Now I am a learner pls teach me FULL VNG INTERPRETATION
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Searching Images
VNG videonystagmography caloric test nystagmus interpretation diagram
Loading Image
Loading Image
Now I have enough material for a comprehensive, well-structured VNG interpretation guide. Let me compose it.
Full VNG (Videonystagmography) Interpretation
Sources: K.J. Lee's Essential Otolaryngology; Cummings Otolaryngology Head & Neck Surgery; Bradley & Daroff's Neurology in Clinical Practice; Harrison's Principles of Internal Medicine 22e
1. What is VNG?
Videonystagmography (VNG) records eye movements directly using infrared video cameras mounted inside goggles. It is the modern replacement for ENG (electronystagmography, which used skin electrodes to measure corneoretinal potential).
VNG captures:
- Horizontal, vertical, and (with 3D systems) torsional eye movements
- Real-time or recorded nystagmus
- Quantified slow-phase eye velocity (SPV) for all subtests
The full VNG battery has two major divisions: oculomotor (central) tests and vestibular tests.
2. The VNG Battery — Overview
| Division | Subtests |
|---|---|
| Oculomotor | Saccades, Smooth Pursuit, Optokinetic, Gaze, Fixation |
| Vestibular | Spontaneous Nystagmus, Positional, Positioning (Dix-Hallpike), Caloric |
3. Oculomotor Subtests
3a. Saccades
- What it tests: Voluntary rapid eye movements to jump between targets
- Normal: Accurate, fast, symmetric
- Abnormal patterns:
- Hypometric (undershoots) → cerebellar or brainstem disease
- Hypermetric (overshoots) → cerebellar dysfunction
- Slow saccades → brainstem pathology, drugs, progressive supranuclear palsy
- Asymmetric latency → frontal lobe lesion on the side with prolonged latency
3b. Smooth Pursuit
- What it tests: Ability to smoothly track a slow-moving target
- Normal: Smooth, symmetric gain ~1.0
- Abnormal: Cogwheeling / saccadic intrusions (pursuit "breaks up") → central pathology (cerebellum, brainstem, diffuse CNS disease, medications, age)
3c. Optokinetic Nystagmus (OKN)
- What it tests: Reflexive nystagmus in response to a full-field moving pattern
- Normal: Symmetric OKN in both directions
- Abnormal: Asymmetric or absent OKN → parieto-occipital or brainstem lesion
3d. Gaze Testing
- What it tests: Stability of gaze held at eccentric positions (left, right, up, down)
- Normal: No nystagmus at gaze
- Gaze-evoked nystagmus (GEN):
- Beats in the direction of gaze
- Unilateral GEN → ipsilateral cerebellar or brainstem lesion
- Bilateral GEN (both directions) → drugs (alcohol, anticonvulsants, sedatives), bilateral cerebellar disease
- Direction-changing GEN = strongly central
3e. Fixation Suppression (Critical differentiator!)
- The normal VOR is suppressed when the eyes fix on a target moving with the head
- Intact fixation suppression = peripheral lesion
- Failure of fixation suppression (nystagmus continues despite fixation) = central lesion (vestibulocerebellum, especially flocculus/nodulus)
4. Vestibular Subtests
4a. Spontaneous Nystagmus
What it is: Nystagmus present in the straight-ahead gaze position, without visual fixation (tested in darkness or with eyes closed under VNG goggles).
Interpretation:
| Finding | Significance |
|---|---|
| Present, direction-fixed, suppressed by fixation | Peripheral (unilateral vestibular loss — acute neuritis, labyrinthitis) |
| Present, direction-changing | Central (does not respect Alexander's law) |
| Suppressed by fixation | Peripheral |
| NOT suppressed by fixation (failure of fixation suppression) | Central |
| Beats toward the healthy ear in acute vestibular neuritis | Peripheral (normal expected finding) |
Alexander's Law: In peripheral nystagmus, intensity increases when gaze is directed toward the fast phase and decreases when gaze is toward the slow phase.
4b. Positional Nystagmus (Static)
The patient is placed in various head/body positions (supine, left lateral, right lateral, head-right, head-left) and held there. Nystagmus is observed in darkness.
Types and interpretation:
| Type | Direction | Fatigues? | Latency | Most Likely |
|---|---|---|---|---|
| Cupulolithiasis BPPV | Geotropic or apogeotropic | No | No | Canalithiasis variant |
| Central positional | Variable, direction-changing, vertical | No | No | Central lesion |
| Persistent apogeotropic (canals) | Apogeotropic | May or may not | No | Canal cupulolithiasis |
Key rule: Persistent, non-fatiguing, direction-changing positional nystagmus = central until proven otherwise.
4c. Positioning (Dynamic) Nystagmus — Dix-Hallpike
Patient is rapidly moved from sitting to head-hanging position.
Classic BPPV (posterior canal):
- Latency: 1–5 seconds before nystagmus starts
- Direction: Upbeat + torsional (top pole beats toward the affected/lower ear)
- Duration: < 60 seconds (usually 20–30 s)
- Fatigues with repeated testing
- Reversal: Nystagmus reverses when patient sits back up
Atypical features suggesting central cause:
- No latency (immediate onset)
- No fatigue
- Pure vertical (downbeat or upbeat) without torsional component
- Duration > 60 seconds
- Nystagmus in direction opposite to expected
4d. Bithermal Caloric Testing — The Core of VNG
This is the most important and quantitative vestibular test.
Principle
- Each ear is irrigated with warm (44°C) and cool (30°C) water (or air: 58°C / 24°C) for 30 seconds (water) or 60 seconds (air).
- The temperature gradient creates convection currents in the endolymph of the lateral (horizontal) semicircular canal, producing a controlled, measurable nystagmus.
Mnemonic — COWS:
Cold Opposite, Warm Same
- Cool irrigation → nystagmus beats AWAY from the irrigated ear
- Warm irrigation → nystagmus beats TOWARD the irrigated ear
Why this works (physiology):
- Cool → endolymph falls → ampullofugal flow → hair cell inhibition → slow eye drift toward irrigated ear → compensatory fast phase away
- Warm → endolymph rises → ampullopetal flow → hair cell excitation → slow drift away from irrigated ear → fast phase toward irrigated ear
The Four Measurements
The peak slow-phase eye velocity (SPV) is measured for each of the four irrigations:
- RW = Right Warm | RC = Right Cool | LW = Left Warm | LC = Left Cool
4e. Caloric Formulas
Unilateral Weakness (UW) — Jongkees Formula
$$UW = \frac{(RW + RC) - (LW + LC)}{RW + RC + LW + LC} \times 100%$$
- Normal: < 20–25% (lab-dependent; most use 20–25%)
- Abnormal: > 20–25% → reduced response on the weaker side = peripheral vestibular hypofunction
- Points to the side with lower total response (i.e., the side contributing less to the numerator being positive = right side weak if UW is positive and right values are low)
Directional Preponderance (DP)
$$DP = \frac{(RW + LC) - (LW + RC)}{RW + RC + LW + LC} \times 100%$$
- Normal: < 30%
- Abnormal DP = nystagmus beats more strongly in one direction
- DP toward the side of lesion suggests central; DP away from lesion suggests peripheral (still debated)
- DP alone without UW is non-localizing
Bilateral Weakness (BW)
- Total response of both sides < 12°/s (lab-dependent)
- i.e., LW + LC < 12°/s AND RW + RC < 12°/s
- Suggests bilateral vestibular loss (ototoxicity, bilateral Menière's, autoimmune labyrinthopathy)
5. Caloric Trace Interpretation — Real Images
Normal bilateral caloric traces:
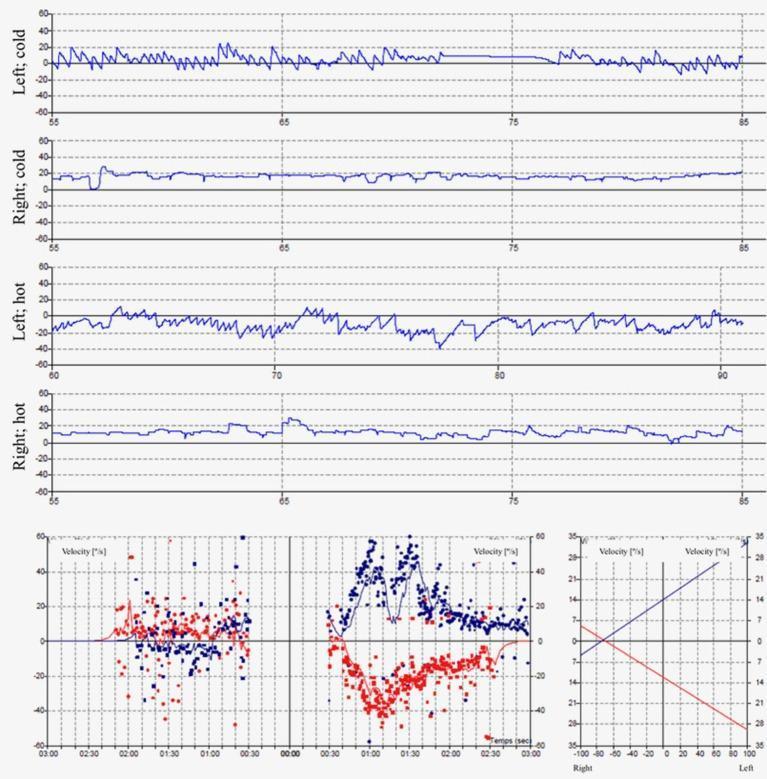
The left ear (top two panels) shows robust nystagmus responses to both cold and hot irrigation. The right ear panels show nearly flat traces (SPV ≤ 5°/s) = right vestibular areflexia.
Caloric inversion (central finding):
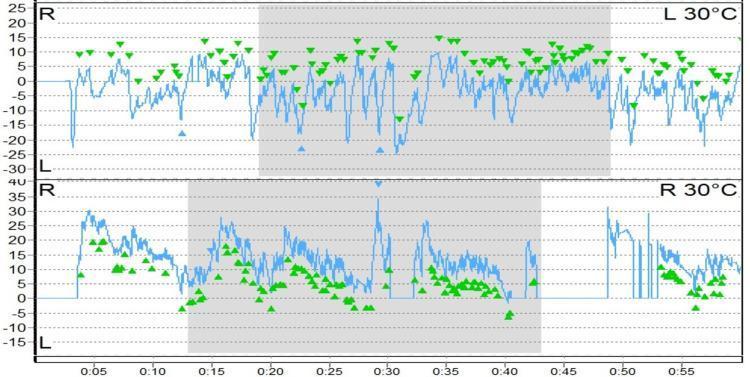
Both ears show cold irrigation (L 30°C top, R 30°C bottom). Green arrowheads mark peak SPV. The nystagmus beats in the OPPOSITE direction to what COWS predicts = caloric inversion = highly suggestive of central (brainstem) pathology.
6. Pattern Recognition — Central vs. Peripheral Summary
| Feature | Peripheral | Central |
|---|---|---|
| Spontaneous nystagmus | Direction-fixed | Direction-changing |
| Fixation suppression | Present (suppresses nystagmus) | Absent (fails to suppress) |
| Caloric responses | Unilateral or bilateral weakness | Normal, hyperactive, or inverted |
| Bilateral weakness + normal calorics | Uncommon | Suggests central |
| Abnormal saccades/pursuit | Absent (calorics usually abnormal) | Present (calorics may be normal) |
| Positional nystagmus | Fatiguing, direction-fixed | Non-fatiguing, direction-changing |
| Dix-Hallpike | Latency + fatigue + torsional | No latency, no fatigue, purely vertical |
| Hyperactive calorics | If TM defect / mastoid cavity | Loss of cerebellar inhibition |
| Bilateral absent calorics | Ototoxicity, labyrinthine disease | Bilateral vestibular nuclei lesion |
7. Findings That Are ALWAYS Central
Memorize these red flags:
- Failure of fixation suppression
- Direction-changing spontaneous nystagmus
- Spontaneous or positional nystagmus with NORMAL calorics (central nystagmus generator, not the labyrinth)
- Abnormal saccades or broken pursuit with normal calorics
- Bilateral caloric weakness without history of ototoxicity or labyrinthine disease
- Hyperactive caloric responses (absent cerebellar inhibition) without TM perforation
- Purely vertical positioning nystagmus (no torsional component)
- Caloric inversion
8. Findings That Are ALWAYS Peripheral
- Unilateral caloric weakness (abnormal UW formula)
- Bilateral caloric weakness WITH history of ototoxicity/labyrinthine disease
- Intact fixation suppression on nystagmus
- Direction-fixed nystagmus that obeys Alexander's law
- Fatiguing positional nystagmus
- Classic Dix-Hallpike response (latency + torsional + fatigue)
9. Clinical Correlation — Common Diagnoses on VNG
| Diagnosis | Typical VNG Pattern |
|---|---|
| Vestibular neuritis | UW on affected side; direction-fixed spontaneous nystagmus beating away from lesion; intact fixation suppression |
| BPPV (posterior canal) | Normal calorics; classic Dix-Hallpike with upbeat-torsional nystagmus, latency, fatigue |
| Menière's disease | Unilateral caloric weakness (often); DP may be present; spontaneous nystagmus during acute attack |
| Acoustic neuroma/schwannoma | UW on tumor side; may have abnormal saccades if large |
| Cerebellar stroke | Normal or hyperactive calorics; failure of fixation suppression; broken pursuit; abnormal saccades; direction-changing nystagmus |
| Brainstem lesion | Multiple oculomotor abnormalities; may show caloric inversion |
| Bilateral vestibular loss | Bilateral caloric weakness + oscillopsia + absent dynamic visual acuity |
| Drug/medication effect | Bilateral GEN; broken pursuit; symmetrically depressed or normal calorics |
10. Practical Considerations Before/During Testing
- Otoscopy first — always inspect TM before calorics
- Water is contraindicated with TM perforation → use air calorics instead (perforated side will show an artificially heightened response)
- Excess cerumen must be cleared — it impedes heat transfer and gives falsely reduced responses
- Medications that suppress the CNS (benzodiazepines, antihistamines, anticonvulsants) must be stopped 48–72 hours before testing — they depress nystagmus responses and create false findings
- Patient must be alert and mentally stimulated (asked to count or name items) during caloric testing — mental alertness maximizes nystagmus amplitude
11. Quick Summary Flowchart
VNG Result
│
├── Abnormal CALORICS?
│ ├── Unilateral weakness → Peripheral (ipsilateral)
│ ├── Bilateral weakness + ototoxicity hx → Peripheral (bilateral)
│ ├── Bilateral weakness, no hx → CENTRAL
│ └── Hyperactive / inverted → CENTRAL
│
├── Normal CALORICS but NYSTAGMUS present?
│ └── → CENTRAL (nystagmus generator, not labyrinth)
│
├── Fixation suppression ABSENT?
│ └── → CENTRAL (vestibulocerebellum)
│
├── Abnormal SACCADES / PURSUIT with normal calorics?
│ └── → CENTRAL (brainstem/cerebellum)
│
└── UW + direction-fixed + fixation suppresses + normal oculomotor?
└── → PERIPHERAL
Key Formula Card
| Metric | Formula | Cutoff |
|---|---|---|
| Unilateral Weakness | [(RW+RC)−(LW+LC)] / (RW+RC+LW+LC) × 100% | >20–25% = abnormal |
| Directional Preponderance | [(RW+LC)−(LW+RC)] / (RW+RC+LW+LC) × 100% | >30% = significant |
| Bilateral Weakness | LW+LC < 12°/s AND RW+RC < 12°/s | Both sides < 12°/s |
— K.J. Lee's Essential Otolaryngology, pp. 349–352 | Cummings Otolaryngology Head & Neck Surgery | Harrison's Principles of Internal Medicine 22e | Bradley & Daroff's Neurology in Clinical Practice
Deeper focus with reference values in one pdf
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
VNG oculomotor saccade pursuit optokinetic normal abnormal tracing interpretation
Running Command
Writing File
Running Command
VNG Interpretation Deep Reference
PDF Document · PDF
If you want, I can also produce a second version with:
- exam-style MCQs + answer key, or
- a 1-page rapid-reference sheet for clinic use.
This is a shared conversation. Sign in to Orris to start your own chat.