Asthma pdf given
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have very comprehensive content. Let me compile the complete asthma notes.
🫁 Asthma - Comprehensive Notes
Source: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume
1. Definition
Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. Per the 2019 GINA guidelines:
"Asthma is defined by the history of respiratory symptoms such as wheeze, shortness of breath, chest tightness, and cough that vary over time and in intensity, together with variable expiratory airflow limitation."
No single feature is unique to asthma - it encompasses many phenotypes with variable responses to therapy.
2. Epidemiology
- Affects 4-8% of the general population
- Most common pulmonary disorder in pregnancy (3.7-8.4% of pregnancies)
- Often presents first in childhood; can arise at any age
- Risk factors for childhood onset: family history of asthma, personal/family history of atopy (atopic dermatitis, allergic rhinitis, conjunctivitis)
3. Pathophysiology
Asthma involves three overlapping mechanisms:
A. Airway Inflammation
- Eosinophilic inflammation - the classic Type 2 pathway, driven by IL-4, IL-13, and IL-5
- Non-eosinophilic (non-Type 2) inflammation - neutrophilic or paucigranulocytic; less responsive to corticosteroids
- Approximately 30-50% of asthmatics have non-eosinophilic inflammation with decreased response to ICS
B. Airway Hyperresponsiveness (AHR)
- Exaggerated bronchoconstriction response to stimuli (methacholine, exercise, cold air, allergens)
- Measured by PC20 (provocative concentration causing 20% fall in FEV1)
C. Airway Remodeling
- Structural changes from chronic inflammation: subepithelial fibrosis, smooth muscle hypertrophy/hyperplasia, goblet cell metaplasia, mucus hypersecretion
- Airway smooth muscle plays a major role - bronchial thermoplasty targets this
4. Clinical Features
Symptoms
- Wheeze (expiratory > inspiratory)
- Shortness of breath
- Chest tightness
- Cough (especially nocturnal or with exercise)
- Symptoms vary over time and in intensity - this variability is a hallmark
Triggers
- Allergens (dust mites, pollen, animal dander)
- Respiratory infections (viral URTIs)
- Exercise and cold air
- Aspirin/NSAIDs (aspirin-exacerbated respiratory disease)
- Chemical exposures (occupational asthma)
- Gastroesophageal reflux, stress, obesity
Physical Examination
- May be normal between attacks
- During attack: expiratory wheeze on auscultation, prolonged expiration, use of accessory muscles
- Silent chest = very severe obstruction (ominous sign)
5. Diagnosis
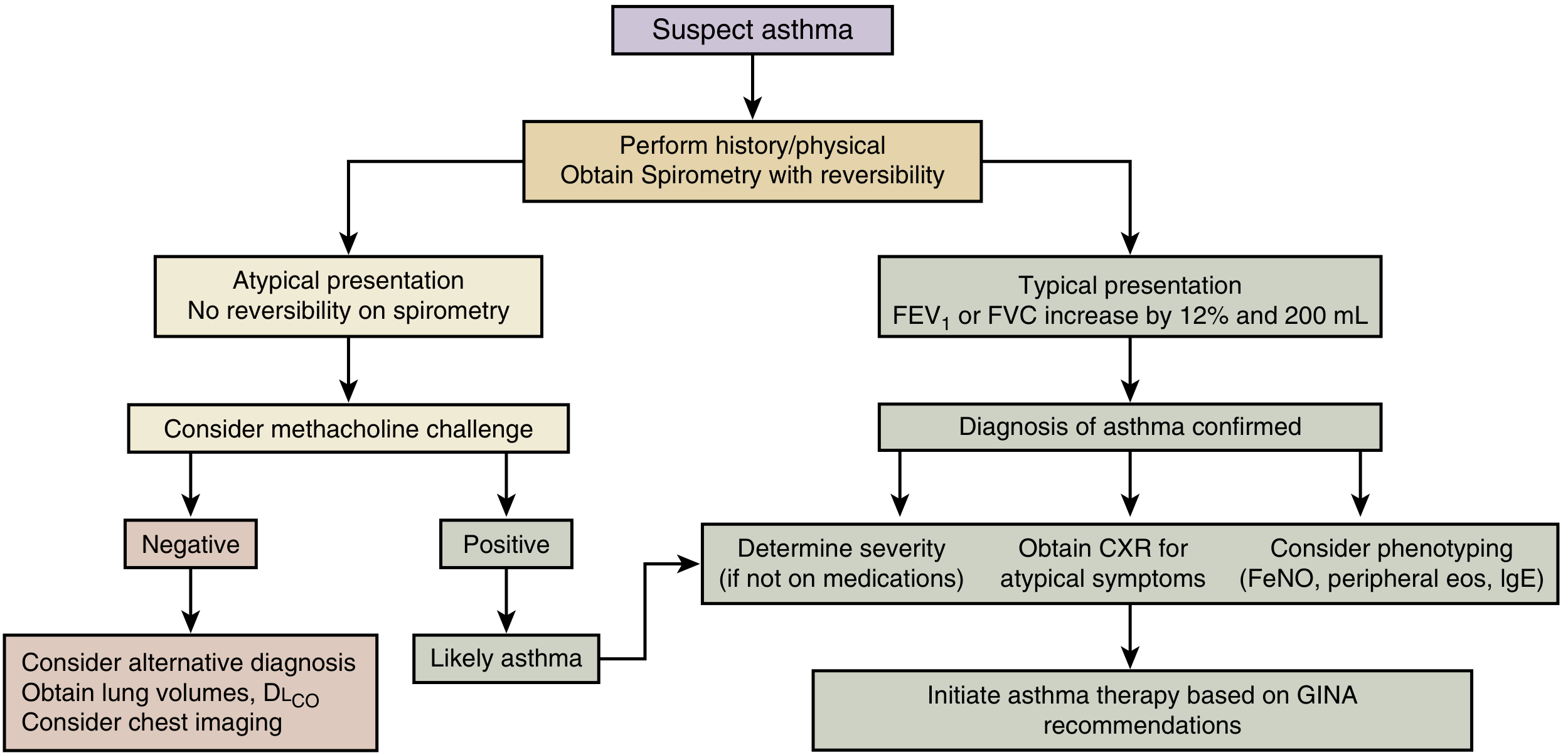
Step-by-step approach:
Step 1: History + Physical + Spirometry with reversibility
Step 2: Typical presentation?
- Bronchodilator reversibility = FEV1 or FVC increases by ≥12% AND ≥200 mL post-bronchodilator → Diagnosis confirmed
Step 3: Atypical presentation / No reversibility?
- Perform methacholine challenge test
- Positive (PC20 ≤ 8 mg/mL or equivalent) → Likely asthma
- Negative → Consider alternative diagnosis; obtain lung volumes, DLCO, chest imaging
Differential Diagnosis
COPD, vocal cord dysfunction, cystic fibrosis, bronchiectasis, congestive heart failure, sleep apnea, pneumonia, sarcoidosis, psychosomatic conditions
Biomarkers / Phenotyping
| Biomarker | Significance |
|---|---|
| FeNO (Fraction Exhaled NO) | Marker of IL-4/IL-13 mediated eosinophilic inflammation; elevated = eosinophilic/allergic asthma; responds to ICS |
| Blood eosinophils | >300 cells/µL suggests eosinophilic phenotype |
| Sputum eosinophils | Identifies steroid-responsive patients; requires specialized lab |
| Serum IgE | Elevated in allergic/atopic asthma; targets omalizumab therapy |
| Urinary bromotyrosine | Eosinophil peroxidase product; correlates with uncontrolled asthma and exacerbation risk |
6. Pulmonary Function Tests (PFTs)
| Parameter | Finding in Asthma |
|---|---|
| FEV1 | Reduced (obstructive pattern) |
| FVC | May be reduced |
| FEV1/FVC ratio | Reduced (<0.70) |
| Post-BD reversibility | ≥12% + ≥200 mL rise in FEV1 or FVC |
| Peak Expiratory Flow (PEF) | Reduced; diurnal variability >20% suggests poor control |
| Methacholine PC20 | ≤8 mg/mL = significant hyperresponsiveness |
ATS Impairment Rating for Asthma (3 domains scored 0-4):
- A. Post-bronchodilator FEV1 (0 = normal; 4 = <50% predicted)
- B. Reversibility / AHR (PC20)
- C. Minimum medication need (0 = none; 4 = daily oral steroids)
7. Asthma Control & Monitoring
- Peak Expiratory Flow (PEF) monitoring: diurnal variability >20% = suboptimal control
- PEF correlates strongly with symptom burden (Asthma Control Test)
- PEF predominantly reflects large airway patency - may underestimate small airway involvement
- PEF ≈ 7% lower with peak flowmeters vs. spirometry
- Personal best PEF should be established after optimal therapy and re-evaluated frequently
8. Management
Step Therapy (GINA-based)
| Step | Severity | Treatment |
|---|---|---|
| Step 1 | Mild intermittent | As-needed SABA (+ consider low-dose ICS per latest GINA) |
| Step 2 | Mild persistent | Low-dose ICS daily; OR as-needed low-dose ICS + formoterol |
| Step 3 | Moderate persistent | Low-dose ICS + LABA (combination inhaler) |
| Step 4 | Severe persistent | Medium/high-dose ICS + LABA |
| Step 5 | Refractory | High-dose ICS + LABA + add-on biologics or oral corticosteroids |
Key GINA 2019 update: SABA-only treatment (without ICS) is no longer recommended even for mild intermittent asthma - all patients should receive ICS because even mild asthma shows chronic airway inflammation.
Drug Classes
Short-Acting Beta-2 Agonists (SABA)
- Salbutamol (albuterol), terbutaline
- Rapid bronchodilation for acute symptoms (rescue)
- Frequent SABA need signals worsening control
Inhaled Corticosteroids (ICS) - Mainstay of controller therapy
- Beclomethasone, budesonide, fluticasone, mometasone, ciclesonide
- Oral bioavailability: fluticasone ~1%, mometasone <1%, ciclesonide near 0% (activated only in lung tissue) - minimizes systemic effects
- Systemic absorption from lung itself can cause: growth suppression in children, decreased bone mineral density, cataracts
- Preferred controller for all persistent asthma
Long-Acting Beta-2 Agonists (LABA)
- Formoterol, salmeterol
- Should only be used with ICS (never as monotherapy in asthma)
- ICS/LABA combination inhalers are preferred
Leukotriene Modifiers (LTMs)
- Montelukast, zafirlukast
- Alternative to ICS for mild persistent asthma; adjunct therapy
- Particularly useful with concomitant allergic rhinitis
Long-Acting Muscarinic Antagonists (LAMA)
- Tiotropium - add-on for step 4-5
Theophylline
- Oral bronchodilator and mild anti-inflammatory
- Narrow therapeutic window; requires monitoring
Biologic Therapies (for severe/refractory asthma)
| Drug | Target | Indication |
|---|---|---|
| Omalizumab | Anti-IgE | Allergic, severe asthma |
| Mepolizumab, reslizumab | Anti-IL-5 | Severe eosinophilic asthma |
| Benralizumab | Anti-IL-5Rα | Severe eosinophilic asthma |
| Dupilumab | Anti-IL-4Rα (blocks IL-4 + IL-13) | Severe eosinophilic asthma |
Assess biologic response markers: exacerbations, OCS use, lung function, FeNO, eosinophils. ~10-15% have no response.
9. Special Situations
Asthma in Pregnancy
- Poorly controlled asthma risks: preeclampsia, preterm birth, low birth weight, IUGR, perinatal death
- Natural history: 22% worsen, 29% improve, 49% unchanged
- Preferred ICS in pregnancy: Budesonide (best safety data); beclomethasone and fluticasone also acceptable
- LABA only with concurrent ICS
- Objective spirometry + home PEF monitoring recommended
- Risks of poorly controlled asthma far outweigh risks of drug therapy
Asthma + Obesity
- Obese asthmatics are a distinct, difficult-to-control phenotype
- Obesity-associated asthma may be non-Type 2 / non-eosinophilic
- High prevalence of comorbid OSA in obese asthmatics
Asthma + OSA (Nocturnal Asthma)
- OSA prevalence is increased in asthmatic patients
- Mechanisms of interaction: sleep fragmentation, hypoxemia → oxidative stress → bronchoconstriction
- CPAP improves asthma quality of life, reduces exacerbations and bronchodilator use
- CPAP is not recommended in asthmatics without OSA
Occupational Asthma / Work-Exacerbated Asthma
- Sensitizer-induced (new-onset) vs. work-exacerbated (pre-existing worsened by work)
- Requires identifying occupational exposures; removing sensitizer exposure critical
10. Inhaler Devices
- Peak Inspiratory Flow (PIF) ≥60 L/min is optimal for dry powder inhalers (DPIs)
- PIF <30 L/min = insufficient for DPI actuation
- Factors associated with low PIF: advanced age, female sex, reduced lung function
- High oropharyngeal deposition (up to 80% with pMDIs) → swallowed drug → importance of low oral bioavailability of ICS
Key Points Summary
- Asthma = chronic airway inflammation + variable airflow obstruction + AHR
- Diagnosis confirmed by reversibility on spirometry (FEV1/FVC ↑ ≥12% + ≥200 mL)
- Phenotyping (eosinophilic vs. non-eosinophilic) guides biologic selection
- ICS is the cornerstone of controller therapy at all steps
- GINA 2019: no SABA-only treatment - even mild asthma needs ICS
- LABA must always be co-prescribed with ICS
- PEF diurnal variability >20% = poor control
- Biologics are reserved for Step 5 severe/refractory disease
- Budesonide is the preferred ICS in pregnancy
- Comorbidities (OSA, obesity, GERD, rhinosinusitis) must be addressed
Source: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume (9780323655873), Chapter 62, pp. 1440-1533
This is a shared conversation. Sign in to Orris to start your own chat.