Tapering dose of medrol in RA
Reading File
Finding Sources
Finding Sources
Searching PubMed
glucocorticoid tapering rheumatoid arthritis
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching the Web
Medrol methylprednisolone tapering schedule rheumatoid arthritis EULAR 2025
Here is a comprehensive, clinically practical guide to tapering Medrol (methylprednisolone) in RA:
Medrol (Methylprednisolone) Tapering in Rheumatoid Arthritis
Role of Glucocorticoids in RA
Medrol is used in RA primarily as a bridging agent - to control inflammation while a csDMARD (most often methotrexate) builds up to its therapeutic effect. It can also be used during acute flares. The overarching goal is always the lowest effective dose for the shortest possible time, as stated in both EULAR 2025 guidance and major rheumatology textbooks.
Methylprednisolone Dose Equivalence
Methylprednisolone 4 mg = Prednisone 5 mg (both intermediate-acting, preferred over long-acting dexamethasone in RA). The common Medrol tablet strengths are 4 mg and 16 mg.
| Prednisone equivalent | Methylprednisolone (Medrol) dose |
|---|---|
| 5 mg/day | 4 mg/day |
| 10 mg/day | 8 mg/day |
| 20 mg/day | 16 mg/day |
| 30–40 mg/day (acute flare) | 24–32 mg/day |
Starting Doses in RA
Bridging therapy (DMARD initiation):
- Oral: up to prednisone 30 mg/day equivalent (= Medrol ~24 mg/day), though typical practice uses lower: 8–16 mg/day
- Single IM injection: methylprednisolone 120 mg (Depo-Medrol)
- IV pulse: 250 mg methylprednisolone single dose
Typical maintenance/bridging starting dose: Medrol 8 mg/day (= prednisone 10 mg)
Acute flare: Medrol 16–32 mg/day, with rapid taper thereafter
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1036
Tapering Schedule
The taper rate depends on the starting dose, duration of use, and disease activity.
Short course (acute flare, <2–4 weeks use)
Rapid taper over 1–3 weeks:
| Week | Medrol Dose |
|---|---|
| Starting dose | 16–32 mg/day |
| Week 1 | Reduce by 4–8 mg every 2–3 days |
| Week 2 | 8 mg/day |
| Week 3 | 4 mg/day |
| Week 4 | Stop |
Bridging course (DMARD initiation, typical 3–6 months)
Slower, stepwise taper - target discontinuation by 3 months (exceptionally 6 months):
| Time point | Medrol dose | Comments |
|---|---|---|
| Weeks 1–2 | 8–16 mg/day | Starting dose with DMARD initiation |
| Month 1 | 8 mg/day | Reduce if disease controlled |
| Month 2 | 4–6 mg/day | DMARD should be taking effect |
| Month 3 | 2–4 mg/day | Aim for lowest dose |
| Month 3–6 | Stop | Taper 1–2 mg every 2–4 weeks below 4 mg |
EULAR 2025 recommendation: Short-term GCs with MTX; taper and ideally stop, usually within 3 months.
Chronic low-dose GC (if long-term use necessary)
If the patient is on Medrol 4–8 mg/day long-term (e.g., SEMIRA trial scenario with biologics):
- Reduce by 1 mg every 4–8 weeks
- At doses ≤4 mg/day: taper even more slowly (1 mg every 2–3 months)
- The SEMIRA trial showed that ~2/3 of RA patients on tocilizumab + prednisone 5 mg/day were able to taper off without a flare; one-third experienced flares requiring restart
- Firestein & Kelley's Textbook of Rheumatology, p. 1209
Key Clinical Principles
- Taper is guided by disease activity - use DAS28 or clinical assessment; do not taper mechanically if disease remains active
- EULAR 2025 recommends GCs as short-term bridge alongside MTX; goal is discontinuation, not long-term use
- Attempted GC tapering should be done for any patient in low disease activity - many can successfully stop
- Worsening on taper = consider DMARD adjustment or biologic escalation, not just restarting GCs
- Below physiologic threshold (~Medrol 3 mg/day = prednisone ~4 mg/day): taper very slowly to avoid HPA axis insufficiency; consider morning cortisol assessment if concerned
- Infection risk even at low doses (≤Medrol 4 mg/day = prednisone 5 mg/day) - counsel patients accordingly
- Always co-prescribe bone protection (calcium + vitamin D; consider bisphosphonate) for courses >3 months
Routes in Bridging
| Route | Dose | Use case |
|---|---|---|
| Oral Medrol | 8–24 mg/day, taper as above | Standard bridging |
| IM Depo-Medrol | 80–120 mg single injection | Patients who prefer or cannot comply with oral; covers ~4–6 weeks |
| IV methylprednisolone | 250–500 mg single pulse | Severe flare, vasculitic features |
| Intra-articular (triamcinolone) | 5–20 mg per joint | 1–3 active joints, avoid >3-monthly |
- Rheumatology, 2-Volume Set (Elsevier 2022), p. 536; Goodman & Gilman's, p. 1036
2025 EULAR Update (Current Guidance)
The 2025 EULAR RA management update (PMID 41826212) confirms: MTX ideally in combination with short-term GCs as initial strategy; GC tapering and discontinuation is the goal. With sustained remission, DMARDs (including biologics) may also be tapered cautiously, but stopping everything often leads to flare.
Practical summary: Start at the minimum effective dose (typically Medrol 8 mg/day), taper by 2–4 mg every 2–4 weeks aiming to stop by 3 months. For chronic low-dose use, taper 1 mg every 4–8 weeks. Always reassess disease activity at each step - the taper rate follows the clinical response, not a fixed calendar.
If giving once weekly
Finding Sources
Searching the Web
methylprednisolone Medrol once weekly dosing rheumatoid arthritis tapering schedule
Searching the Web
Medrol 4mg once weekly methotrexate rheumatoid arthritis tapering reduce dose
Great clarifying follow-up. Once-weekly Medrol in RA is a well-recognized Indian rheumatology practice, typically co-administered on the same day as weekly methotrexate to help with MTX-associated nausea and to provide a pulse anti-inflammatory effect.
Once-Weekly Medrol (Methylprednisolone) in RA - Tapering Guide
Why Once Weekly?
This regimen is used in two scenarios:
- Given alongside weekly MTX - the steroid blunts MTX side effects (nausea, fatigue) and provides a burst of anti-inflammatory cover on the active treatment day
- Low-frequency bridging - for patients who cannot or will not take daily steroids, a weekly pulse provides periodic inflammation control
Typical Starting Doses (Once Weekly)
| Disease severity | Medrol weekly dose | Equivalent prednisone |
|---|---|---|
| Mild RA / maintenance | 4–8 mg once weekly | 5–10 mg |
| Moderate RA / bridging | 8–16 mg once weekly | 10–20 mg |
| Moderate-severe / flare | 16–32 mg once weekly | 20–40 mg |
The most commonly used once-weekly dose in Indian practice alongside MTX is Medrol 4–8 mg once a week, taken on the same day as MTX.
Tapering Schedule - Once Weekly Dosing
Since the total weekly steroid exposure is already low, tapering is done by reducing the dose by one tablet (4 mg) every 4–8 weeks, guided by disease activity:
| Time | Medrol Dose (once weekly) | Comment |
|---|---|---|
| Start | 16 mg once weekly | Acute flare / DMARD initiation |
| 4–6 weeks | 12 mg once weekly | If disease settling |
| 2–3 months | 8 mg once weekly | DMARD effect building |
| 3–4 months | 4 mg once weekly | Maintenance phase |
| 5–6 months | 4 mg every 2 weeks | Near discontinuation |
| 6 months | Stop | Target: discontinue by 6 months |
Or for lower starting doses (the common 4–8 mg weekly scenario):
| Time | Dose |
|---|---|
| Months 1–2 | 8 mg once weekly |
| Months 3–4 | 4 mg once weekly |
| Month 5 | 4 mg every 2 weeks |
| Month 6 | Stop |
Key Points for Once-Weekly Dosing
- HPA suppression risk is lower with once-weekly dosing compared to daily dosing - abrupt stopping is generally safer, but still taper if used for >3 months
- Reduce by 4 mg (1 tablet) per step - do not halve the dose abruptly
- Taper trigger: disease in low activity or remission on DAS28; if DAS28 remains elevated, do not taper - escalate DMARD instead
- If flare occurs on taper: step back up one dose level for 4 weeks, then retry taper
- No need to give on an empty stomach - once-weekly dosing is usually with food on MTX day
- HPA axis: once-weekly doses of ≤8 mg Medrol are unlikely to cause clinically significant adrenal suppression; abrupt discontinuation is generally safe at this dose level
- Official Pfizer prescribing information for Medrol notes a maintenance dose of 6–12 mg/day for severe RA and 2–6 mg/day for mild RA - the once-weekly approach represents a significantly lower cumulative dose and is thus favorable from a side-effect standpoint
Practical Summary
For the common Indian RA practice of Medrol 8 mg once weekly with MTX:
- Reduce to 4 mg once weekly after 2–3 months if disease is controlled
- Then 4 mg every 2 weeks for 4 more weeks
- Then stop
- Total steroid exposure is minimal; HPA suppression is not a concern at these doses/frequencies
The goal remains the same: taper and stop within 3–6 months, in line with EULAR guidance on glucocorticoids as short-term bridging in RA.
CSCR in ophtha
Reading File
Finding Sources
Finding Sources
Searching PubMed
"central serous chorioretinopathy" treatment
Reading File
Reading File
Reading Article
PMID: 40513762
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete, clinically structured overview of CSCR:
Central Serous Chorioretinopathy (CSCR)
Definition & Pathophysiology
CSCR is an idiopathic disorder characterized by a localized serous detachment of the neurosensory retina at the macula, secondary to leakage from the choriocapillaris through hyperpermeable RPE sites. It is classified within the pachychoroid spectrum - the choroid is abnormally thick, with dilated outer choroidal vessels (pachyvessels) causing pressure on the choriocapillaris, leading to RPE dysfunction and fluid accumulation under the retina.
- Kanski's Clinical Ophthalmology 10th ed., p. 617
Epidemiology & Risk Factors
| Feature | Detail |
|---|---|
| Classic patient | Young/middle-aged male (20–50 years) |
| Sex ratio | Male : Female = 3:1 (females tend to be older at presentation) |
| Laterality | Usually unilateral; bilateral in ~10–40% |
| Recurrence | Up to 50% of cases |
| Chronic course | ~15% (fluid >12 months) |
Risk factors and associations:
- Exogenous corticosteroids (any route - oral, inhaled, nasal spray, topical skin creams, intravitreal) - the most important modifiable risk factor
- Endogenous hypercortisolism - Cushing syndrome, adrenal adenoma
- Psychological stress / type A personality
- Systemic hypertension
- Sleep apnea syndrome
- Pregnancy
- Helicobacter pylori infection
- Renal dialysis
- Lupus (SLE)
- Genetic: SNP in complement factor H gene (chromosome 1) predisposes to chronic form in White individuals
- Wills Eye Manual 11th ed., p. 830; Kanski's, p. 617
Clinical Features
Symptoms
- Unilateral blurred/dim central vision
- Metamorphopsia (distortion)
- Micropsia (objects appear smaller)
- Mild dyschromatopsia (color desaturation)
- Central scotoma (relative)
- May be asymptomatic
Signs
- Visual acuity: typically 20/20 to 20/200 (6/9 to 6/18)
- Acquired hypermetropia - VA improves with +1 dioptre convex lens (due to retinal elevation)
- Round/oval serous detachment of neurosensory retina at the macula, with sloping margins
- Subretinal fluid (clear or turbid)
- One or more small pigment epithelial detachments (PEDs) within the detachment
- Precipitates on posterior retinal surface
- RPE atrophy/hyperplasia at sites of old lesions (visible on FAF)
- Gravitational tract - fluid tracking inferiorly (best seen on FAF)
- Wills Eye Manual, p. 827–828; Kanski's, p. 617
Classification
| Type | Duration | Features |
|---|---|---|
| Acute CSCR | <3–4 months | Self-limiting, good prognosis, resolves in ~80% |
| Chronic CSCR | >3–4 months (some say >12 months) | RPE changes, photoreceptor damage, permanent visual loss risk |
| Recurrent CSCR | Multiple episodes | Cumulative RPE damage |
| Bullous CSCR | Severe variant | Gravity-dependent detachment, significant SRF |
Investigations
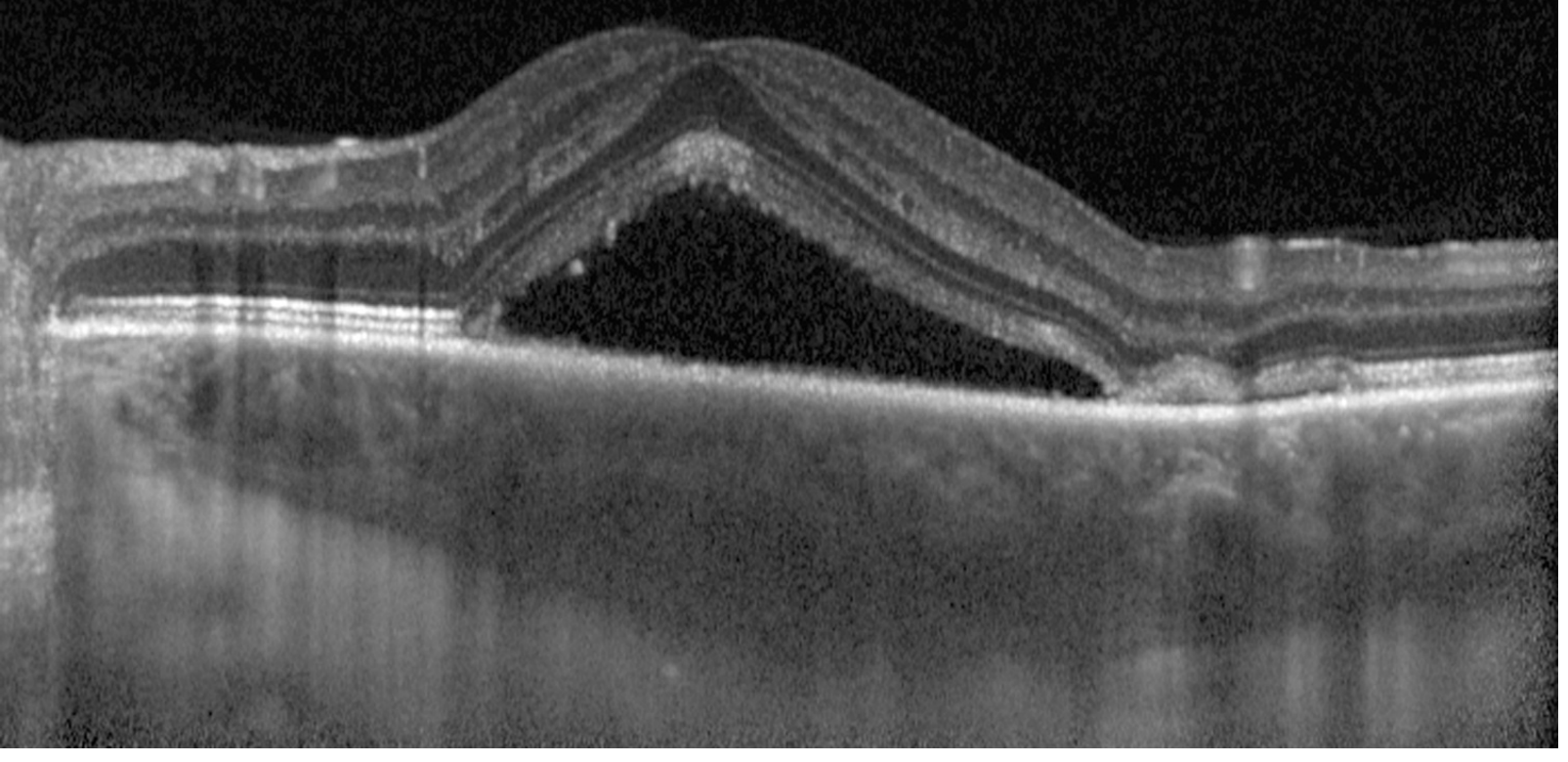
1. OCT (most important clinical tool)
Optically empty (dark) neurosensory elevation with subretinal fluid. May show:
- Underlying PEDs
- Subretinal precipitates/fibrin
- Choroidal thickening (enhanced-depth imaging OCT / EDI-OCT) - hallmark of pachychoroid
- Photoreceptor/RPE degeneration in chronic cases
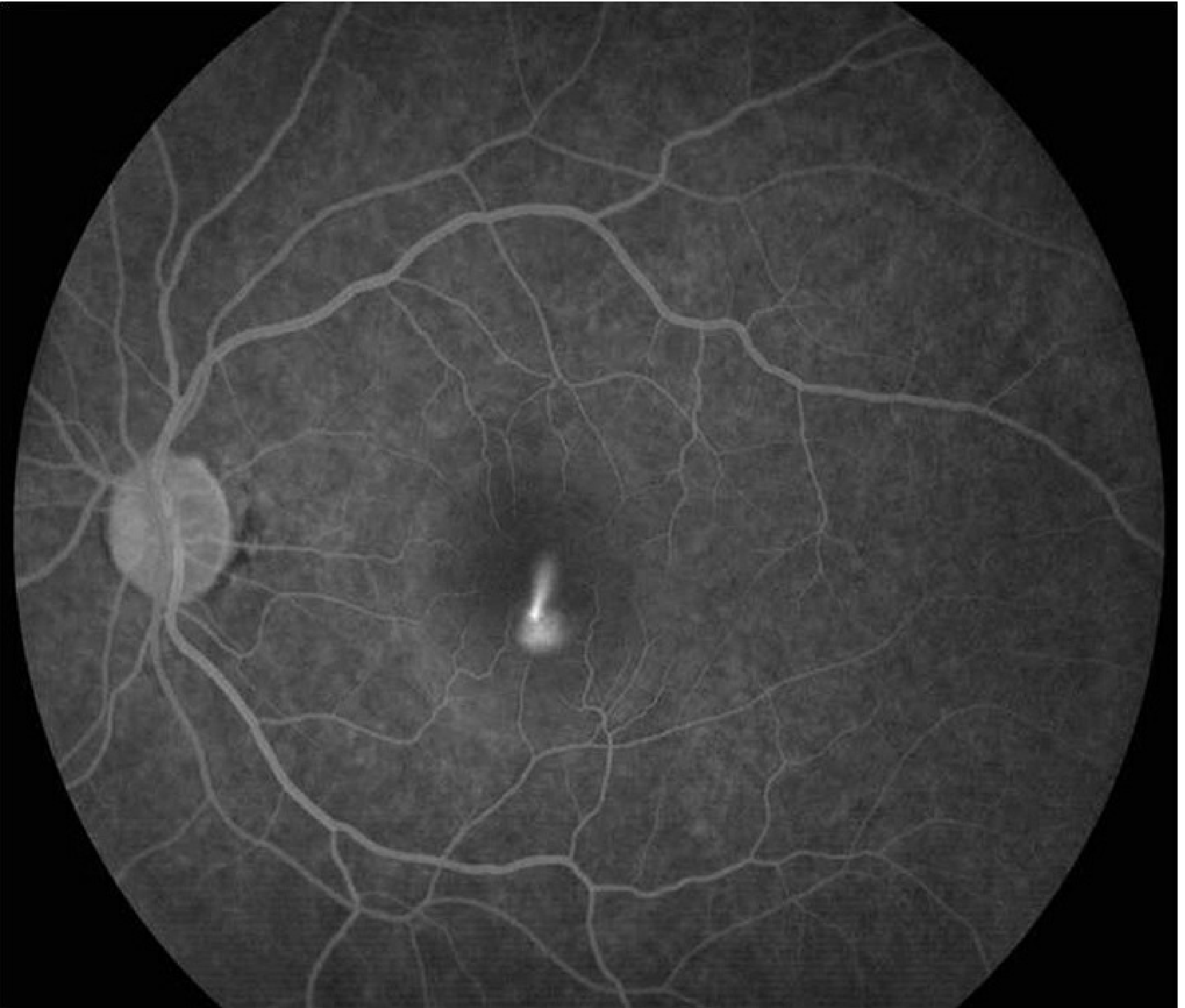
2. Fluorescein Angiography (FA/IVFA)
- Early hyperfluorescent spot at RPE leak site
- Two classic patterns:
- "Ink blot" (most common) - spot enlarges centrifugally
- "Smoke-stack" (10–20% of cases) - vertical column of dye rising upward, then spreading laterally - nearly pathognomonic
3. ICGA (Indocyanine Green Angiography)
- Dilated/compromised outer choroidal vessels
- Mid-phase multifocal hyperfluorescent patches (choroidal hyperpermeability)
- Reveals subclinical foci not visible on FA
- Useful to identify leaking sites before PDT
4. FAF (Fundus Autofluorescence)
- Decreased autofluorescence at leakage site
- Gravitational tract pattern
- Old RPE atrophy visible
5. Amsler Grid
- Confirms metamorphopsia and relative scotoma area
6. Systemic workup in chronic CSCR
- Cortisol levels (rule out Cushing), renal function
- Kanski's, p. 620; Wills Eye Manual, p. 830
Differential Diagnosis
| Condition | Key differentiating features |
|---|---|
| AMD (wet/dry) | Age ≥50, drusen, bilateral, may have CNV/hemorrhage |
| PED | Distinct margins, RPE elevated without overlying SRF |
| Optic pit maculopathy | Serous detachment contiguous with optic disc pit |
| Rhegmatogenous retinal detachment (macular) | History of floaters/flashes, may see break |
| Choroidal tumor | Mass lesion on USG/OCT |
| Uveal effusion syndrome | Peripheral bilateral detachments |
| VKH / posterior uveitis | Bilateral, inflammatory signs, systemic features |
| Hypertensive retinopathy | BP history, hard exudates, AV changes |
Course & Prognosis
- Spontaneous resolution in ~80% within 3–6 months
- Return to near-normal or normal vision in most
- Recurrence in up to 50%
- ~15% follow a chronic course (>12 months) - risk of permanent photoreceptor/RPE damage and reduced VA
- Complications: CNV (choroidal neovascularization), RPE tears, cystoid macular degeneration
Management
1. Observation
Appropriate for acute CSCR with good vision, as most resolve spontaneously. Review every 6–8 weeks.
2. Stop corticosteroids (if possible)
- Discontinue all forms - oral, topical, nasal, inhaled, intravitreal
- TIP from Kanski's: "All forms of corticosteroid treatment should be discontinued if possible in patients with chronic or recurrent CSCR."
- This is the single most important step when steroids are implicated
3. Laser Photocoagulation (conventional)
- May accelerate visual recovery but no proven long-term benefit
- Identifies and treats the RPE leak point on FA
- Risk: CNV formation - use only low-intensity laser
- Indications:
- Persistent SRF for several months
- Recurrence in an eye with permanent prior visual deficit
- Fellow eye involvement after permanent deficit
- Occupational necessity (e.g., pilots, drivers)
4. Subthreshold Micropulse Diode Laser
- Laser applied to RPE leak site without visible burn
- Good results; significantly less retinal damage on OCT than conventional photocoagulation
- Preferred over conventional laser in most centers
5. Photodynamic Therapy (PDT) with Verteporfin
- Treatment of choice for chronic CSCR
- Half-dose / reduced-fluence PDT (30–50% of standard MNV dose, 50% light intensity) - leads to complete resolution including severe chronic cases
- Lower incidence of choroidal ischemia vs. full-dose PDT
- Also considered for rapid SRF resolution in acute CSCR
- Mechanism: reduces choroidal hyperpermeability
6. Mineralocorticoid Receptor Antagonists (MRAs)
- Eplerenone and spironolactone (oral spironolactone 40 mg BD)
- Reduce choroidal vascular hyperpermeability by blocking mineralocorticoid receptors
- Associated with improved anatomic and visual outcomes in chronic CSCR
- A 2025 meta-analysis (PMID 40513762) of 13 studies found MRAs offer short-term benefits in reducing subretinal fluid (faster resolution at 1 month) but PDT outperforms MRAs in long-term SRF reduction
- Spironolactone significantly reduced retinal thickness vs observation
- MRAs were comparable to subthreshold micropulse laser at last follow-up
7. Anti-VEGF (intravitreal)
- Bevacizumab alone is not helpful unless there is associated CNV
- Used in conjunction with PDT when CNV develops as a complication
- Not a first-line treatment for CSCR itself
8. Other agents (limited evidence)
- Aspirin, beta-blockers, mifepristone - case reports only; not standard of care
Management Algorithm
Acute CSCR (<3-4 months)
↓
Stop steroids + Observe for 3 months
↓
Resolved? → Review at 3-6 months
Not resolved / Chronic CSCR?
↓
Half-dose PDT (preferred)
OR Subthreshold micropulse laser
OR Oral MRA (eplerenone/spironolactone)
↓
CNV develops?
↓
Add intravitreal anti-VEGF
Key Points to Remember
- CSCR = pachychoroid spectrum disorder - thick choroid is the underlying anatomical basis
- Steroids (any route) are the most important treatable precipitant - always ask and always stop
- Smoke-stack on FA is nearly pathognomonic (but seen in only 10–20%)
- EDI-OCT showing subretinal fluid + choroidal thickening is the standard diagnostic tool
- Most acute cases resolve without treatment; chronic cases need active intervention
- Half-dose PDT is the most effective treatment for chronic CSCR
- MRAs provide short-term SRF reduction but PDT remains superior long-term
- Recurrence rate up to 50% - follow up is essential
Sources: Kanski's Clinical Ophthalmology 10th ed.; Wills Eye Manual; 2025 Meta-Analysis on MRAs in chronic CSCR (Am J Ophthalmol, PMID 40513762)
Azathioprine and sulfasalazine in pregnancy
Finding Sources
Finding Sources
Searching PubMed
azathioprine sulfasalazine pregnancy rheumatoid arthritis safety
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Here is the full clinical answer:
Azathioprine & Sulfasalazine in Pregnancy
Overview - Safety Classification
| Drug | Pregnancy Safety | Lactation | FDA/Risk |
|---|---|---|---|
| Sulfasalazine | Compatible - minimal risk | Compatible (one case report of bloody diarrhea) | Low risk |
| Azathioprine | Compatible - low-moderate risk | Compatible - low risk | Low to moderate risk |
| Methotrexate | CONTRAINDICATED | Avoid | High risk - teratogenic |
| Leflunomide | CONTRAINDICATED | Avoid | High risk |
| MMF | CONTRAINDICATED | Avoid | High risk - teratogenic |
- Firestein & Kelley's Textbook of Rheumatology, Table 39.6, p. 747
SULFASALAZINE
Mechanism Relevant to Pregnancy
Sulfasalazine crosses the placenta with its metabolite sulfapyridine. It inhibits folate absorption by competitively inhibiting jejunal folate conjugase, which is the main concern in pregnancy.
Teratogenicity
- Case reports of fetal malformations have been published
- However, a large meta-analysis showed no statistically significant increase in congenital anomalies after fetal exposure
- Overall considered safe for use in pregnancy
Key Practical Points
- Continue sulfasalazine throughout pregnancy - it is a good option for active inflammatory arthritis (RA, peripheral SpA) in pregnant women
- Mandatory: higher-dose folic acid supplementation
- Standard pregnancy dose is 0.4–0.5 mg/day; women on sulfasalazine need more
- Goldman-Cecil recommends 1 mg twice daily (2 mg/day total) for women on sulfasalazine who are pregnant or planning pregnancy
- This compensates for impaired folate absorption and prevents neural tube defects
Lactation
- Compatible with breastfeeding
- One isolated case report of bloody diarrhea in a breastfed neonate - but this is rare and overall data support continued use
- Monitor neonate for GI symptoms
- Rheumatology (Elsevier 2022), p. 4493–4507; Goldman-Cecil Medicine, p. 1873
AZATHIOPRINE (AZA)
Mechanism Relevant to Pregnancy
- The placenta in humans cannot metabolize azathioprine to its active form 6-mercaptopurine (6-MP)
- This means little to no biologically active drug actually reaches the fetus - a key reason AZA is considered relatively safe
- Despite this, some 6-MP has been detected in fetal blood, so caution remains appropriate
Teratogenicity Data
- Case reports exist of neonates with: pancytopenia, combined immunodeficiency, chromosomal abnormalities, craniofacial malformations
- However, multiple large case series (including transplant registries) fail to show increased congenital anomaly rates
- Study of 189 azathioprine-exposed vs. 230 control pregnancies: no significant difference in major malformations (3.5% vs. 3.0%)
- Lower mean birth weight and gestational age in AZA group (possibly from preterm delivery or IUGR, not directly teratogenic)
- Conclusion: AZA does not increase risk of congenital anomalies above background rates
Obstetric Risks (Low-Moderate)
All four immunosuppressants (AZA, 6-MP, cyclosporine, tacrolimus) are associated with:
- PROM (premature rupture of membranes)
- SGA (small for gestational age)
- IUGR (intrauterine growth restriction)
These are class effects, not specific to AZA alone.
Indications in Pregnancy
- Steroid-sparing agent for RA, SLE, vasculitis during pregnancy
- Often used to replace mycophenolate (which is teratogenic) in women with lupus nephritis or transplant who become pregnant
- Standard doses used: 1–2 mg/kg/day (same as non-pregnant adults)
Lactation
- AZA is excreted in breast milk in low concentrations
- Considered compatible with lactation by most experts
- Active metabolites (6-MP, 6-TGN) are at low or unmeasurable levels in infant serum
- No adverse effects on infants up to 3 years of age in available data
- Long-term carcinogenesis data in infants are not available - discuss with patients
- Rheumatology (Elsevier 2022), p. 4521–4545; Creasy & Resnik's Maternal-Fetal Medicine, p. 3447; Firestein & Kelley, p. 747
Comparative Summary Table
| Feature | Sulfasalazine | Azathioprine |
|---|---|---|
| Placental transfer | Yes (+ sulfapyridine) | Minimal (placenta cannot convert to 6-MP) |
| Teratogenicity | Not shown in large studies | Not shown in large studies |
| Main fetal concern | Folate deficiency if no supplementation | PROM, SGA, IUGR (class effect) |
| Key action required | High-dose folic acid (2 mg/day) | Monitor fetal growth (serial USG) |
| 1st trimester | Compatible | Compatible |
| 2nd trimester | Compatible | Compatible |
| 3rd trimester | Compatible | Compatible |
| Breastfeeding | Compatible | Compatible (low risk) |
| Contraindicated? | No | No |
| Used for RA in pregnancy? | Yes - preferred option | Yes - preferred option |
What to AVOID in Pregnancy (for context)
| Drug | Reason |
|---|---|
| Methotrexate | Embryotoxic, teratogenic - stop 3 months before conception |
| Leflunomide | Congenital anomalies - requires washout with cholestyramine |
| MMF (mycophenolate) | Strongly teratogenic (ear, limb, heart defects) |
| Cyclophosphamide | Teratogenic |
| NSAIDs | Safe in 1st/2nd trimester; avoid after 20 weeks (oligohydramnios, premature ductus closure) |
Practical Points for RA in Pregnancy
- Plan pregnancy - switch from teratogenic DMARDs (MTX, leflunomide) to AZA or sulfasalazine before conception
- Sulfasalazine is the first choice for peripheral RA/SpA in pregnancy if tolerated
- Azathioprine is the first choice for immunosuppression in patients with lupus, vasculitis, or as a steroid-sparer
- Start high-dose folic acid (2–5 mg/day) in any patient on sulfasalazine
- Monitor CBC and LFTs regularly (both drugs) - unchanged from standard monitoring
- Monitor fetal growth with serial USS from 20 weeks onwards in patients on AZA
- Both drugs can be continued through all trimesters and during breastfeeding
Sources: Firestein & Kelley's Textbook of Rheumatology; Rheumatology (Elsevier 2022); Creasy & Resnik's Maternal-Fetal Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.