12. Define evidence-based medicine and explain the approach and practice of evidence-based medicine in clinical settings.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Evidence-Based Medicine (EBM): Definition, Approach, and Clinical Practice
1. Definition
Evidence-based medicine (EBM) is a systematic practice that integrates the most current and best available research evidence with clinical expertise and individual patient values and preferences when making medical decisions.
The most widely cited definition, formulated by Sackett and colleagues (2000) and echoed across major textbooks, is:
"EBM is a process by which medical decisions can be made by using as many objective tools as possible... It integrates the most current and best evidence with clinical expertise and patient preferences when making medical decisions."
- Henry's Clinical Diagnosis and Management by Laboratory Methods
Harrison's Principles of Internal Medicine (22nd ed.) frames EBM as an update to traditional clinical medicine:
"Clinical medicine is defined traditionally as a practice combining medical knowledge (including scientific evidence), intuition, and judgment in the care of patients. EBM updates this construct by placing much greater emphasis on the processes by which clinicians gain knowledge of the most up-to-date and relevant clinical research."
Historical origin: The term and formal program were introduced in the early 1990s by a group at McMaster University, published in JAMA (1992) by the Evidence-Based Medicine Working Group. It emerged in response to heavy reliance on clinical experience, expert opinion, and anecdote in medical decision-making - approaches recognized as subjective and potentially biased.
2. The Three Pillars of EBM
EBM rests on the integration of three elements:
| Pillar | Meaning |
|---|---|
| Best available research evidence | Current, valid, and relevant findings from the literature |
| Clinical expertise | The clinician's experience, judgment, and skill |
| Patient values and preferences | Individual goals, concerns, and expectations |
None of these elements alone is sufficient. It is the blend of evidence and clinical intuition that makes EBM both attractive and essential to modern practice. (Creasy & Resnik's Maternal-Fetal Medicine)
3. The EBM Process: Steps in Clinical Practice
3.1 The Classic Four-Step Model (McMaster, early 1990s)
As described in Harrison's Principles of Internal Medicine, the founding proponents at McMaster University outlined four key steps:
- Formulating the management question to be answered
- Searching the literature and online databases for applicable research data
- Appraising the evidence gathered with regard to its validity and relevance
- Integrating this appraisal with knowledge about the unique aspects of the patient (including the patient's preferences about possible outcomes)
3.2 The Five-Step Model (Sackett / Henry's)
A widely practiced expanded version (Henry's Clinical Diagnosis and Management by Laboratory Methods) uses five steps:
- Ask - Formulate a focused clinical question based on a patient encounter
- Acquire - Search information resources (journals, electronic databases, textbooks)
- Appraise - Critically evaluate the information; reach a conclusion that answers the question
- Apply - Apply the information to the individual patient
- Audit - Monitor effectiveness and audit outcomes
3.3 The "A5" Cycle (Tietz / Evidence-Based Laboratory Medicine)
The Tietz Textbook of Laboratory Medicine (7th ed.) describes this as a continuous cycle beginning with identifying a clinical problem:
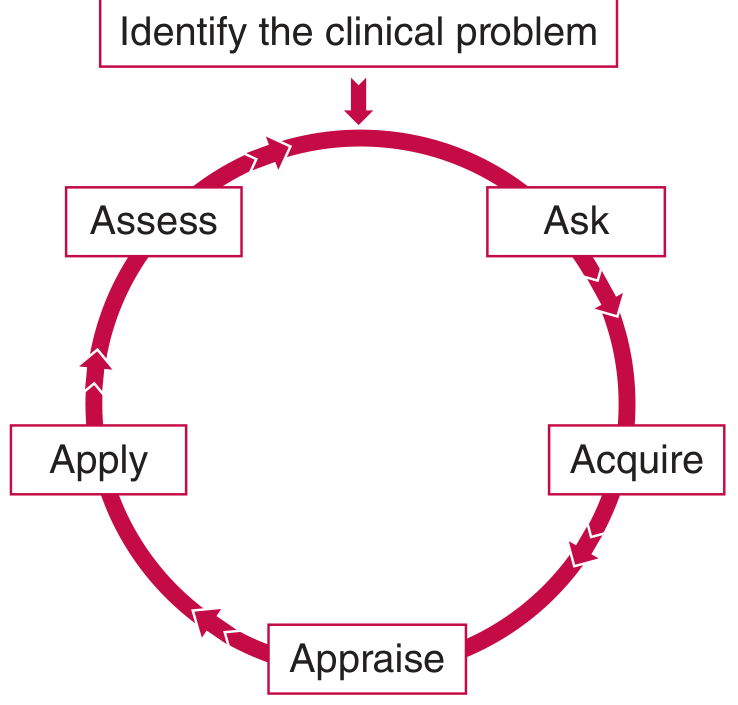
The "A5" evidence-based laboratory medicine cycle (Tietz Textbook of Laboratory Medicine, 7th Edition)
The steps are:
- Identify the clinical problem
- Ask / formulate the question to help solve the problem
- Acquire the evidence that addresses the question
- Appraise the evidence
- Apply the knowledge gained in resolving the problem
- Audit (assess) the application of the evidence
4. Formulating the Clinical Question: PICO
A structured and answerable clinical question is the foundation of EBM. The PICO framework provides a standardized format:
| Letter | Stands For | Meaning |
|---|---|---|
| P | Problem/Patient | What is the specific problem or patient population? |
| I | Intervention | What test, treatment, or exposure is being considered? |
| C | Comparison | What is the alternative or comparator? |
| O | Outcome | What is the relevant, quantifiable clinical outcome? |
Example (Henry's Clinical Diagnosis):
- P: 58-year-old man with hepatocellular carcinoma after liver resection
- I: Serum AFP measured after resection
- C: Serum AFP not measured
- O: Predictive value for HCC recurrence and survival
The PICO question must be formulated before searching resources to prevent selection bias.
5. Sources of Evidence
Information sources include:
- Primary literature: Original research articles, especially randomized controlled trials (RCTs)
- Secondary literature: Systematic reviews, meta-analyses
- Electronic databases: MEDLINE/PubMed, Cochrane Database, EMBASE
- Clinical practice guidelines (CPGs): Evidence-based recommendations from professional societies
- Textbooks: Useful for background knowledge, though may be outdated at time of publication
The strategy for search must be determined before searching to avoid selection bias. Journal articles reporting results of double-blinded RCTs are the most valuable because they are least biased, though still highly dependent on the methods used. (Henry's Clinical Diagnosis and Management)
6. Hierarchy (Levels) of Evidence
The concept of an evidence hierarchy ranks study types by their likelihood of producing accurate and unbiased results. The Oxford Centre for Evidence-Based Medicine (CEBM) 2011 system is among the most widely used.
Oxford CEBM Levels (for Therapeutic Questions):
| Level | Study Type |
|---|---|
| Level I | Systematic review of RCTs; Individual RCT with narrow confidence interval |
| Level II | Systematic review of cohort studies; Prospective cohort study; Observational study with dramatic effect |
| Level III | Systematic review of case-control studies; Retrospective cohort study; Case-control study |
| Level IV | Case series; Historically controlled study |
| Level V | Mechanism-based reasoning (expert opinion, bench research) |
(Rockwood and Green's Fractures in Adults, 10th ed.; Schwartz's Principles of Surgery, 11th ed.)
Key principle: A study may be downgraded based on poor quality, imprecision, indirectness, or inconsistency. An observational study with a very large treatment effect may outrank a poorly conducted RCT. The hierarchy represents the likely best evidence, not an absolute ranking.
GRADE Evidence Quality System (Schwartz's):
| Grade | Meaning |
|---|---|
| High | Further research is very unlikely to change confidence in the estimate of effect |
| Moderate | Further research is likely to have an important impact and may change the estimate |
| Low | Further research is very likely to change the estimate |
| Very Low | Any estimate of effect is very uncertain |
7. Systematic Reviews and Clinical Practice Guidelines
Because individual clinicians cannot keep pace with the rapidly expanding literature (estimated >1,000 articles added to MEDLINE per day - Creasy & Resnik), EBM in practice relies on:
Systematic Reviews (SRs)
- Identify, select, assess, and synthesize findings of relevant literature
- Use predefined, reproducible search strategies with explicit inclusion/exclusion criteria
- Aim to avoid biases inherent in narrative reviews
- Prototype resource: Cochrane Database of Systematic Reviews
- May include meta-analysis - a quantitative pooling of results from multiple studies
Limitations of SRs (Harrison's): They are not uniformly the pinnacle of EBM. Value is reduced when: only a few trials are available; trials and observational studies are mixed; or the evidence base is only observational. They cannot compensate for deficiencies in underlying research.
Clinical Practice Guidelines (CPGs)
Professional societies translate evidence into clinical recommendations. The flowchart below illustrates how SRs and CPGs interact to produce EBM in practice:
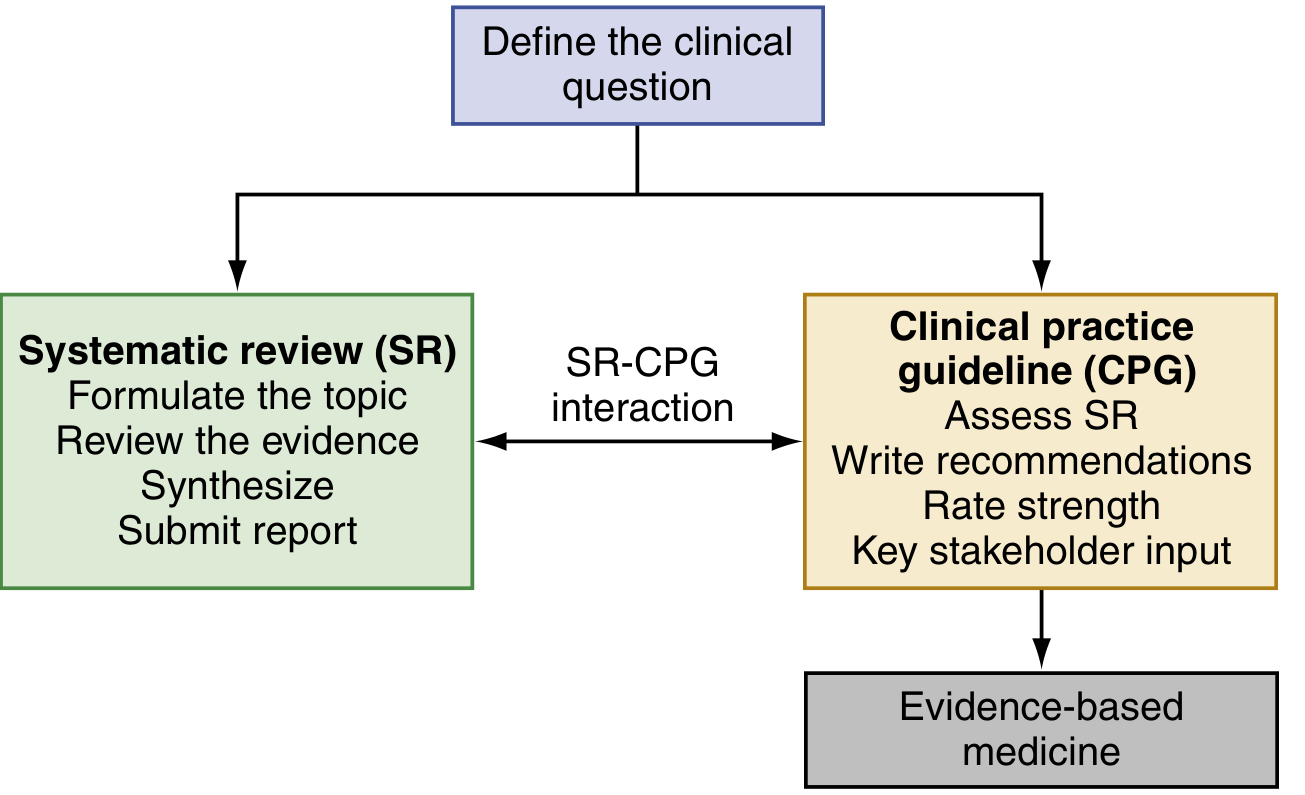
Flowchart: The development of systematic reviews (SRs) informs the group developing clinical practice guidelines (CPGs), leading to evidence-based medicine. (Henry's Clinical Diagnosis and Management)
Quality issues with CPGs: CPG quality can be affected by:
- Quality of SRs used to inform them
- Unmanaged conflicts of interest
- Failure to use rigorous methodologies
The Institute of Medicine (IOM) has created standards addressing group structure, transparent process, scientific rigor, and reporting of SRs and CPGs. (Henry's)
8. Sources of Evidence: Clinical Trials and Registries
Harrison's notes that the two major tools for developing reliable evidence are:
-
Randomized Clinical Trials (RCTs) - the gold standard for measuring benefits of interventions. New adaptive trial designs, pragmatic trials, and real-world evidence methods are evolving the classical RCT model.
-
High-quality observational registries - focused on diseases or syndromes, supplementing RCT data with real-world populations.
Lesson from COVID-19: Despite >40,000 publications appearing in the first 7 months of the pandemic, enormous uncertainty remained because most were small observational series or reviews - reinforcing that small observational studies have no role in formulating modern standards of practice. (Harrison's, 22nd ed.)
9. Importance of EBM in Clinical Settings
Why EBM matters (from Creasy & Resnik's Maternal-Fetal Medicine):
-
Best patient care: EBM prevents premature adoption of unproven interventions. Classic example: electronic fetal heart rate monitoring was widely implemented before evidence of benefit - it became a major driver of cesarean delivery without proven superiority over intermittent auscultation in low-risk patients.
-
Information management: With thousands of articles published daily, EBM tools allow clinicians to efficiently assess relevant, high-quality literature.
-
Tackling emerging challenges: EBM provided the framework to rapidly evaluate COVID-19 interventions through cohort studies and clinical trials.
-
Answering unanswered questions: EBM methodology guides research to resolve outstanding clinical dilemmas.
10. Barriers and Limitations in Practice
- Time: Searching, appraising, and synthesizing evidence in a busy clinical setting is logistically challenging (Harrison's). This has driven reliance on pre-appraised summaries (SRs, guidelines).
- Skills: Most clinicians lack formal training in critical appraisal.
- Evidence gaps: For many clinical questions, high-quality evidence does not yet exist.
- Generalizability: Trial populations may not match the individual patient ("internal vs. external validity").
- Variable quality: The medical literature is "flooded with systematic reviews of varying quality and clinical utility" - peer review has not proved to be an effective arbiter (Harrison's).
- Conflicting guidelines: The same body of evidence can produce different recommendations depending on the rating system used (e.g., AAOS vs. ACCP on VTE prophylaxis - Schwartz's Surgery).
Summary
| Aspect | Key Point |
|---|---|
| Definition | Integration of best research evidence + clinical expertise + patient values |
| Origin | McMaster University, early 1990s |
| Core steps | Ask (PICO) → Acquire → Appraise → Apply → Audit |
| Question format | PICO framework |
| Highest quality evidence | Systematic reviews of RCTs; individual high-quality RCTs |
| Practical shortcut | Systematic reviews and clinical practice guidelines |
| Key tool | Cochrane Database, PubMed/MEDLINE, GRADE system |
| Fundamental goal | Reduce uncertainty in medical decision-making through objective, reproducible, patient-centered methods |
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025, McGraw Hill)
- Henry's Clinical Diagnosis and Management by Laboratory Methods (Elsevier)
- Tietz Textbook of Laboratory Medicine, 7th ed.
- Creasy & Resnik's Maternal-Fetal Medicine (Elsevier)
- Rockwood and Green's Fractures in Adults, 10th ed. (2025)
- Schwartz's Principles of Surgery, 11th ed.
- Goldman-Cecil Medicine, International Edition
This is a shared conversation. Sign in to Orris to start your own chat.