Iontophorosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Now I have comprehensive information. Let me compose a thorough answer.
Iontophoresis
Definition & Mechanism
Iontophoresis is a technique in which direct electrical current (DC) is used to transport ionically charged drug molecules across the skin and mucous membranes without needles. The principle relies on electrostatic repulsion: a charged drug ion placed under an electrode of the same polarity is driven away from that electrode and into the tissue.
- Positively charged drugs → placed under the anode (+)
- Negatively charged drugs → placed under the cathode (−)
- Drug penetration depth: 0.2–1.5 cm, depending on the agent and local tissue characteristics
- Drug delivery rate is proportional to applied current, enabling programmable delivery — especially important with miniaturized microprocessor-based systems
(Dermatology 2-Volume Set 5e; Pfenninger and Fowler's Procedures for Primary Care)
Physics of Drug Delivery
Three processes drive transdermal ion movement:
- Electrophoresis — direct migration of charged ions under an electric field (primary mechanism)
- Electroosmosis — bulk flow of water (and dissolved solutes) toward the cathode
- Electroporation (at higher voltages) — structural rearrangement of stratum corneum lipids creating pores (a separate but related technique)
Clinical Applications
1. Musculoskeletal / Anti-inflammatory
The most common clinical use is delivery of anti-inflammatory and analgesic agents to superficial musculoskeletal structures:
| Ion / Drug | Polarity | Indication | Dose |
|---|---|---|---|
| Dexamethasone | Negative (−) | Tendinitis, tenosynovitis, bursitis, arthritis | 1–4 mA × 15–20 min |
| Methylprednisolone | Negative (−) | Postherpetic neuralgia | 1–4 mA × 15–20 min |
| Acetic acid | Negative (−) | Calcified tendinitis, calcium deposits | 3–4 mA × 10–20 min |
| Salicylate | Negative (−) | Analgesia, myalgia, plantar warts | 4 mA × 45 min |
| Iodine | Negative (−) | Fibrosis, scar tissue, trigger finger | 2 mA × 1 min → 4 mA × 5 min |
| Chloride/sodium | Negative (−) | Keloids, scar tissue | 4 mA × 20–45 min |
| Lidocaine 4% | Positive (+) | Skin anesthesia | 4 mA × 20–30 min |
| Hyaluronidase | Positive (+) | Edema, lymphedema, scleroderma | 1–2 mA × 20–40 min |
| Copper sulfate | Positive (+) | Fungal infection | 4 mA × 20–30 min |
| Zinc | Positive (+) | Wound healing, ulcers | 4 mA × 15 min |
(Pfenninger and Fowler's Procedures for Primary Care)
2. Topical Anesthesia
Lidocaine with epinephrine delivered via iontophoresis provides adequate cutaneous anesthesia before venipuncture — particularly in pediatric patients — and is superior to EMLA for this purpose. Used before dermatologic procedures and IV insertion. (Roberts and Hedges' Clinical Procedures in Emergency Medicine)
3. Hyperhidrosis
In palmoplantar hyperhidrosis, tap or deionized water iontophoresis is an established treatment. The affected area is submerged in water; DC passes through at 8–20 mA for 10–20 minutes, 3–4 times weekly. The mechanism is incompletely understood but hypotheses include:
- Obstruction of eccrine ducts at the stratum corneum level
- Inhibition of sympathetic nerve transmission
- Local pH alterations affecting sweat gland function
Adding glycopyrrolate to the water trays enhances efficacy. Home devices (e.g., Drionic®) are available. Works best on palms and soles; less effective for axillary hyperhidrosis.
(Fitzpatrick's Dermatology; Dermatology 2-Volume Set 5e)
4. Sweat Chloride Testing (Cystic Fibrosis Diagnosis)
Iontophoresis of pilocarpine nitrate is the first step of the quantitative pilocarpine iontophoresis sweat test (Gibson-Cooke method). Pilocarpine stimulates localized sweat gland secretion; the collected sweat is analyzed for chloride concentration — the gold standard for CF diagnosis. (Tietz Textbook of Laboratory Medicine)
5. Other Applications (Emerging/Investigational)
- Fentanyl — patient-controlled transdermal pain relief
- Sumatriptan — migraine relief
- Reverse iontophoresis — extraction of glucose from skin for non-invasive glucose monitoring in diabetic patients
- Chemotherapeutic delivery into superficial skin tumors (combined with electroporation)
Equipment & Technique
Equipment needed:
- DC generator with constant current output (calibrated in mA)
- Active electrode (drug reservoir) and dispersive/return electrode
- Appropriate medication
Technique (summary):
- Inspect skin; clip (do not shave) hair; clean with 70% isopropyl alcohol
- Fill active electrode reservoir with medication per manufacturer specs
- Apply active electrode over treatment area, dispersive electrode at a remote site
- Set current 0.1–4 mA; gradually increase to patient tolerance (tingling sensation)
- Treat for 10–20 minutes; monitor every 2–4 minutes
- Electrical dose = intensity (mA) × duration (min) = mA·min
Wearable battery-powered patches are also available, delivering 0.06–0.45 mA continuously over 3–24 hours with auto-shutoff. (Pfenninger and Fowler's)
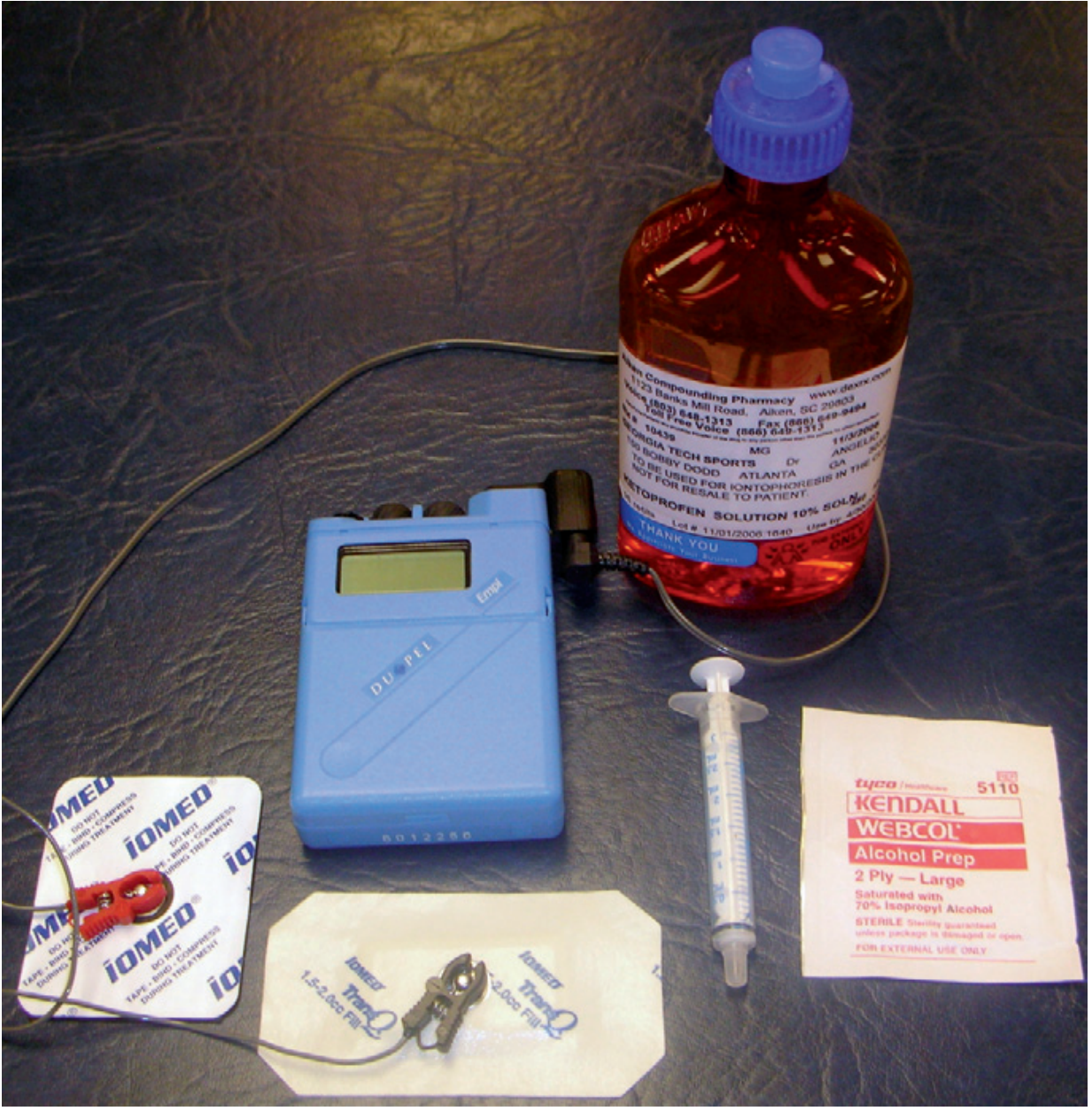
Iontophoresis current generator with iontophoresis agent, measuring syringe, alcohol wipe for skin preparation, electrodes, and electrode leads.
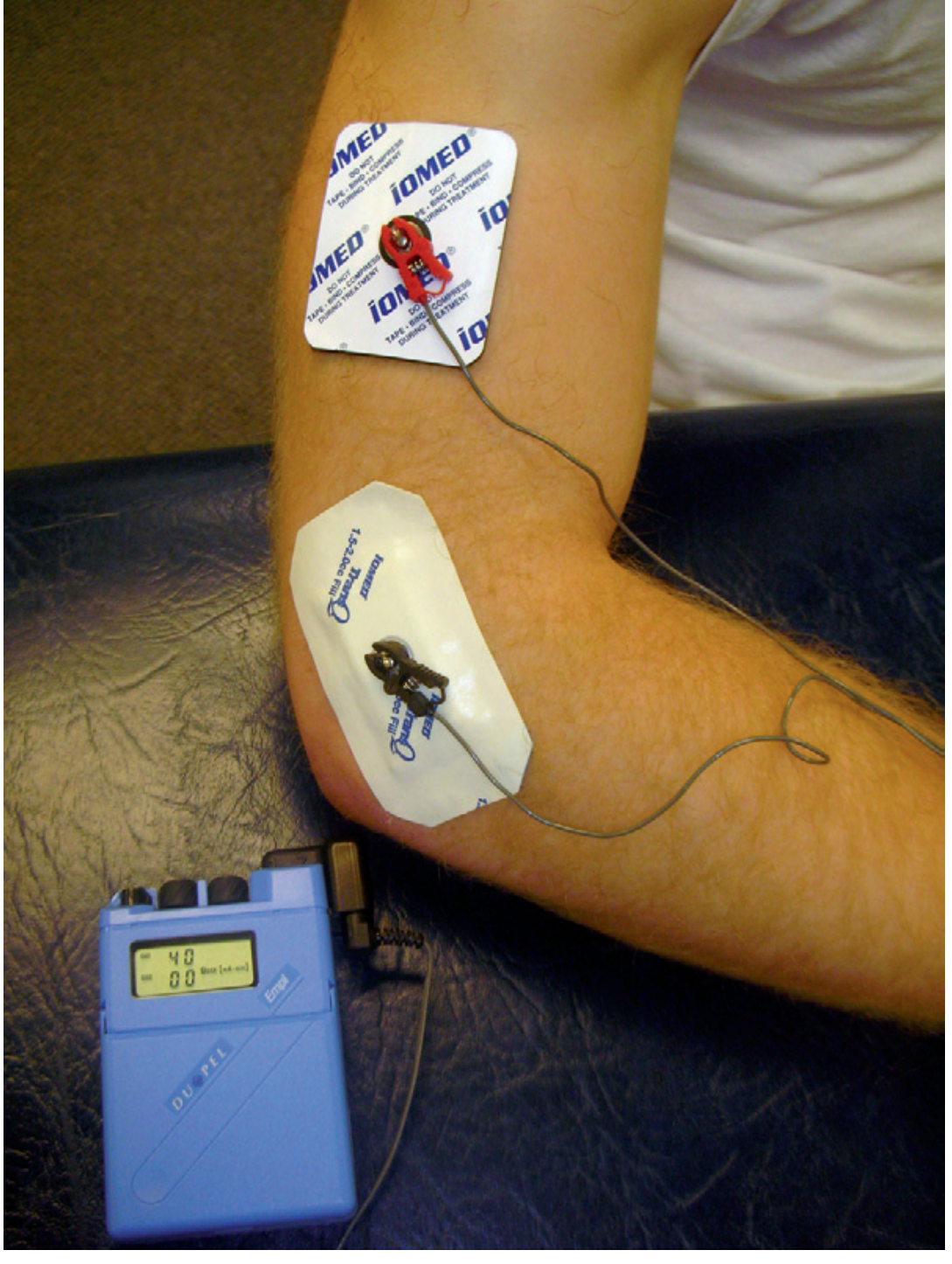
Iontophoresis treatment in progress.
Contraindications
| Category | Specific Contraindication |
|---|---|
| Systemic | Pacemakers or implanted cardiac devices |
| Drug-related | Known allergy/sensitivity to the therapeutic agent |
| Skin / Local | Superficial abrasions, cuts, bruises; recent bleeding; recent scars or skin grafts |
| Anatomical | Over the heart; over the carotid sinus; over metallic implants (screws, staples, wires) |
| Sensory | Areas of abnormal or absent sensation (patient must provide feedback to set current correctly) |
Complications
| Complication | Description |
|---|---|
| Galvanic rash | Hypersensitivity to DC; appears within 5 min of initiating stimulation |
| Electrode (cathode) burn | Alkaline reaction under the negative electrode; decreased skin resistance allows excess current; newer buffered electrodes reduce this |
| Twitch response | Inadvertent nerve stimulation from inappropriate current level |
| Post-treatment erythema | Common; from skin pH changes or local histamine release |
| Drug allergy | Previously unknown sensitivity to the iontophoresed agent |
| Irritation / blisters | Particularly with hyperhidrosis treatment at higher currents |
| Burns | Rare; risk with pilocarpine iontophoresis sweat testing |
Key Points
- Works best when the pathologic process is superficial and localized
- Dexamethasone is the primary agent for inflammation; lidocaine for topical anesthesia
- The drug must be ionizable in solution and placed under the electrode of the same charge
- Maximum penetration is ~1.5 cm — a practical limit for selecting appropriate indications
- Iontophoresis is CPT-coded (97033, each 15-minute application) and reimbursable in primary care settings
This is a shared conversation. Sign in to Orris to start your own chat.