Methylcobala min
Reading File
Searching the Web
methylcobalamin pharmacology clinical uses 2025
Finding Sources
Searching PubMed
methylcobalamin neuropathy clinical trial
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a detailed, textbook-grounded overview of methylcobalamin:
Methylcobalamin
Structure
Methylcobalamin (CH3-B12) is one of the two physiologically active coenzyme forms of vitamin B12. Its structure centers on a corrin ring with cobalt (Co) held at the center. The key difference from cyanocobalamin (the pharmaceutical/supplement form) is the substituent attached to cobalt: a methyl group (-CH3) replaces the cyanide (-CN) group. The other active coenzyme form, 5'-deoxyadenosylcobalamin, carries a deoxyadenosine group instead.
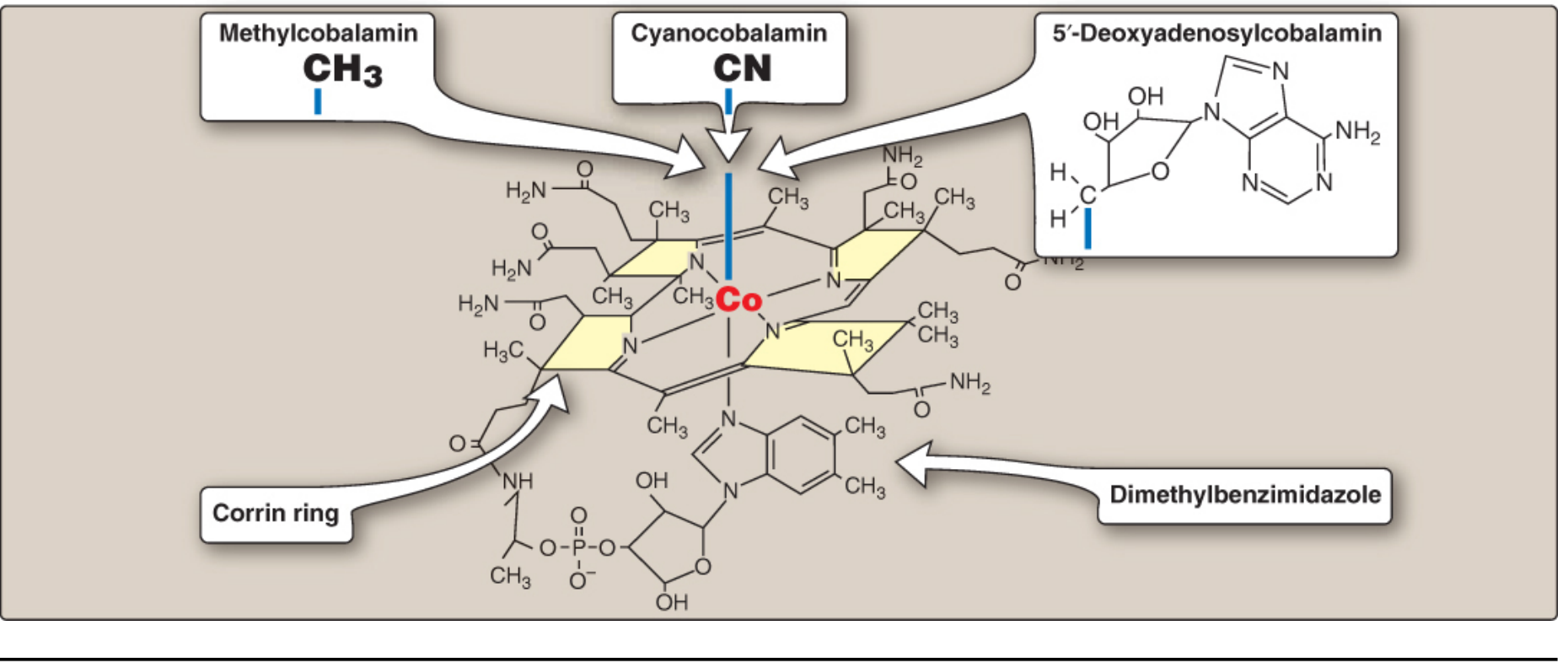
Structure of cobalamin forms - Lippincott's Biochemistry, 8th ed.
Biochemical Roles
Methylcobalamin has one primary enzymatic role:
1. Methionine Synthase Reaction (Methyl Transfer)
Methylcobalamin serves as a cofactor for methionine synthase, the enzyme that converts homocysteine to methionine. The methyl group is donated by N5-methyltetrahydrofolate (CH3-THF), which passes it to cobalamin forming methylcobalamin, which then transfers it to homocysteine to produce methionine.
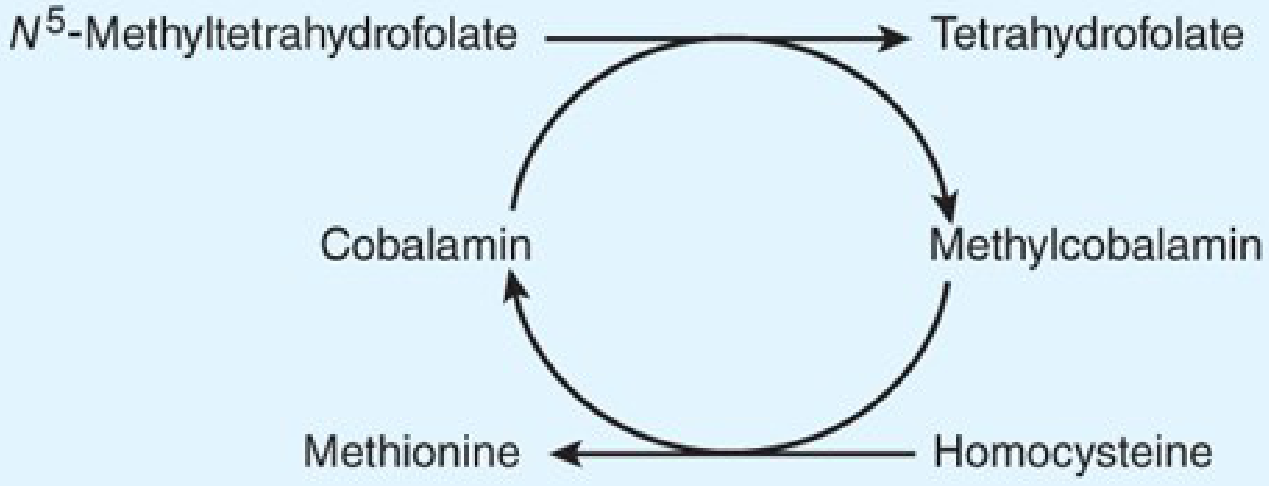
Methyl transfer cycle - Katzung's Basic & Clinical Pharmacology, 16th ed.
This reaction is critical because:
- It regenerates tetrahydrofolate (THF) from the trapped N5-methyl form
- It produces methionine and subsequently S-adenosylmethionine (SAM), the universal methyl donor for numerous methylation reactions
- It links folate metabolism to B12 metabolism (the "folate trap" mechanism)
2. Folate Trap (Consequences of Deficiency)
When methylcobalamin is deficient, N5-methyl-THF cannot be demethylated. Folate becomes "trapped" in this unusable form, starving cells of the THF derivatives (N5,N10-methylene-THF, N10-formyl-THF) needed for purine and thymidylate synthesis. This impairs DNA replication in rapidly dividing cells - most notably erythroid precursors in bone marrow and intestinal epithelium - causing megaloblastic anemia.
"The methionine synthetase reaction is largely responsible for the control of the recycling of folate cofactors... and through the synthesis of methionine and its product S-adenosylmethionine (SAM), the maintenance of a number of methylation reactions." - Goodman & Gilman's, 13th ed.
Methylcobalamin vs. Adenosylcobalamin
| Feature | Methylcobalamin | 5'-Deoxyadenosylcobalamin |
|---|---|---|
| Location | Cytoplasm | Mitochondria |
| Enzyme | Methionine synthase | Methylmalonyl-CoA mutase |
| Reaction | Homocysteine → Methionine | L-methylmalonyl-CoA → Succinyl-CoA |
| Deficiency marker | Elevated homocysteine | Elevated methylmalonic acid (MMA) |
| Clinical relevance | Megaloblastic anemia, neuropathy | Organic acidemia (methylmalonic aciduria) |
Methylcobalamin vs. Cyanocobalamin
| Methylcobalamin | Cyanocobalamin | |
|---|---|---|
| Naturally occurring | Yes (in food, plasma, CSF) | No (synthetic) |
| Active form | Yes - directly usable | No - requires hepatic conversion |
| CNS penetration | Better | Limited |
| Storage | Lower | More stable, longer shelf life |
| Conversion needed | None | Must be converted to methyl- or adenosyl-cobalamin |
| Preferred in | Neurological disease, malabsorption | Broad supplementation, fortified foods |
Clinical Uses
- Vitamin B12 deficiency - pernicious anemia, vegans, malabsorption states (gastric resection, Crohn's, metformin use)
- Peripheral neuropathy - particularly diabetic peripheral neuropathy; commonly used in Asia (orally or IM)
- Elevated homocysteine - hyperhomocysteinemia, reducing cardiovascular risk markers
- Subacute combined degeneration of the spinal cord - demyelination of posterior and lateral columns due to B12 deficiency
- Neuropathic pain - emerging use; reduces hyperpolarization-activated ion channel activity
Deficiency: Neurological Mechanism
The neurological complications of B12 deficiency (subacute combined degeneration) are thought to result from disruption of the methionine synthesis pathway rather than methylmalonyl-CoA accumulation. Disrupted SAM production impairs myelin synthesis and maintenance. Branched-chain fatty acids (from abnormal methylmalonyl-CoA metabolism via the adenosylcobalamin pathway) may also incorporate into CNS cell membranes, contributing to neurological damage.
"Folic acid in the setting of vitamin B12 deficiency will not prevent neurologic manifestations even though it will largely correct the anemia." - Katzung's Basic & Clinical Pharmacology, 16th ed.
This is a clinically important point: treating with folate alone can mask the anemia while neurological damage progresses silently.
Dosing & Administration
- Dietary requirement (RDA): 2.4 mcg/day
- Body stores: 2-5 mg (mostly in liver); deficiency symptoms may take 3-5 years to emerge after cessation of intake
- Oral supplementation: 500-1,500 mcg/day (high-dose oral can bypass intrinsic factor deficiency via passive diffusion)
- Intramuscular: 100-1,000 mcg/day to weekly; preferred in pernicious anemia and severe deficiency
- Pernicious anemia maintenance: 100 mcg IM every 4 weeks for life
Recent Evidence
A 2025 systematic review and meta-analysis (PMID: 40612436) examined dapagliflozin combined with methylcobalamin for type 2 diabetes with peripheral neuropathy, finding the combination beneficial for neuropathy outcomes. A 2024 meta-analysis (PMID: 38330524) of disease-modifying therapies for diabetic peripheral neuropathy supports methylcobalamin as one of the more evidence-backed agents for this indication.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic & Clinical Pharmacology, 16th ed.; Lippincott's Illustrated Reviews: Biochemistry, 8th ed.; Tietz Textbook of Laboratory Medicine, 7th ed.
Dynapar qps
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Viveramn
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Doli 650
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.