Neural regulation of respiration 5m answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete 5-mark answer on the neural regulation of respiration:
Neural Regulation of Respiration
1. The Respiratory Center
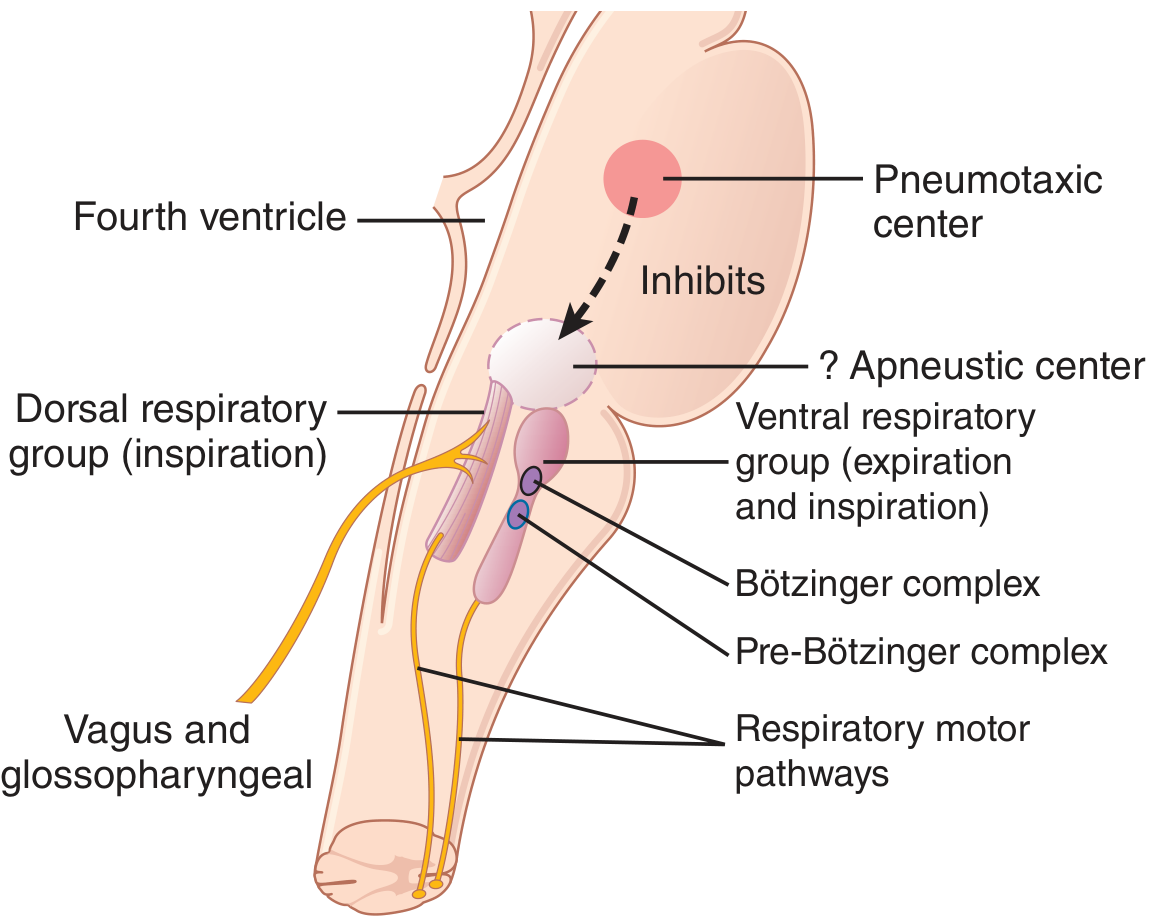
The respiratory center consists of bilateral groups of neurons in the medulla oblongata and pons of the brainstem. It is divided into three main collections:
- Dorsal Respiratory Group (DRG) - in the dorsal medulla (nucleus tractus solitarius); primarily drives inspiration
- Ventral Respiratory Group (VRG) - in the ventrolateral medulla; drives both inspiration and expiration (active during exercise)
- Pneumotaxic Center - in the upper pons (nucleus parabrachialis); controls the switch-off of inspiration
2. Generation of Respiratory Rhythm
The pre-Bötzinger complex (rostral VRG) contains pacemaker-like neurons that fire spontaneously and project to both the DRG and VRG. It functions as the central pattern generator for respiration - destruction of this region abolishes rhythmic breathing.
The DRG generates an inspiratory "ramp" signal: the neural output to the diaphragm starts weak, increases steadily over ~2 seconds (causing smooth lung inflation), then abruptly ceases for ~3 seconds (allowing passive elastic recoil = expiration). The cycle then repeats.
The Bötzinger complex (rostral to pre-Bötzinger) inhibits inspiration and helps switch to expiration.
3. The Pneumotaxic Center and Apneustic Center
- Pneumotaxic center (upper pons): Sends inhibitory signals to the DRG, cutting off the inspiratory ramp early. A strong signal = rate up to 30-40 breaths/min; a weak signal = rate as low as 3-5 breaths/min. Primary role is to limit tidal volume and increase respiratory rate.
- Apneustic center (lower pons): Tends to prolong inspiration. Normally kept in check by the pneumotaxic center. If the pneumotaxic center is destroyed and the vagus is cut, apneusis results - prolonged inspiratory gasps interrupted by brief expirations.
4. Chemical Control - Chemoreceptors
Central chemoreceptors (ventral surface of medulla):
- Respond to CSF pH (i.e., indirectly to arterial PCO2)
- CO2 crosses the blood-brain barrier freely → reacts with water in CSF → forms H⁺ → stimulates chemoreceptors → increases ventilation
- PCO2 is the dominant minute-to-minute controller of breathing
- Effect attenuates over 1-2 days as kidneys compensate by raising HCO3⁻
Peripheral chemoreceptors (carotid and aortic bodies):
- Carotid bodies (at bifurcation of common carotid arteries): afferents via CN IX (Hering's nerve) → DRG
- Aortic bodies (arch of aorta): afferents via CN X → DRG
- Respond to ↓ PaO2 (especially below 60 mmHg, on the steep part of the O2-Hb curve), ↑ PCO2, ↓ pH
- O2 has no direct effect on central respiratory neurons; it acts only peripherally
- In metabolic acidosis, carotid bodies (not aortic) mediate the compensatory hyperventilation
5. Reflex and Higher Center Inputs
Hering-Breuer inflation reflex: Stretch receptors in bronchial/bronchiolar walls send signals via the vagus to the DRG when the lungs are over-inflated, switching off the inspiratory ramp. In humans this activates mainly when tidal volume exceeds ~1.5 L - it is a protective reflex more than a normal ventilatory regulator.
Other receptors:
- Irritant receptors (airway epithelium): respond to dust/chemicals → reflex bronchoconstriction + increased breathing rate (via CN X)
- J (juxtacapillary) receptors (alveolar walls): activated by pulmonary capillary engorgement (e.g., left heart failure) → rapid shallow breathing and dyspnea
- Joint and muscle mechanoreceptors: anticipatory increase in ventilation at the start of exercise before blood gases change
Cerebral cortex: Can temporarily override brainstem centers (voluntary breath-holding, voluntary hyperventilation). Hyperventilation is self-limiting because the resulting ↓ PaCO2 eventually causes unconsciousness and reversion to automatic breathing.
Summary table:
| Component | Location | Function |
|---|---|---|
| DRG | Dorsal medulla | Inspiratory rhythm; receives sensory inputs |
| VRG / Pre-Bötzinger | Ventrolateral medulla | Rhythm generator; active expiration |
| Pneumotaxic center | Upper pons | Limits inspiration, increases rate |
| Apneustic center | Lower pons | Prolongs inspiration (normally inhibited) |
| Central chemoreceptors | Ventral medulla | Respond to CSF H⁺/PCO2 |
| Peripheral chemoreceptors | Carotid & aortic bodies | Respond to ↓ PO2, ↑ PCO2, ↓ pH |
(Sources: Guyton & Hall Textbook of Medical Physiology; Costanzo Physiology 7th Edition)
This is a shared conversation. Sign in to Orris to start your own chat.