Provide details info about nexa cochlear and comparison in brief and details
Reading File
Finding Sources
Searching Images
NEXA cochlear implant components design
Finding Sources
Searching Images
cochlear implant brands comparison MED-EL Cochlear Advanced Bionics
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of cochlear implants, with a dedicated focus on the NEXA (Cochlear Ltd.) system and comparisons with the other major manufacturers.
Cochlear Implants — Detailed Overview
What Is a Cochlear Implant?
A cochlear implant (CI) is a surgically implanted neuroprosthetic device that bypasses damaged hair cells and directly stimulates the spiral ganglion cells / auditory nerve to restore hearing in patients with severe-to-profound sensorineural hearing loss (SNHL). Even when all hair cells are destroyed, if the auditory nerve is intact, a CI can restore substantial hearing.
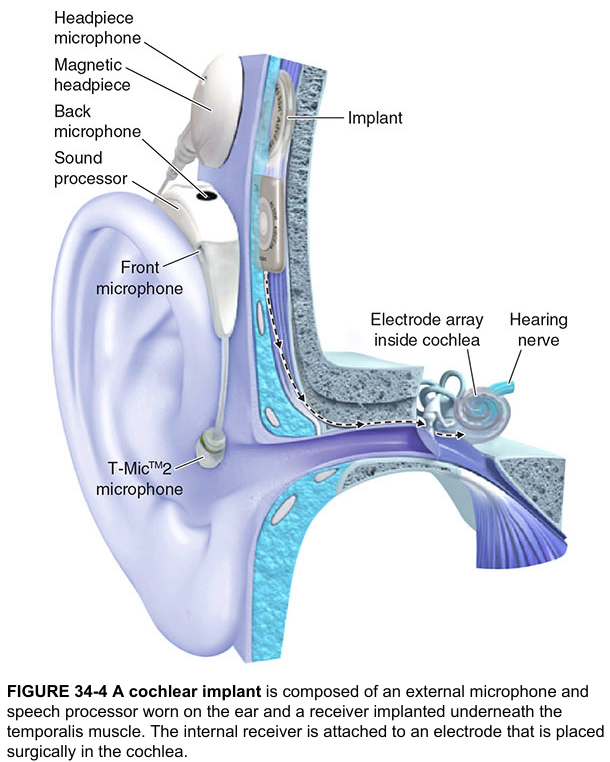
System Components (Universal to All CI Brands)
External Components
| Component | Function |
|---|---|
| Microphone | Captures acoustic signals from the environment |
| Sound Processor | Amplifies, compresses, filters, and digitizes the signal via Fourier analysis; encodes timing, frequency, and intensity |
| RF Transmitter Antenna | Sends the processed signal transcutaneously to the internal device |
| External Magnet | Aligns with the internal magnet to facilitate signal transmission |
| Battery | Powers all external components |
Internal Components
| Component | Function |
|---|---|
| Internal Magnet | Aligns with external magnet |
| Internal RF Antenna | Receives the transcutaneous signal |
| Receiver/Stimulator | Decodes signal into electrical impulses sent to the electrode array |
| Electrode Array | Placed in the scala tympani; stimulates spiral ganglion cells along the tonotopic axis |
The most common signal processing strategy is Continuous Interleaved Sampling (CIS), which presents non-simultaneous rapid impulses across the array to minimize channel interaction and better represent the tonotopic organization of the cochlea.
— K.J. Lee's Essential Otolaryngology, p. 407–408
The Three Major FDA-Approved CI Manufacturers
There are three manufacturers with devices used in the United States: Cochlear Americas, Advanced Bionics Corporation, and MED-EL. The NEXA is the latest flagship processor from Cochlear Americas.
NEXA (Cochlear Americas) — Detailed Profile
The Nucleus NEXA is the most recent sound processor from Cochlear Americas, pairing with the Nucleus implant family (CI512, CI522, CI532, CI624, CI622). Key features include:
Internal Device — Nucleus Profile / CI532 / CI624
- Titanium case with flexible silicone housing
- Only 3.9 mm thick at the receiver housing; 3.3 mm at the coil/magnet region — among the slimmest on the market
- Removable magnet (standard)
- MRI compatibility: up to 3.0 T with magnet removed; 1.5 T with magnet in place using the Cochlear Nucleus Implant Bandage and Splint Kit
Electrode Options (Nucleus Family)
| Electrode | Contacts | Distribution | Design |
|---|---|---|---|
| Slim Modiolar (CI532) | 22 half-banded | Over 15 mm | Perimodiolar, precurved; loaded in disposable sheath; reloadable if needed |
| Contour Advance | 22 half-banded | Over 15 mm (22 mm insertion) | Perimodiolar, uses stylet — NOT reloadable once stylet removed |
| Slim Straight | 22 half-banded | Over 20 mm | Lateral wall, straight |
| Hybrid (EAS) | 22 half-banded | Over 19.5 mm | For electroacoustic stimulation (residual low-frequency hearing) |
| Straight | 22 full-banded | Over 16.3 mm | Lateral wall |
| Split Array | 11 + 11 full-banded | 8.2 mm each | For severely ossified cochleas |
- All electrodes use 22 contacts — the highest count among the three manufacturers
- Perimodiolar design places electrodes close to the modiolus → closer to the spiral ganglion → theoretically lower power consumption and better selectivity
External Processor Features (NEXA / N7 / Kanso series)
- BTE (behind-the-ear) and off-the-ear single-unit (Kanso) options
- Multiple colors for aesthetic customization
- Waterproof cover option (Aqua+)
- Remote control and Bluetooth connectivity
- Designed specifically for children with smaller, lighter BTE variants
— Cummings Otolaryngology Head and Neck Surgery, p. 3075–3081
Comparison: NEXA (Cochlear) vs. Advanced Bionics vs. MED-EL
| Feature | Cochlear Nucleus / NEXA | Advanced Bionics HiRes Ultra | MED-EL SYNCHRONY |
|---|---|---|---|
| Electrode contacts | 22 | 16 | 12 |
| Primary electrode design | Slim Modiolar (perimodiolar) | HiFocus Mid-Scala / Helix / 1j | FLEX series (lateral wall to perimodiolar) |
| Electrode array length | 15–24 mm (varies by array) | 17–23 mm | 26.4 mm (longest — deepest apical coverage) |
| Electrode spacing | Variable, 0.3 mm width contacts | 1.1 mm spacing over 17 mm | 2.4 mm spacing (standard); 1.1 mm (compressed) |
| Implant thickness | 3.9 mm (thinnest) | Tapered-edge design | 4.5 mm at receiver |
| MRI approval | 1.5 T (magnet in) / 3.0 T (magnet out) | 1.5 T (magnet in) / 3.0 T (magnet out); HiRes Ultra 3D: no magnet removal or bandaging needed | 1.5 T (magnet in); SYNCHRONY: 1.5 T and 3.0 T with or without magnet (first to achieve this) |
| Magnet | Removable | Removable (Ultra 3D: fixed, MRI-safe) | Diametric rotating magnet — optionally removable |
| Reloadable electrode | Yes (CI532 Slim Modiolar); No (Contour Advance once stylet removed) | Yes — easily reloaded multiple times | Yes |
| Hearing preservation options | Hybrid/EAS array | Mid-Scala array | FLEX series (especially FLEX28, FLEX24) |
| Ossified cochlea options | Split array | HiFocus 1j | Compressed array (15 mm) + custom common cavity |
| Sound processor styles | BTE (N7/NEXA) + off-ear (Kanso) | BTE (Naida) + body-worn (Neptune, waterproof) | BTE (OPUS 2) + off-ear (RONDO 2 single unit) |
| Signal processing channels | 22 channels | 16 channels | 12 channels |
— Cummings Otolaryngology, pp. 3076–3079; K.J. Lee's Essential Otolaryngology, p. 408
Candidacy Criteria (All Devices)
| Population | Criteria |
|---|---|
| Adults (≥18 y) | Profound SNHL (PTA ≥ 70–90 dB); aided sentence recognition ≤50% in ear to be implanted, ≤60% contralateral |
| Children (2–17 y) | Moderate-to-profound SNHL (>40 dB); aided sentence recognition ≤50% |
| Infants (12–24 mo) | Severe-to-profound SNHL (>70 dB); aided word recognition ≤20–30% |
| Hybrid/EAS | Normal-to-moderate low-frequency hearing (≤500 Hz) + severe-to-profound mid/high-frequency loss |
Expanding indications now include single-sided deafness (SSD), asymmetric SNHL, and patients with more residual hearing than historically required.
— K.J. Lee's Essential Otolaryngology, p. 406; Cummings Otolaryngology, p. 3073
Key Clinical Points
- Bilateral implantation is now routinely recommended, offering head shadow effect, binaural summation, and improved speech-in-noise performance
- Electroacoustic stimulation (EAS/Hybrid): Combines residual acoustic low-frequency hearing with CI electric stimulation — superior performance in noise compared to either alone
- Duration of deafness is a key outcome predictor — longer deafness = poorer outcomes
- Cochlear ossification (e.g., post-meningitis) requires special electrode selection; CT and MRI are both used in pre-surgical planning
- Outcomes: >85% of implant recipients achieve open-set sentence recognition in quiet; speech-in-noise and music perception remain more challenging
Summary: Choosing Between Systems
- NEXA/Cochlear Nucleus: Most electrode contacts (22), thinnest implant, widest electrode variety, strong perimodiolar positioning — preferred when modiolar proximity matters
- Advanced Bionics HiRes Ultra 3D: Best MRI simplicity (no bandaging/magnet removal), easily reloadable electrode, good Mid-Scala positioning
- MED-EL SYNCHRONY: Deepest cochlear coverage (longest array), best MRI flexibility with SYNCHRONY (1.5 T and 3.0 T), widest range of array lengths for malformed/ossified cochleas, safest for patients needing frequent MRI
All three systems deliver equivalent speech perception outcomes in controlled trials — device selection is guided by surgical anatomy, MRI needs, patient lifestyle, electrode design preference, and surgeon familiarity.
Provide info about like viva or meeting question and answers pertaining to nucleus nexa
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive material. Let me compile this into a focused viva/meeting Q&A format specifically about the Nucleus NEXA.
Nucleus NEXA — Viva / Clinical Meeting Q&A
SECTION 1: BASICS & IDENTITY
Q1. What is the Nucleus NEXA?
The Nucleus NEXA is the latest-generation behind-the-ear (BTE) sound processor from Cochlear Americas, designed to pair with the Nucleus internal implant family (CI512, CI522, CI532, CI622, CI624). It is the successor to the N7 processor. It integrates Bluetooth wireless streaming, rechargeable batteries, and updated signal-processing capability within a slim BTE form factor.
Q2. Which internal devices is the NEXA compatible with?
The NEXA is backward compatible with the full Cochlear Nucleus implant family:
- CI512 (Nucleus Profile + Contour Advance)
- CI522 / CI532 (Nucleus Profile + Slim Modiolar)
- CI622 / CI624 (Nucleus Profile Plus)
- Also compatible with older CI24 series devices
This backward compatibility is a major clinical advantage — existing implant recipients can upgrade their external processor without further surgery.
Q3. What are the components of the Nucleus CI system?
External (NEXA Processor):
| Component | Role |
|---|---|
| Microphone | Captures environmental sound |
| Sound processor | Amplifies, filters, digitizes via Fourier analysis |
| RF transmitter coil | Sends signal transcutaneously to internal device |
| External magnet | Aligns with internal magnet |
| Battery (rechargeable) | Powers the system |
Internal (e.g., CI532):
| Component | Role |
|---|---|
| Receiver/stimulator | Decodes RF signal into electrical pulses |
| Loop antenna | Receives transcutaneous signal |
| Internal magnet (removable) | Alignment and MRI management |
| Electrode array | Stimulates spiral ganglion via scala tympani |
— Cummings Otolaryngology, p. 3075
SECTION 2: ELECTRODE TECHNOLOGY
Q4. How many electrodes does the Nucleus system have, and why does it matter?
The Nucleus system uses 22 electrode contacts — the highest among the three major manufacturers (Advanced Bionics = 16; MED-EL = 12). More contacts allow finer tonotopic mapping and more frequency channels, though research shows most users perceive fewer than 10 truly independent channels at any one time.
— K.J. Lee's Essential Otolaryngology, p. 408
Q5. What electrode arrays are available for the Nucleus system?
| Array | Contacts | Length | Design | Indication |
|---|---|---|---|---|
| Slim Modiolar (CI532) | 22 | 15 mm (insert 19 mm) | Perimodiolar, precurved, sheath-loaded | Standard; hearing preservation preferred |
| Contour Advance | 22 | 22 mm insertion | Perimodiolar, stylet-assisted | Standard ears |
| Slim Straight | 22 | 20 mm | Lateral wall, straight | Shorter cochlea, hearing preservation |
| Hybrid / EAS | 22 | 19.5 mm | Short, straight | Electroacoustic stimulation |
| Straight | 22 | 16.3 mm | Full-banded, lateral wall | Normal anatomy |
| Split Array | 11 + 11 | 8.2 mm each | Two arrays | Severely ossified cochlea |
Q6. What is the key difference between the Slim Modiolar and the Contour Advance electrodes?
The Slim Modiolar (CI532) is loaded in a disposable sheath that holds it straight during insertion; once deployed, it curves perimodiolarly. Crucially, it can be reloaded into the sheath if insertion difficulties arise. The Contour Advance uses a stylet to maintain its straight shape; once the stylet is removed, it cannot be reloaded — if the insertion fails, a backup device must be used. This is the single greatest disadvantage of the Contour Advance design.
— Cummings Otolaryngology, p. 3076
Q7. What is perimodiolar electrode positioning, and what is its advantage?
Perimodiolar positioning places the electrode array close to the modiolus (the central axis of the cochlea), in proximity to the spiral ganglion cells in Rosenthal's canal. The advantages are:
- Lower stimulation thresholds → lower power consumption
- Reduced channel interaction
- Better tonotopic selectivity
- Potentially improved speech perception
SECTION 3: MRI COMPATIBILITY
Q8. What are the MRI specifications for the Nucleus system?
- 3.0 T — approved with magnet removed, using the Cochlear Nucleus Implant Bandage and Splint Kit
- 1.5 T — approved with magnet in place, again using the bandage/splint kit
This requires head bandaging to immobilize the magnet and prevent rotation or discomfort inside the MRI bore. Magnet flipping within the silastic pocket has been reported but device integrity is not typically compromised.
Patients requiring frequent MRI (e.g., for neurological conditions) should be counselled about this limitation during device selection — the MED-EL SYNCHRONY offers the most MRI flexibility (1.5 T and 3.0 T with or without magnet removal).
— Cummings Otolaryngology, pp. 1951–1958
Q9. What happens if MRI is done without proper preparation in a Nucleus recipient?
The internal magnet within the RF coil area may experience torque and rotate or flip within its silastic pocket due to MRI magnetic field interactions. This generates discomfort, potential magnet extrusion, and image artifact around the temporal bone. While device electronic integrity is generally preserved, magnet displacement may require surgical correction.
SECTION 4: CANDIDACY
Q10. What are the FDA candidacy criteria for Nucleus cochlear implantation in adults?
- Severe-to-profound SNHL — PTA ≥ 70 dB HL (some criteria specify ≥ 90 dB)
- Appropriately fitted hearing aids with limited benefit
- Aided open-set sentence recognition ≤ 50% in the ear to be implanted; ≤ 60% contralateral or binaurally
- No central auditory lesion or absent auditory nerve
- No surgical contraindications
— Cummings Otolaryngology, p. 3073; K.J. Lee's Essential Otolaryngology, p. 406
Q11. What are the candidacy criteria for the Nucleus Hybrid (EAS) system?
The Hybrid system is for patients with:
- Normal to moderate low-frequency hearing (thresholds better than 60 dB HL at ≤ 500 Hz) in the ear to be implanted
- Severe-to-profound mid-to-high-frequency SNHL (PTA at 2, 3, 4 kHz ≥ 75 dB HL)
- Aided CNC word recognition 10%–60% in the ear to be implanted
- Contralateral ear: equal to or better than the implant ear, but ≤ 80% correct
— K.J. Lee's Essential Otolaryngology, p. 406
Q12. What are the expanding / off-label indications for cochlear implantation?
- Single-sided deafness (SSD)
- Asymmetric SNHL — one ear above the standard threshold
- Children < 12 months of age
- Patients with retrocochlear hearing loss (selected cases)
- Adults with moderate residual hearing (progressively relaxed criteria)
Candidacy has expanded markedly since the 1980s, when only total or near-total SNHL (PTA ≥ 100 dB) qualified.
SECTION 5: PROGRAMMING & MAPPING
Q13. What is a cochlear implant MAP, and how is it created for a Nucleus NEXA user?
A MAP is the individualized program stored in the external processor. It defines:
- Threshold levels (T-levels): minimum current for perception
- Comfort levels (C-levels / M-levels): maximum comfortable stimulation
- Dynamic range: the range between T and C levels for each electrode channel
Programming requires manufacturer-specific software (Custom Sound for Cochlear). The audiologist adjusts per-electrode settings based on the patient's loudness judgments.
Q14. What objective tools assist in Nucleus mapping?
- Neural Response Telemetry (NRT) — Cochlear Corporation's tool; measures the Electrically Evoked Compound Action Potential (ECAP) from the auditory nerve directly through the implant. Useful in young children or non-cooperative patients who cannot provide behavioral responses
- Electric Acoustic Stapedial Reflex Thresholds — correlate well with comfort levels; useful when NRT is unavailable
- Aided audiogram — verifies the overall map but cannot confirm loudness or sound quality adequacy
Q15. When are the most map changes expected?
The greatest frequency of programming changes occurs in the first few months after activation as the nervous system and cortex adapt to electric stimulation. Stimulus levels stabilize over time, after which only fine-tuning adjustments are typically needed. Anecdotally, hormonal changes (pregnancy, puberty, menopause) may also trigger the need for map adjustments.
SECTION 6: OUTCOMES & PERFORMANCE
Q16. What are the expected speech perception outcomes with the Nucleus system?
- In patients with >6 months implant experience:
- Open-set word recognition: mean approximately 25%–55% (wide range: 0–100%)
- Open-set sentence recognition: mean scores >80% in quiet with current processing strategies
-
85% of implant recipients achieve meaningful engagement with the hearing world (speech in quiet)
- Performance continues to improve up to 3 years post-implant, with smaller but continued gains beyond that
— Cummings Otolaryngology, pp. 3110, 3444
Q17. What factors predict better outcomes with cochlear implantation?
| Favorable | Unfavorable |
|---|---|
| Short duration of deafness | Long-standing (pre-lingual) deafness |
| Post-lingual deafness | Pre-lingual deafness in adults |
| Higher pre-op speech recognition | No residual hearing at all |
| Younger age at implantation | Cognitive decline / dementia |
| Good cochlear nerve integrity | Cochlear nerve deficiency |
| Motivated patient + active rehabilitation | Lack of auditory training post-implant |
| No cochlear ossification | Significant ossification / malformation |
Q18. What are the benefits of bilateral Nucleus cochlear implantation?
- Head shadow effect — the ear farther from noise receives a better signal-to-noise ratio
- Binaural summation — combined input from both ears improves speech in noise
- Binaural squelch — the ear near the noise source can extract useful signal
- Sound localization — significantly improved Bilateral implantation is now routinely recommended unless contraindicated.
— Cummings Otolaryngology, p. 3076
Q19. What is electroacoustic stimulation (EAS), and how does the Nucleus Hybrid deliver it?
EAS combines:
- Electric stimulation from the short CI electrode array (mid and high frequencies)
- Acoustic amplification via a hearing aid component (low frequencies, typically <1 kHz) — in the same ear
Advantages of EAS over standard CI:
- Superior speech-in-noise performance
- Better melody recognition and music appreciation
- More faithful pitch differentiation through preserved low-frequency acoustic hearing
A subset of patients loses residual hearing post-implantation despite soft surgical technique; they then revert to standard electric-only CI use.
— Cummings Otolaryngology, pp. 3538–3565
SECTION 7: REHABILITATION
Q20. What does post-activation rehabilitation for a Nucleus NEXA user involve?
- Consistent, frequent exposure to conversational speech
- Auditory training targeting: sound detection → discrimination → identification → comprehension
- Goals are highly individualized depending on age, duration of deafness, and communication needs
- Adults must learn to re-associate electrical signals with familiar sound patterns — this takes months
- Music perception tasks are increasingly used as a tool to evaluate and push complex auditory performance
- Regular follow-up with a CI-specialized audiologist for device programming optimization
Q21. Why is rehabilitation mandatory after cochlear implantation — not just device activation?
Hearing through a CI is not the same as normal hearing. The brain requires time and training to interpret the novel electrical signals as meaningful sound. Higher communicative skills (language comprehension, speech-in-noise, music) require active cortical learning beyond mere peripheral sound detection. Studies confirm that auditory training produces measurable improvements in vowel and speech recognition beyond what activation alone achieves.
— Cummings Otolaryngology, pp. 3450, 3705–3720
SECTION 8: SURGICAL & SAFETY POINTS
Q22. What imaging is mandatory before Nucleus cochlear implantation?
- MRI (T2-weighted, e.g., CISS/FIESTA): Gold standard for confirming cochlear nerve presence and cochlear patency (fluid vs. fibrosis)
- High-resolution CT temporal bone: Evaluates cochlear anatomy, ossification, malformations, and surgical route planning
Both modalities are complementary — CT is superior for bony anatomy and electrode placement confirmation; MRI is superior for soft tissue and nerve assessment.
Q23. What are the contraindications to Nucleus cochlear implantation?
- Absence of cochlear nerve (absolute)
- Cochlear aplasia (Michel deformity — absolute)
- Active middle ear infection (relative — treat first)
- Uncontrolled systemic disease affecting wound healing (relative)
- Significant central auditory processing disorder or cognitive impairment (relative — counselling needed)
Q24. What is Neural Response Telemetry (NRT) and what is its clinical significance?
NRT is Cochlear Americas' intraoperative and postoperative tool that measures the Electrically Evoked Compound Action Potential (ECAP) — the direct electrical response of the auditory nerve to stimulation through the Nucleus implant. Clinical uses:
- Confirms electrode–nerve contact and auditory nerve viability intraoperatively
- Guides initial MAP thresholds in non-cooperative or pediatric patients
- Helps identify poorly functioning electrodes
- NRT levels fall between T-levels and C-levels on the MAP
Equivalent for Advanced Bionics is Neural Response Imaging (NRI).
Q25. What is the significance of the Nucleus implant's thin profile (3.9 mm)?
The slim 3.9 mm thickness of the receiver/stimulator:
- Reduces the extent of bone bed drilling needed during surgery
- Lowers risk of skin flap complications (thin flap over a thick implant risks pressure necrosis and extrusion)
- Improves cosmetic outcome, particularly important in children with thin scalp tissue
- Reduces the lateral profile under the scalp
These viva questions cover the full spectrum from device anatomy and electrode design to candidacy, mapping, outcomes, and surgical considerations — exactly the depth expected in ENT/Otology oral examinations and clinical team meetings.
This is a shared conversation. Sign in to Orris to start your own chat.