AKI scoring systems in ER
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute kidney injury" AND "scoring system" AND "emergency department"
Reading File
Finding Sources
Searching PubMed
"acute kidney injury" AND "emergency department" AND "prediction"
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Searching the Web
AKI scoring systems emergency department RIFLE AKIN KDIGO comparison 2024 2025
Reading File
Reading File
I now have comprehensive data. Let me compile the full answer.
AKI Scoring Systems in the Emergency Department
Overview
Three major staging systems are used to define and classify AKI in clinical practice, including the ER: RIFLE, AKIN, and KDIGO. Each uses serum creatinine (sCr) and urine output (UO) as the two primary parameters.
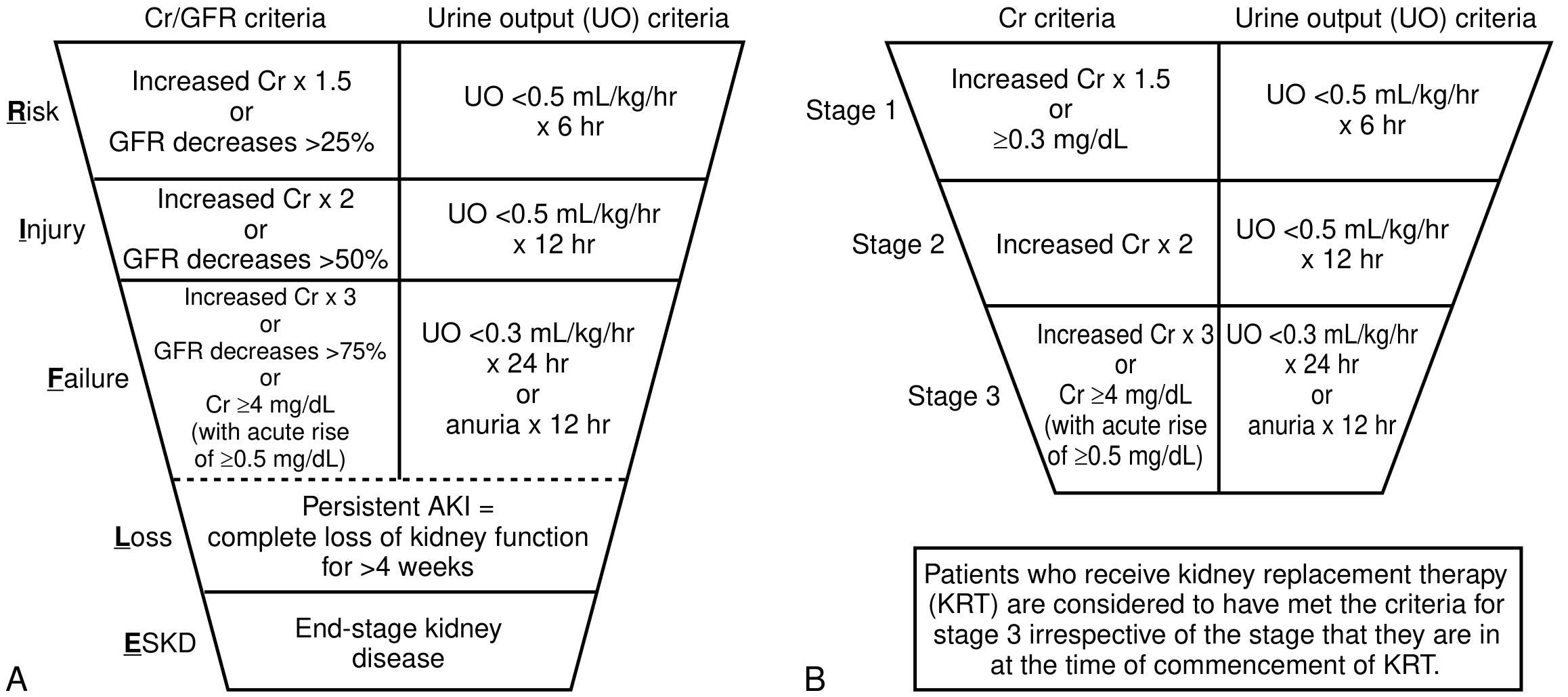
1. RIFLE Criteria (2004)
Developed by the Acute Dialysis Quality Initiative (ADQI)
| Stage | Serum Creatinine (sCr) | Urine Output |
|---|---|---|
| Risk | ↑ ×1.5 OR GFR ↓ >25% | <0.5 mL/kg/h for >6 h |
| Injury | ↑ ×2 OR GFR ↓ >50% | <0.5 mL/kg/h for >12 h |
| Failure | ↑ ×3 OR GFR ↓ >75% OR sCr ≥4 mg/dL (acute rise ≥0.5) | <0.3 mL/kg/h for >24 h or anuria >12 h |
| Loss | Complete loss of function >4 weeks | — |
| ESKD | End-stage kidney disease >3 months | — |
- Time frame: sCr change over <7 days
- Loss and ESKD are outcome stages, not severity stages
- National Kidney Foundation Primer on Kidney Diseases, 8e
2. AKIN Criteria (2007)
Developed by the Acute Kidney Injury Network
Simplified RIFLE into 3 stages and added an absolute sCr threshold for Stage 1:
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| Stage 1 | ↑ ≥0.3 mg/dL or ↑ ≥50% | <0.5 mL/kg/h for >6 h |
| Stage 2 | ↑ ×2 (≥100%) | <0.5 mL/kg/h for >12 h |
| Stage 3 | ↑ ×3 (≥200%) OR sCr ≥4 mg/dL (acute rise ≥0.5) OR initiation of RRT | <0.3 mL/kg/h for >24 h or anuria >12 h |
- Time frame for absolute sCr change: 48 hours
- Requires at least 2 sCr measurements ≤48 h apart
- Eliminates the Loss/ESKD categories
3. KDIGO Criteria (2012) — Current Standard
Developed by Kidney Disease: Improving Global Outcomes
Merges RIFLE and AKIN; now the most widely adopted system:
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| Stage 1 | ↑ ≥0.3 mg/dL within 48 h OR ↑ ≥1.5× baseline within 7 days | <0.5 mL/kg/h for >6 h |
| Stage 2 | ↑ ≥2× baseline | <0.5 mL/kg/h for >12 h |
| Stage 3 | ↑ ≥3× baseline OR sCr ≥4 mg/dL OR initiation of RRT | <0.3 mL/kg/h for >24 h or anuria >12 h |
Patients receiving kidney replacement therapy (KRT) are automatically classified as Stage 3 regardless of sCr level.
The KDIGO definition requires two sCr values: an index value and a baseline. When no baseline is available, KDIGO recommends back-calculating using the MDRD formula assuming eGFR of 75 mL/min/1.73 m².
Comparison Table
| Feature | RIFLE | AKIN | KDIGO |
|---|---|---|---|
| Year | 2004 | 2007 | 2012 |
| sCr time frame | 7 days | 48 h (absolute) | Both (48 h + 7 days) |
| Absolute sCr threshold | No | ≥0.3 mg/dL | ≥0.3 mg/dL |
| Stages | 5 (3 severity + 2 outcome) | 3 | 3 |
| RRT auto-Stage 3 | No | Yes | Yes |
| Outcome categories | Loss, ESKD | — | — |
- Brenner and Rector's The Kidney, 2-Volume Set
ER-Specific Considerations
Baseline creatinine
The ER frequently lacks prior sCr. Options:
- Use previous values if in the electronic record
- Back-calculate using MDRD (eGFR assumed 75 mL/min/1.73 m²) per KDIGO/ADQI guidance
- Use the lowest recent sCr within 3–12 months as the baseline
Urine output in the ER
Oliguria criteria require time-based monitoring. In the ED, accurate UO assessment requires a Foley catheter. Without one, the UO criterion is often impractical, making sCr the primary tool in most emergency presentations.
KDIGO and UO together
Studies adding the UO criterion to sCr reveal AKI incidence as high as 80% in ICU patients — most are Stage 1 and have higher recovery rates. However, patients meeting both sCr AND UO criteria have significantly worse outcomes.
Functional Tests and Biomarkers (Emerging Tools)
| Biomarker | Mechanism | Clinical Value |
|---|---|---|
| NGAL (urine/plasma) | Tubular damage | Early AKI detection before sCr rises |
| Cystatin C | Glomerular filtration | sCr alternative, less influenced by muscle mass |
| TIMP-2 × IGFBP7 (NephroCheck) | Tubular cell cycle arrest | Detects Stage 2–3 AKI within 12 h |
| KIM-1 | Proximal tubular damage | High specificity; cutoff >2.0 |
| Furosemide Stress Test | Tubular functional reserve | Predicts AKI progression |
- Current Surgical Therapy 14e
Limitations Relevant to the ER
- sCr is not an immediate marker — rises 24–48 h after the kidney insult; early AKI may be missed
- Creatinine is affected by non-renal factors: muscle mass, age, sex, medications (e.g., trimethoprim, cimetidine block tubular secretion and raise sCr without true GFR change)
- No single system is superior for mortality prediction — RIFLE, AKIN, and KDIGO perform comparably for in-hospital mortality (AUC-ROC ~0.65–0.67 in sepsis cohorts)
- KDIGO is preferred for its combined 48-h and 7-day windows, accommodating different ER presentation timelines
Sources: National Kidneys Foundation Primer on Kidney Diseases 8e; Brenner and Rector's The Kidney; Current Surgical Therapy 14e; Sabiston Textbook of Surgery 14e; Tietz Textbook of Laboratory Medicine 7e
This is a shared conversation. Sign in to Orris to start your own chat.