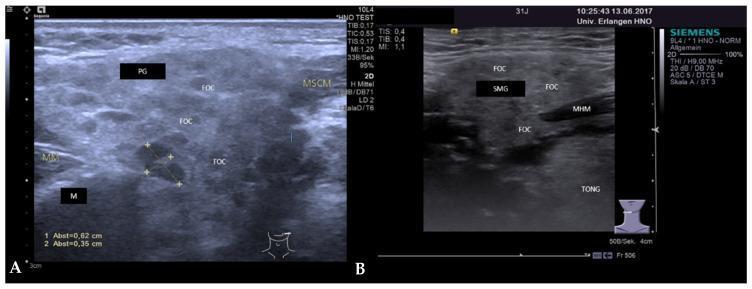
Imaging
Salivary gland ultrasound in early SS shows enlarged glands with multiple small (~2–3 mm) hypoechoic foci throughout the parenchyma, representing focal lymphocytic accumulations:
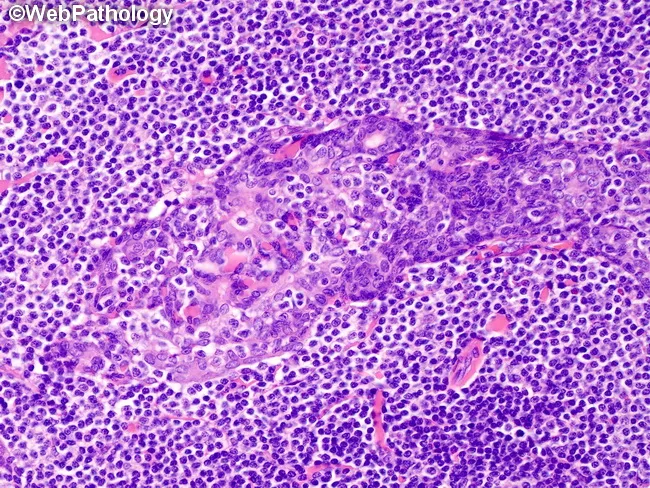
Histopathology
Minor salivary gland biopsy shows dense lymphocytic infiltrates destroying acinar epithelium. In advanced cases, lymphoepithelial lesions develop — a hallmark of SS — where lymphoid cells infiltrate and distort ductal epithelium:
Complications
- MALT lymphoma (extranodal marginal zone B-cell lymphoma): most feared complication; arises in salivary glands from autoreactive B-cell clones that escape tolerance. Risk is significantly elevated in SS patients. Histology shows CD20+, CD79a+, BCL2+, CD5−, Cyclin D1− lymphoid infiltrate with lymphoepithelial lesions.
- Renal involvement: tubulointerstitial nephritis, distal RTA (covered in nephrology texts)
- Neurologic involvement: peripheral and cranial neuropathies
- Hepatic involvement: overlap with primary biliary cirrhosis
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Sarcoidosis | Non-caseating granulomas, hilar adenopathy |
| HIV/AIDS | HIV serology positive |
| Lymphoma | Clonal B-cell expansion, no autoantibodies |
| Hepatitis C | HCV serology, hepatic involvement |
| IgG4-related disease | Elevated IgG4, storiform fibrosis on biopsy |
Management (Overview)
- Oral dryness: salivary substitutes, sugar-free lozenges, pilocarpine (muscarinic agonist), meticulous dental hygiene, antifungals for candidiasis
- Ocular dryness: artificial tears, cyclosporine eye drops, moisture chambers
- Systemic/severe disease: hydroxychloroquine, corticosteroids, rituximab (for severe systemic features or lymphoma)
- MALT lymphoma: radiotherapy (early stage) or rituximab-based regimens
— Cummings Otolaryngology; Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.