barium study in detail
Reading File
Finding Sources
Searching the Web
barium study radiology types indications technique findings
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive textbook content and images to compile a detailed, authoritative answer. Let me write it up.
Barium Studies - A Comprehensive Overview
Barium studies are fluoroscopic contrast examinations of the gastrointestinal (GI) tract using barium sulfate (BaSO₄) as a radio-opaque contrast agent. They provide real-time, dynamic imaging of the GI lumen, mucosa, and motility. While CT, MRI, and endoscopy have replaced barium studies for many indications, they remain clinically useful - particularly where these modalities are unavailable, in specific diagnostic scenarios, and for superior mucosal detail.
1. The Contrast Agent: Barium Sulfate
- Chemical: Barium sulfate (BaSO₄) - an insoluble, inert salt that is not absorbed from the GI tract
- Property: Strongly radio-opaque due to high atomic number of barium
- Formulations: Available as suspensions of varying density (35-40% weight/volume for small bowel follow-through, higher densities for double-contrast studies)
- Safety: Non-toxic because it is not absorbed. However, if it leaks into the peritoneal cavity or mediastinum (e.g. perforation), it causes severe chemical peritonitis/mediastinitis - a life-threatening complication
- Alternative - Water-soluble contrast (e.g. Gastrografin/iodinated contrast): Used when perforation is suspected (pharynx, esophagus, bowel anastomosis). Water-soluble agents are absorbed and excreted without the risk of barium peritonitis. Note: Gastrografin is hypertonic and contraindicated if aspiration risk is high (causes pulmonary edema)
2. Techniques: Single vs. Double Contrast
| Feature | Single Contrast | Double Contrast |
|---|---|---|
| Agent | Low-density barium, large volume | High-density barium (small volume) + air/gas |
| Mechanism | Fills the lumen completely | Thin barium coat on mucosa + air distension |
| Best for | Elderly/debilitated patients, suspected obstruction, fistulas, acute diverticulitis | Mucosal detail - polyps, early IBD, subtle lesions |
| Views | Fluoroscopy + mucosal relief + filling views | Double-contrast images supplemented by compression + mucosal relief |
Three types of views used in barium studies:
- Mucosal relief views - small volume barium in collapsed/partially collapsed lumen, shows mucosal fold pattern
- Barium-filled views - large volume fills lumen completely; good for gross lesions
- Double-contrast views - thin barium coating + gas distension; superior for subtle mucosal lesions
(Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Yamada's Textbook of Gastroenterology)
3. Types of Barium Studies
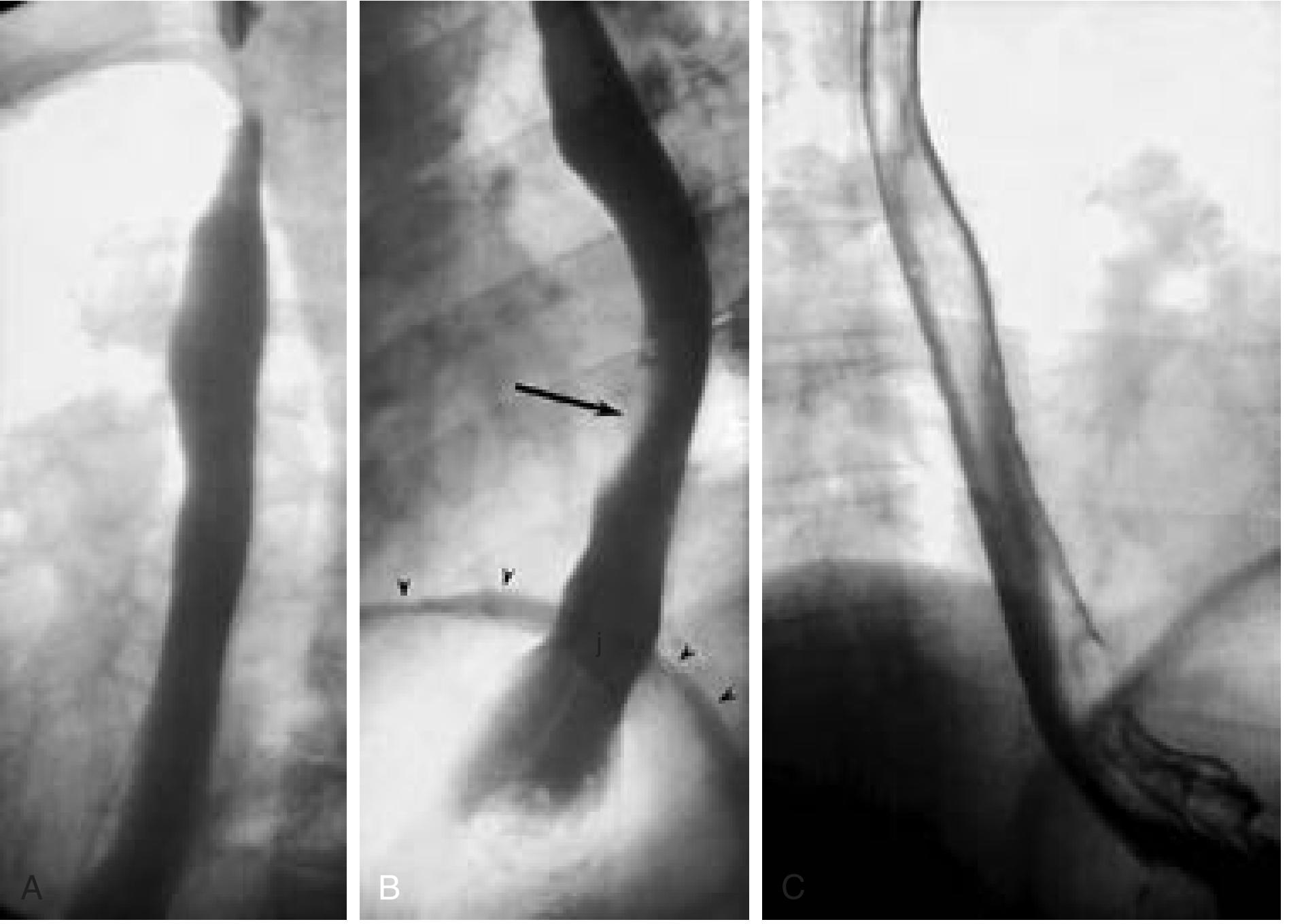
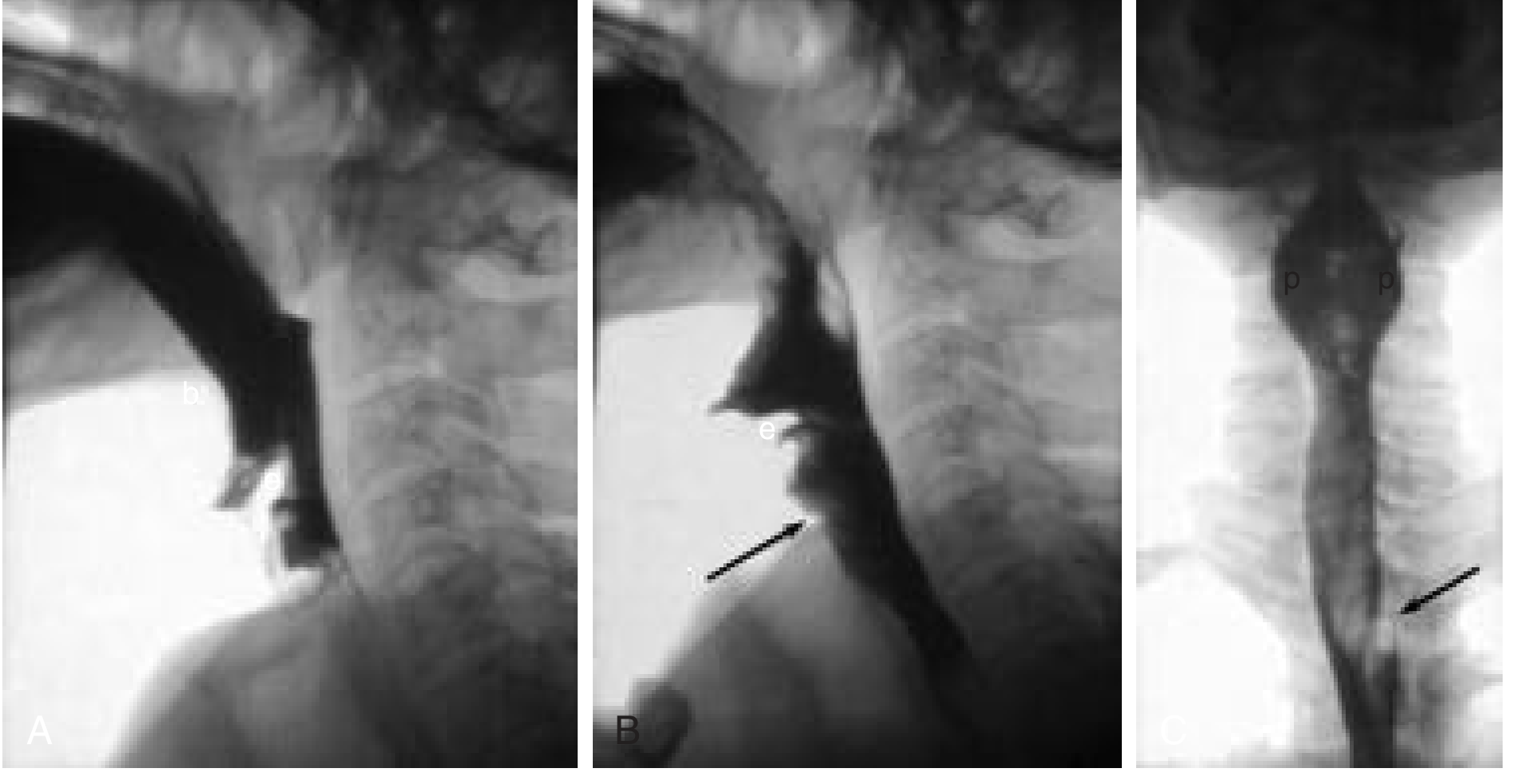
A. Barium Swallow (Esophagogram)
Also known as: Esophagogram, barium esophagogram
Purpose: Evaluates the structural and functional characteristics of the esophagus (and to some extent, the pharynx and proximal stomach).
Technique:
- Patient drinks liquid barium; fluoroscopic images taken in multiple projections
- Motility assessed with multiple single swallows in different positions, including recumbent (to assess peristalsis without gravity effect)
- Continuous and single swallows observed separately (a second swallow obliterates peristalsis of the first)
- The oesophageal lumen is distended with liquid barium, or coated with thick barium and distended by gas to show intrinsic irregularities and extrinsic impressions
Indications:
- Dysphagia (oropharyngeal and esophageal)
- Suspected esophageal stricture, web, ring (Schatzki's ring)
- Hiatal hernia - assessment of presence and reducibility
- Achalasia and esophageal motility disorders
- Suspected esophageal diverticulum (e.g. Zenker's)
- GERD evaluation - spontaneous reflux of barium into proximal esophagus is highly specific for reflux (though not sensitive)
- Pre-operative assessment of esophageal peristalsis before antireflux surgery
- Assessment for esophageal leiomyoma (appears as smooth, semilunar/crescent-shaped filling defect)
Clinical value: A 13 mm radiopaque pill or marshmallow given alongside barium helps identify subtle narrowings (Schatzki's rings, webs, minimally narrowed peptic strictures) that endoscopy may miss due to inadequate luminal distension. Sensitivity for esophagitis: 79-100% for moderate-to-severe disease; mild esophagitis is usually missed.
Provocative maneuvers for reflux: leg lifting, coughing, Valsalva, water siphon test - improve sensitivity but may reduce specificity.
Limitations:
- Barrett's esophagus cannot be reliably assessed
- Mild esophagitis frequently missed
- Not adequate for mucosal biopsies
- Both pharynx and esophagus should be examined even if complaint is only esophageal (35% of patients have simultaneous disorders of both)
(Sleisenger & Fordtran's; Scott-Brown's Otorhinolaryngology; Cummings Otolaryngology)
B. Modified Barium Swallow (MBS) / Videofluoroscopic Swallow Study (VFSS)
Purpose: Evaluates the coordination of the swallow reflex - specifically to determine cause and severity of tracheal aspiration. This is distinct from a standard barium swallow.
Key distinctions from standard barium swallow:
- Focuses on oral and pharyngeal phases of swallowing (not primarily the esophagus)
- Performed jointly with a speech-language pathologist
- Entire examination is videotaped (real-time fluoroscopic recording)
- Performed primarily in lateral projection (frontal supplemented for piriform sinus symmetry)
Technique:
- Patient given barium suspensions of several consistencies: thin liquid, thick liquid, paste, and solid
- Speech pathologist administers boluses while radiologist observes fluoroscopically
- If aspiration or laryngeal penetration is identified with neutral head position, protective maneuvers are tested: chin tuck, neck turn, postprandial forced cough
Aspiration rule: If a patient aspirates more than 10% of a bolus, they are considered high-risk. The examination should be terminated prematurely for patient protection if significant aspiration occurs.
Safety note: Barium aspiration into the lungs is dangerous - it can concrete within the lungs. Use should be cautious in patients with suspected high aspiration risk.
(Cummings Otolaryngology; Scott-Brown's Otorhinolaryngology)
C. Barium Meal (Upper GI Series)
Purpose: Examines the esophagus, stomach, and duodenum.
Technique:
- Double-contrast technique is standard: patient ingests effervescent granules to produce gas, then swallows high-density barium
- Multiphasic study: double-contrast views (upright), single-contrast compression views (prone), mucosal relief views
- Spot images of all mucosal surfaces in multiple positions
- Important for duodenum: Double-contrast views are supplemented with prone compression views (low-density barium) because up to 50% of duodenal ulcers are on the anterior wall - not optimally coated in supine position
Indications:
- Suspected peptic ulcer disease (gastric or duodenal ulcer)
- Epigastric pain, nausea, vomiting
- Suspected gastric carcinoma
- Suspected esophagogastric junction pathology
- Gastric outlet obstruction
- Post-surgical anatomy assessment
- Hiatal hernia
Key findings:
- Gastric ulcers: primarily on lesser curvature or posterior wall
- Duodenal ulcers: up to 50% on anterior wall
- Linitis plastica (leather-bottle stomach): reduced distensibility due to diffuse gastric infiltration
- "Apple core" or "shouldering" lesion: carcinoma
D. Small Bowel Follow-Through (SBFT) / Barium Small Bowel Series
Purpose: Examines the small intestine from duodenojejunal junction to terminal ileum.
Technique:
- Patient ingests 500-600 mL of a 35-40% (weight/volume) barium sulfate suspension
- Serial overhead abdominal radiographs at timed intervals
- Fluoroscopy is the primary examination method - periodic spot imaging of jejunum and ileum with manual palpation and abdominal compression to separate overlapping loops
- Examination continues until all loops including terminal ileum are demonstrated

Indications:
- Suspected Crohn's disease (terminal ileal disease)
- Small bowel obstruction (intermittent or low-grade)
- Malabsorption evaluation
- Suspected small bowel tumor
- Radiation enteropathy
- Surgical anatomy planning
Limitations:
- CT/MR enterography has largely replaced SBFT for most indications
- Unreliable without fluoroscopy - overhead-only technique misses many lesions due to overlapping loops
- Radiation exposure
(Yamada's Textbook of Gastroenterology; Grainger & Allison's Diagnostic Radiology)
E. Enteroclysis (Small Bowel Enema)
Purpose: Provides a more detailed fluoroscopic study of the entire small bowel compared to SBFT.
Technique:
- A tube is passed nasally into the proximal small bowel (beyond the ligament of Treitz)
- Barium + methylcellulose + air are instilled at controlled rates
- This achieves optimal bowel distension - the key advantage over SBFT
- Double-contrast technique (air after contrast agent) outlines mucosa and walls in superior detail
Advantages over SBFT:
- Controlled bowel distension - superior mucosal detail
- Excellent for subtle mucosal changes (early Crohn's, malabsorption)
- Diagnostic yield: 10-25% for small bowel bleeding (vs. 0-6% for standard SBFT)
Disadvantages:
- Uncomfortable for the patient (requires nasoenteric intubation)
- Technically demanding - requires expertise
- Greater radiation exposure than SBFT
- Rarely performed in modern practice due to availability of VCE and CT/MR enterography
(Clinical Gastrointestinal Endoscopy; Yamada's Textbook of Gastroenterology)
F. Barium Enema (Large Bowel Enema)
Purpose: Examines the colon from rectum to cecum.
Patient preparation: Thorough bowel cleansing (laxatives + dietary restriction); inadequate prep is a major source of error.
Techniques:
Single-contrast barium enema:
- Entire colon filled with low-density barium under fluoroscopic control
- Extensive palpation and compression during filling
- Post-evacuation radiograph for mucosal detail
- Preferred for: suspected obstruction, acute diverticulitis, fistulas, elderly/debilitated patients
Double-contrast barium enema (DCBE):
- Small volume high-density barium → coat mucosa → insufflation of air → distension
- Superior for: polyps, early IBD changes, rectal lesions, flexures, rectum
- Overall accuracy: ~95% for colorectal cancer detection
Indications:
- Detection of colorectal polyps and cancer
- IBD - type, extent, severity
- Diverticular disease and complications
- Extrinsic mass lesions involving the colon
- Evaluation of the rectum
- Incomplete colonoscopy (to visualize proximal colon)
- Suspected Hirschsprung's disease (confirms presence; manometry and histology needed for definitive diagnosis)
- Megacolon/megarectum, redundant sigmoid
Limitations and accuracy:
- Polyp detection rates: 32% for adenomas <6 mm, 53% for 6-10 mm, 48% for >10 mm (National Polyp Study)
- False-positive rate: 5-10% (inadequate bowel prep, diverticulosis mimicking polyps)
- False-negative rate: 10% (diverticulosis, redundant bowel, poor mucosal coating)
- Fails to detect 50% of polyps >10 mm (making it inadequate as a standalone screening tool)
- No role in LGI bleeding - cannot demonstrate vascular lesions; may delay angiography by impairing visualization
- Largely replaced by colonoscopy and CT colonography for screening
(Sleisenger & Fordtran's; Yamada's Textbook of Gastroenterology)
4. Contraindications
| Contraindication | Study |
|---|---|
| Suspected perforation | Barium contraindicated - use water-soluble contrast |
| Toxic megacolon | Barium enema absolutely contraindicated |
| Recent bowel anastomosis (within 5-7 days) | Barium enema contraindicated |
| High aspiration risk | Modified barium swallow - use with extreme caution; Gastrografin (water-soluble) contraindicated if aspiration risk (causes pulmonary edema) |
| Large bowel obstruction | Single-contrast preferred over double; barium may worsen impaction |
| Active, severe GI bleeding | No barium enema (impairs colonoscopy visualization) |
5. Comparison with Other Modalities
| Parameter | Barium Study | Endoscopy | CT/MRI |
|---|---|---|---|
| Mucosal detail | Very good (especially DC) | Excellent | Moderate |
| Motility assessment | Yes (real-time fluoroscopy) | Limited | No (static) |
| Biopsy capability | No | Yes | No |
| Extramural lesions | Limited | No | Excellent |
| Radiation | Moderate | None | Higher (CT) |
| Cost | Low | Higher | Higher |
| Availability | Wide | Moderate | Moderate |
| Therapeutic | No | Yes | Limited |
6. Radiation Dose Considerations
Barium studies involve fluoroscopic radiation. Dose varies by study:
- Simple barium swallow: relatively low
- Small bowel follow-through/enteroclysis: moderate (prolonged fluoroscopy time)
- Barium enema: moderate
Current consensus is that for small bowel evaluation, the diagnostic yield of barium studies may not justify the radiation exposure when CT/MR enterography is available. However, barium studies offer superior spatial resolution for mucosal detail compared to CT and MRI when performed optimally.
7. Summary of Clinical Applications by Region
| Region | Study | Key Uses |
|---|---|---|
| Pharynx | Modified barium swallow (VFSS) | Aspiration, dysphagia, post-stroke swallowing |
| Esophagus | Barium swallow/esophagogram | Stricture, ring, web, motility, hiatal hernia, diverticulum |
| Stomach + Duodenum | Barium meal (upper GI series) | PUD, gastric carcinoma, outlet obstruction |
| Small bowel | SBFT / Enteroclysis | Crohn's, obstruction, malabsorption, tumors |
| Colon | Barium enema (SC or DC) | CRC, polyps, IBD, diverticular disease, Hirschsprung's |
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease; Yamada's Textbook of Gastroenterology (7th ed.); Grainger & Allison's Diagnostic Radiology; Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Bailey and Love's Short Practice of Surgery (28th ed.); Clinical Gastrointestinal Endoscopy (3rd ed.)
This is a shared conversation. Sign in to Orris to start your own chat.