Explain me 10 common ecg of heart diseases with figure
Reading File
Finding Sources
Searching Images
ECG electrocardiogram heart disease patterns abnormal
Finding Sources
Searching Images
STEMI ST elevation myocardial infarction ECG
Searching Images
atrial fibrillation ECG tracing irregularly irregular
Searching Images
ventricular fibrillation VF cardiac arrest ECG
Searching Images
complete heart block third degree AV block ECG bradycardia
Searching Images
left bundle branch block LBBB ECG wide QRS
Searching Images
Wolff-Parkinson-White WPW syndrome delta wave ECG
Searching Images
ventricular tachycardia VT wide complex tachycardia ECG
Searching Images
long QT syndrome QTc prolonged ECG torsades de pointes
Searching Images
right bundle branch block RBBB ECG pattern
I now have excellent images for all 10 ECG patterns. Let me compile the comprehensive educational response.
10 Common ECG Patterns in Heart Disease
1. ST-Elevation Myocardial Infarction (STEMI)
Key ECG Features:
- ST-segment elevation ≥ 1 mm in ≥2 contiguous leads (≥2 mm in V1–V3)
- Hyperacute (tall, peaked) T-waves in early phase
- Pathological Q waves develop within hours (necrosis)
- Reciprocal ST depression in mirror leads
- "Tombstone" or convex-upward (coved) ST morphology in severe LAD occlusion
Localization by leads:
| Territory | Elevated leads | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Inferior | II, III, aVF | RCA |
| Lateral | I, aVL, V5–V6 | LCx |

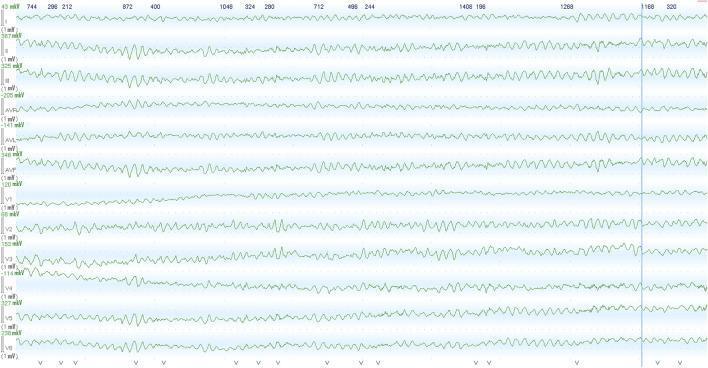
2. Atrial Fibrillation (AF)
Key ECG Features:
- Absent P waves — replaced by irregular fibrillatory (f) waves, best seen in V1
- Irregularly irregular R-R intervals — the hallmark
- Narrow QRS unless aberrant conduction present
- Ventricular rate varies (60–170 bpm in untreated AF)
Clinical context: Most common sustained arrhythmia. Causes include hypertension, valvular disease, thyrotoxicosis, heart failure, alcohol.

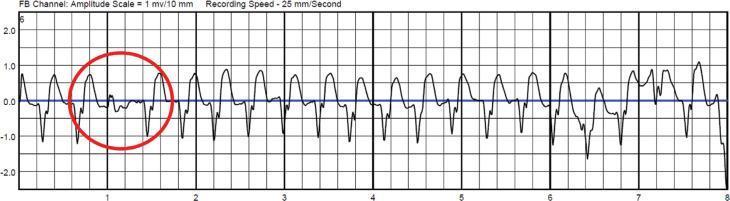
3. Ventricular Fibrillation (VF)
Key ECG Features:
- Chaotic, disorganized waveforms — no identifiable P, QRS, or T waves
- Completely irregular amplitude and frequency
- Coarse VF: higher amplitude fibrillatory waves (more recent onset, better chance of defibrillation success)
- Fine VF: low amplitude, harder to distinguish from asystole
Emergency: Immediately lethal without defibrillation. Shockable rhythm in ACLS.
4. Ventricular Tachycardia (VT)
Key ECG Features:
- Wide QRS complexes (>120 ms), typically >140–160 ms
- Rapid regular rate — typically 100–250 bpm
- No preceding P waves (or AV dissociation when visible)
- Capture beats and fusion beats are pathognomonic
- Positive or negative concordance in precordial leads
Types:
- Monomorphic VT: uniform QRS morphology (scar-related in structural heart disease)
- Polymorphic VT: varying QRS morphology (ischemia, long QT)
5. Complete (Third-Degree) AV Block
Key ECG Features:
- Complete AV dissociation — P waves and QRS complexes fire independently
- P rate > QRS rate (e.g., atrial rate 70–80 bpm; ventricular escape 30–50 bpm)
- No fixed PR interval — P waves "march through" QRS complexes
- Wide escape QRS if infra-nodal origin; narrow if junctional escape
Clinical significance: Causes syncope, hemodynamic compromise; requires pacemaker.
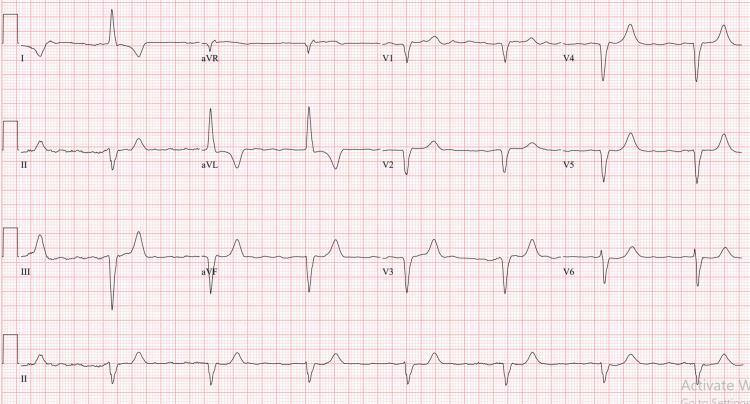
6. Left Bundle Branch Block (LBBB)
Key ECG Features:
- Wide QRS ≥ 120 ms
- Broad, notched "M-shaped" R-wave in lateral leads (I, aVL, V5, V6)
- Deep broad S-wave (QS pattern) in V1–V3
- Absent septal Q waves in lateral leads
- Discordant ST-T changes: T waves opposite to QRS vector
Significance: New LBBB in chest pain may indicate acute MI (Sgarbossa criteria apply). Associated with cardiomyopathy, hypertension, aortic stenosis.

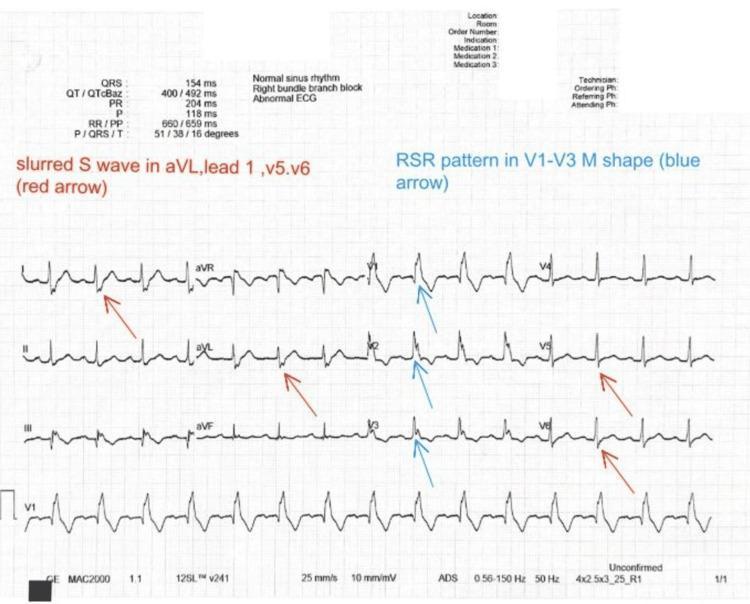
7. Right Bundle Branch Block (RBBB)
Key ECG Features:
- Wide QRS ≥ 120 ms
- rSR' ("rabbit ears") pattern in V1–V3 — classic sign
- Broad, slurred S-waves in lateral leads (I, aVL, V5, V6)
- T-wave inversion in V1–V3 (secondary repolarization change)
Significance: Isolated RBBB may be normal variant; new RBBB with anterior MI indicates proximal LAD occlusion (Brugada-type); also seen in pulmonary embolism, congenital heart disease.
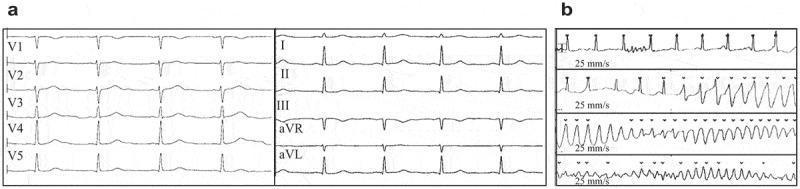
8. Wolff-Parkinson-White (WPW) Syndrome
Key ECG Features:
- Short PR interval (< 120 ms) — accessory pathway bypasses AV node
- Delta wave — slurred, slow upstroke at start of QRS
- Widened QRS (> 110 ms) due to pre-excitation
- Secondary ST-T changes discordant to delta wave
- Pseudo-infarct Q waves in inferior leads with posteroseptal pathway
Risk: Pre-excited AF can degenerate to VF → sudden cardiac death. Definitive treatment is catheter ablation.

9. Long QT Syndrome (LQTS)
Key ECG Features:
- Prolonged QTc (corrected for heart rate):
- Normal: ≤ 440 ms (men), ≤ 460 ms (women)
- Borderline: 440–470 ms
- Definite: > 500 ms = high risk for Torsades de Pointes
- Broad, notched T-waves or T-wave alternans (LQT2)
- Deep, notched T-U waves (LQT3)
- Can precipitate polymorphic VT (Torsades de Pointes)
Causes: Congenital (KCNQ1, KCNH2, SCN5A mutations), drugs (antiarrhythmics, antibiotics, antipsychotics), electrolyte disturbances (hypokalemia, hypomagnesemia).
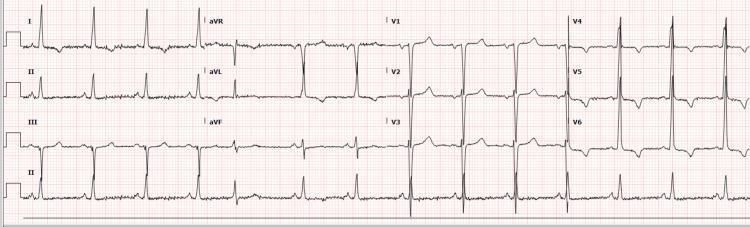
10. Left Ventricular Hypertrophy (LVH) with Strain
Key ECG Features:
- High voltage QRS — Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥ 35 mm
- Left ventricular strain pattern: ST depression + T-wave inversion in lateral leads (I, aVL, V4–V6)
- Left axis deviation
- Prolonged QRS (but usually < 120 ms)
- May show P-mitrale (bifid P in II, notched) if associated left atrial enlargement
Causes: Long-standing hypertension, aortic stenosis, hypertrophic cardiomyopathy.
Quick Reference Summary
| # | Pattern | Rate | Rhythm | P wave | QRS | Key Feature |
|---|---|---|---|---|---|---|
| 1 | STEMI | Normal | Regular | Normal | Normal | ST elevation + Q waves |
| 2 | Atrial Fibrillation | Variable | Irregular | Absent | Narrow | f-waves, irregular RR |
| 3 | Ventricular Fibrillation | — | Chaotic | Absent | None | Wavy baseline |
| 4 | Ventricular Tachycardia | 100–250 | Regular | Dissociated | Wide | Capture/fusion beats |
| 5 | 3rd Degree AV Block | Slow | Regular | Regular, dissociated | Wide escape | Complete AV dissociation |
| 6 | LBBB | Normal | Regular | Normal | ≥120 ms | M-wave lateral, QS V1–V3 |
| 7 | RBBB | Normal | Regular | Normal | ≥120 ms | rSR' V1, S-wave lateral |
| 8 | WPW | Normal | Regular | Normal | Widened | Short PR + delta wave |
| 9 | Long QT | Normal | Regular | Normal | Normal | QTc > 500 ms |
| 10 | LVH/Strain | Normal | Regular | Normal | High voltage | ST depression lateral leads |
Images sourced from peer-reviewed clinical ECG datasets (PMC Clinical VQA). All ECGs displayed at standard 25 mm/s paper speed and 10 mm/mV calibration unless noted.
This is a shared conversation. Sign in to Orris to start your own chat.