40-year-old male who is a known alcoholic, diagnosed to have cirrhosis with portal hypertension, who are gone for grade 2 esophageal varices, for which banding has been done 2 years back. Now presented with a volume overload state. I don't know what is the cause of cirrhosis for him. His brother, who is around 50 years, currently also has cirrhosis with decompensation. SAG came back as high SAG, high protein with 24-hour copper serum, serum ceruloplasmin, and the KF rings were negative for Wilsons. His hepatic viral panel, HBV and anti-HCV were negative. I don't know how to proceed with this case.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have everything needed for a comprehensive, well-structured answer. Let me synthesize this.
Clinical Analysis & Approach
This is a genuinely complex case. The key to unlocking it lies in one finding that contradicts the assumed diagnosis: High SAAG + High ascitic protein.
Step 1: Interpret the SAAG + Ascitic Protein Combination
This is the pivotal clue. Here's the logic:
| SAAG | Ascitic Protein | Interpretation |
|---|---|---|
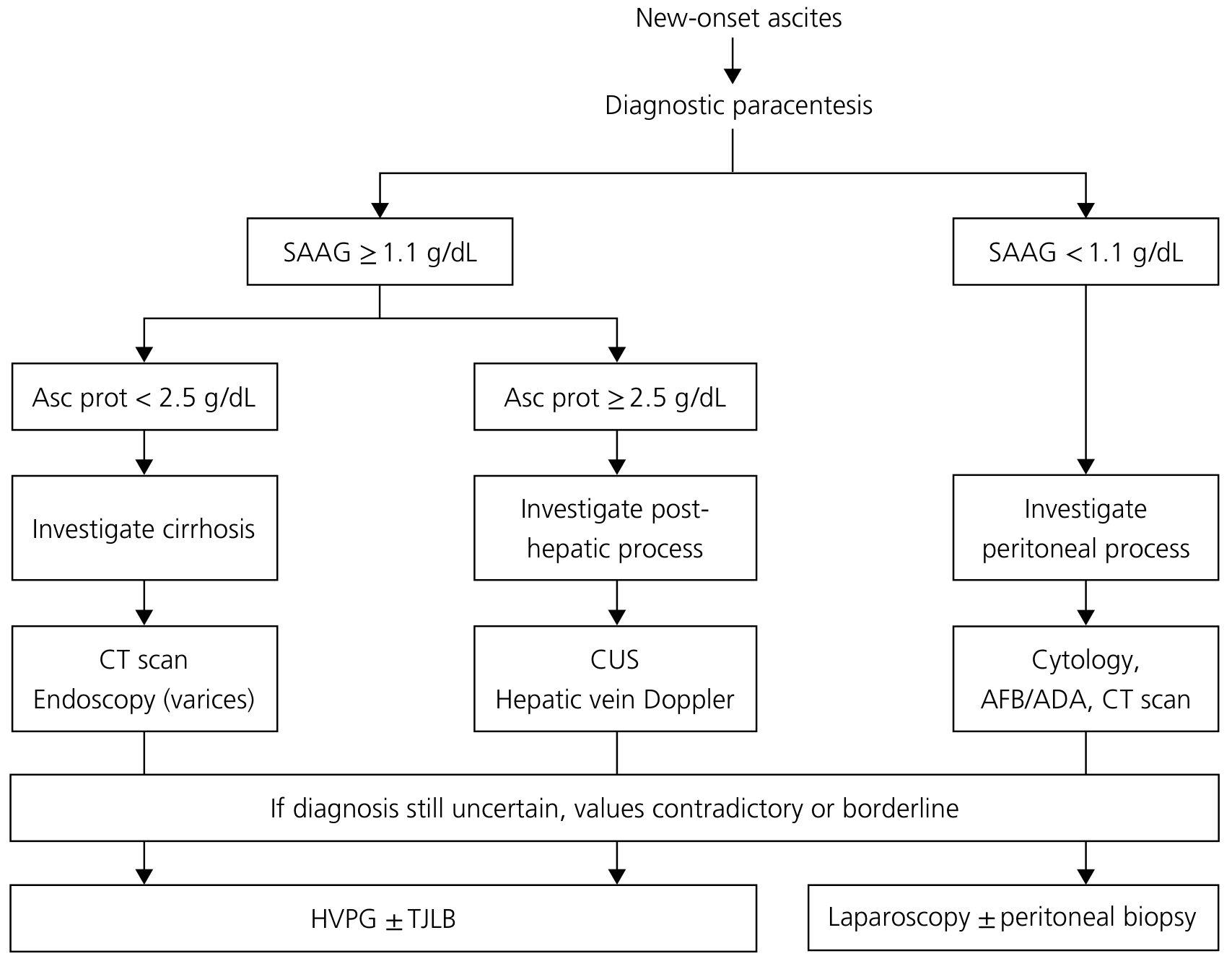
| ≥1.1 g/dL | < 2.5 g/dL | Intrahepatic portal hypertension → cirrhosis (sinusoidal capillarization prevents protein leak) |
| ≥1.1 g/dL | ≥ 2.5 g/dL | Post-hepatic process → hepatic sinusoids are normal and leaky (Budd-Chiari, cardiac, sinusoidal obstruction) |
"In cirrhosis, there is deposition of fibrous tissue in the sinusoids ('capillarization of the sinusoid'), which renders the sinusoids less leaky to macromolecules and this leads to an abnormally low protein content of liver lymph. Therefore… the ascites total protein allows differentiation between intrahepatic causes of ascites (low protein) versus post-hepatic causes (e.g., heart failure, Budd-Chiari) of ascites (high protein), in both of which the SAAG is elevated." — Yamada's Textbook of Gastroenterology, 7e
This patient's high SAAG + high protein tells you his portal hypertension is post-hepatic or non-cirrhotic in mechanism, even though he has known cirrhosis. The cirrhosis itself may not be causing his current volume overload state, or there is an additional/underlying etiology driving it.
Step 2: Differential Diagnosis for High SAAG + High Protein
Causes per Harrison's (22e) and Yamada's:
- Budd-Chiari syndrome (hepatic vein or IVC outflow obstruction)
- Cardiac causes — right heart failure, constrictive pericarditis, alcoholic cardiomyopathy
- Sinusoidal obstruction syndrome (veno-occlusive disease)
"An ascitic protein level of ≥2.5 g/dL indicates that the hepatic sinusoids are normal and are allowing passage of protein into the ascites, as occurs in cardiac ascites, early Budd-Chiari syndrome, or sinusoidal obstruction syndrome." — Harrison's Principles of Internal Medicine, 22e
Step 3: The Crucial Context — Familial Cirrhosis
He is a 40-year-old alcoholic with an unknown etiology of cirrhosis, and his 50-year-old brother also has cirrhosis with decompensation. This familial pattern, combined with alcohol (which accelerates fibrosis in metabolic/storage disorders), strongly raises:
Hereditary Hemochromatosis (HH)
- Autosomal recessive (HFE gene, C282Y, H63D mutations) — brother affected is consistent
- Alcohol independently increases hepatic iron accumulation and accelerates progression
- Wilson's has been excluded; viral hepatitis excluded
- HH is the most common hereditary liver disease in Northern European descent
- Cirrhosis from HH in the context of alcoholism is well recognized
Other considerations:
- Alpha-1 antitrypsin deficiency (autosomal codominant, can affect siblings)
- Non-alcoholic/metabolic fatty liver disease with a familial metabolic predisposition (though less likely in known alcoholic)
- Autoimmune hepatitis (can cluster in families, though less strongly genetic)
Step 4: Immediate Investigations to Order
A. For the volume overload mechanism (High SAAG + High Protein pathway):
| Test | Rationale |
|---|---|
| Serum BNP/NT-proBNP | BNP >365 pg/mL has greater diagnostic accuracy than SAAG+protein for cardiac ascites — Yamada's |
| Echocardiogram | Alcoholic cardiomyopathy, constrictive pericarditis (a curable cause of ascites) |
| Doppler USG of hepatic veins + IVC | Rule out Budd-Chiari syndrome (hepatic vein thrombosis) |
| CT abdomen with contrast/MRI liver | Hepatic vein patency, caudate lobe hypertrophy (Budd-Chiari sign), liver morphology |
"This distinction between cardiac or hepatic origin of ascites is especially important in alcoholic patients who can have ascites secondary to alcoholic cardiomyopathy or from cirrhosis, with significant management implications." — Yamada's Textbook of Gastroenterology, 7e
"Constrictive pericarditis is one of the few curable causes of ascites." — Yamada's
B. For the underlying etiology of cirrhosis (familial + unknown):
| Test | Rationale |
|---|---|
| Serum ferritin + transferrin saturation | Screen for hereditary hemochromatosis (ferritin >1000 µg/L, Tsat >45% are suspicious) |
| HFE gene mutation analysis (C282Y, H63D) | Confirm HH genetically |
| Alpha-1 antitrypsin level + phenotype (Pi typing) | Rule out A1AT deficiency |
| ANA, ASMA, anti-LKM1, IgG | Autoimmune hepatitis |
| Liver biopsy (transjugular if coagulopathic) | Definitive histology for etiology, iron staining, staging |
| Screen the brother similarly | If HH confirmed, siblings have 25% chance of homozygosity |
Step 5: Management Priorities (Immediate)
- Do not manage blindly as "decompensated cirrhosis ascites" — if the etiology is cardiac or Budd-Chiari, the management is fundamentally different
- Therapeutic paracentesis for symptom relief while investigations proceed
- Stop alcohol — critical regardless of etiology
- If Budd-Chiari confirmed: anticoagulation, TIPS, or transplant evaluation
- If cardiac/constrictive pericarditis: pericardiectomy or heart failure management
- If hereditary hemochromatosis: phlebotomy program (after stabilization), screen family members
Summary Diagnostic Roadmap
High SAAG + High Protein
↓
Rule out POST-HEPATIC cause:
→ Echo + BNP (cardiac/constrictive)
→ Hepatic vein Doppler/CT (Budd-Chiari)
↓
Establish ETIOLOGY of cirrhosis (familial):
→ Iron studies + HFE genotype (HH)
→ A1AT phenotype
→ Autoimmune panel
→ Liver biopsy (TJLB if coagulopathic)
The combination of familial cirrhosis of unknown cause + alcoholism in a young male should make hereditary hemochromatosis your top working diagnosis for etiology, while the high SAAG + high protein demands you first rule out Budd-Chiari syndrome and cardiac causes as the driver of his current decompensation.
This is a shared conversation. Sign in to Orris to start your own chat.