Swollen external hemorrhoids
Reading File
Finding Sources
Searching PubMed
"external hemorrhoids" AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Swollen External Hemorrhoids
Anatomy & Pathophysiology
External hemorrhoids arise from the inferior hemorrhoidal plexus, located below the dentate line, and are covered by modified squamous epithelium (anoderm) — a richly innervated tissue that makes external hemorrhoids far more painful than internal ones. They represent normal anal vascular cushions that become symptomatic when the supporting muscularis submucosa weakens, allowing engorgement and distension of the vascular channels. — Rosen's Emergency Medicine, p. 1345
Key contributing factors:
- Straining and constipation (increased intra-abdominal pressure → venous backflow)
- Prolonged sitting, heavy lifting, frequent loose stools
- Pregnancy (direct venous compression)
- Genetic/familial predisposition
Clinical Presentation
Swollen external hemorrhoids typically produce:
- Pain — often the dominant complaint (unlike internal hemorrhoids, which are usually painless unless thrombosed)
- Swelling — visible perianal mass
- Itching, mucoid discharge, moist perianal area
- Bright red bleeding — if traumatized
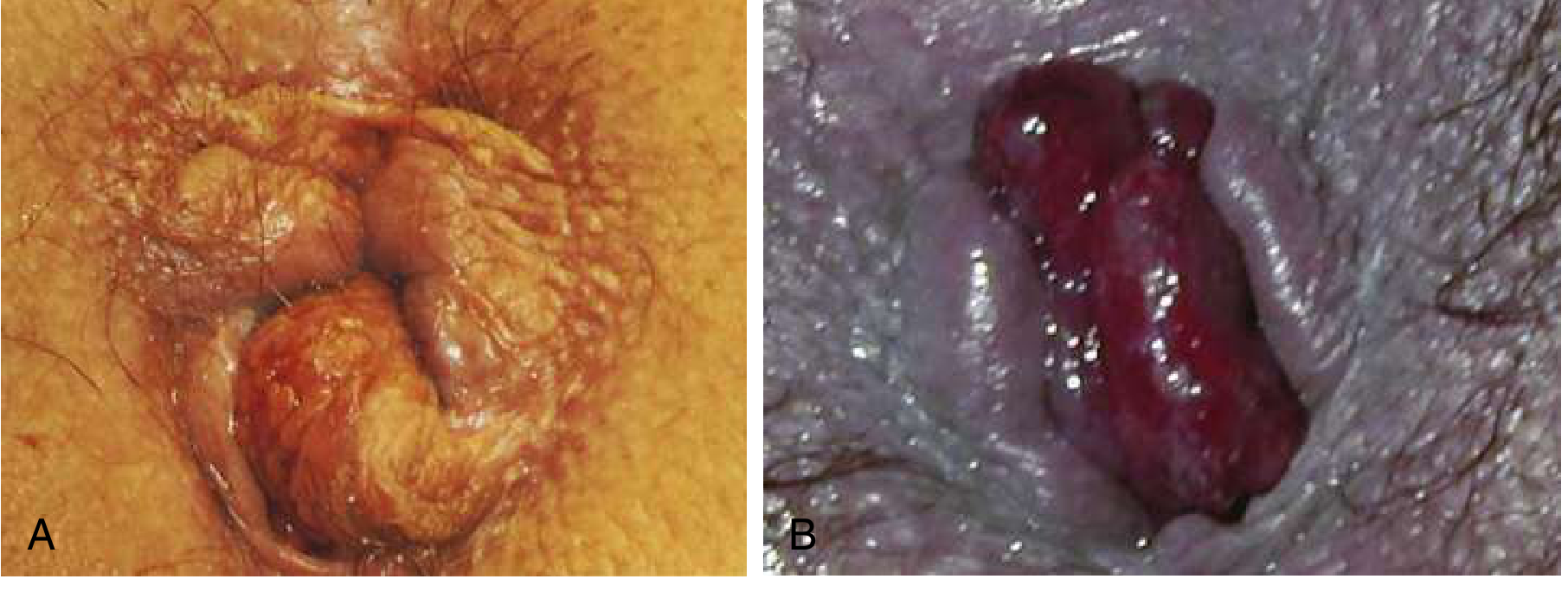
Thrombosis is the most dramatic presentation: sudden onset of a tense, exquisitely tender bluish-purple perianal mass that appears when a clot forms within the external hemorrhoid. Pain peaks in the first 48–72 hours.
Diagnosis
Diagnosis is clinical — history and external inspection:
- Visual inspection at rest and during straining
- Note skin tags (residual from prior thrombosis), edema, color, and reducibility
- Anoscopy is contraindicated in acutely thrombosed or severely swollen hemorrhoids due to pain
- Consider flexible sigmoidoscopy/colonoscopy if: patient >40 years, persistent bleeding, or an alternative source of colorectal bleeding cannot be excluded
Management
Conservative (Non-thrombosed Swollen External Hemorrhoids)
The WASH regimen is the standard first-line approach: — Rosen's Emergency Medicine, p. 1345
| Component | Details |
|---|---|
| Warm water | Sitz baths at ~40°C (104°F) for 10–15 min, 2–3×/day; decreases anal canal pressure, eases swelling |
| Analgesics | Acetaminophen or NSAIDs (ibuprofen preferred for its anti-inflammatory effect) |
| Stool softeners | Psyllium (Metamucil) 1–2 tsp in 8 oz water daily; docusate |
| High-fiber diet | 20–30 g dietary fiber/day + adequate fluid intake (6–8 glasses/day) |
Topical agents (witch hazel, mineral oil, cocoa butter, lidocaine gel): provide temporary symptomatic relief and improve hygiene — no agent is proven superior to another. Topical corticosteroids should not be used beyond a few days due to risk of skin atrophy.
Thrombosed External Hemorrhoid — Time-Sensitive Decision
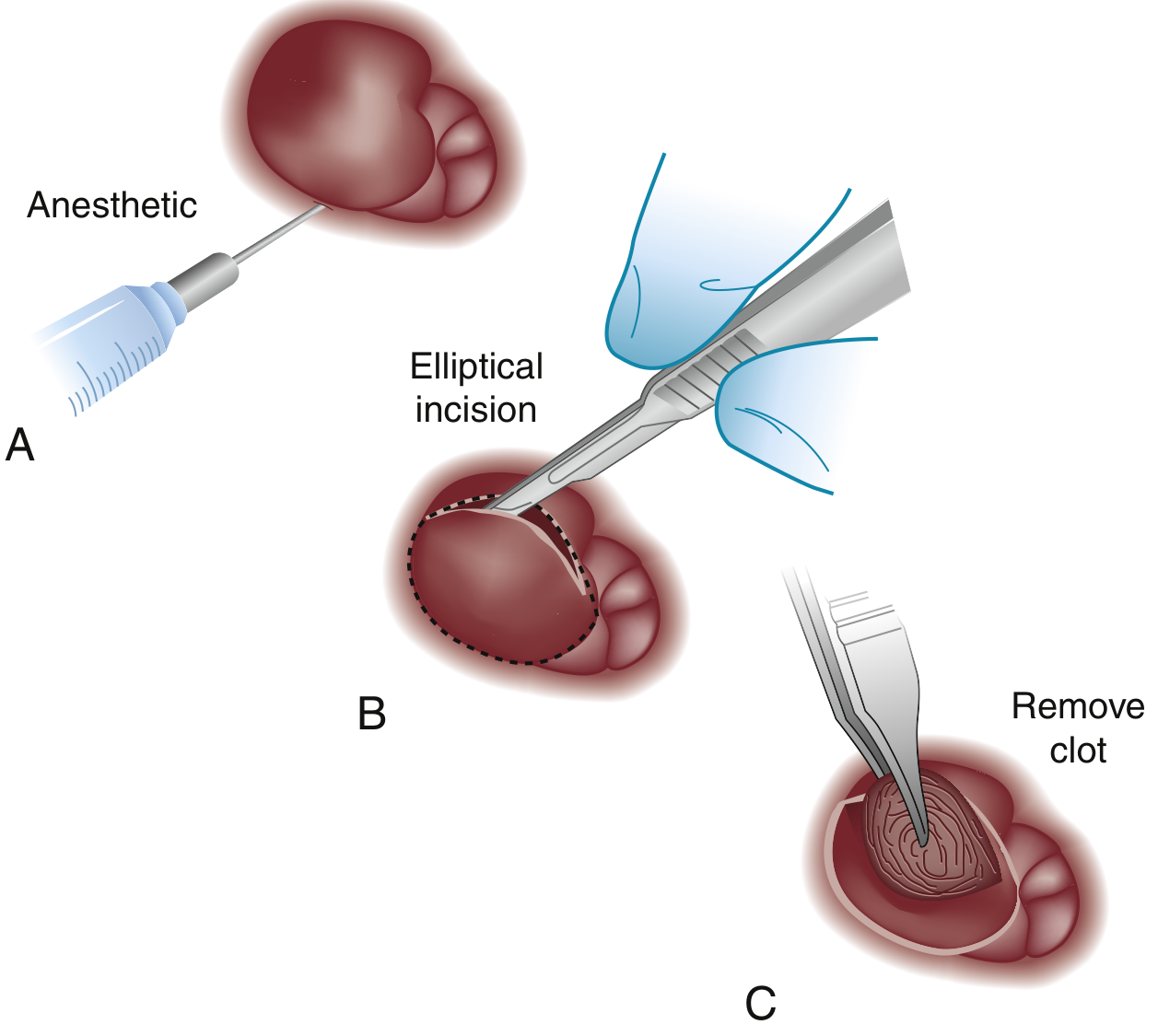
Within 72 hours of symptom onset → Excision (preferred over incision):
- Field block with local anesthetic (e.g., 1% lidocaine with epinephrine)
- Elliptical excision of the overlying skin and complete removal of the clot en bloc
- Simple incision is discouraged — results in incomplete clot evacuation, rebleeding, and skin tag formation
- Provides rapid, definitive pain relief
After 72 hours (pain usually beginning to subside spontaneously):
- Conservative management preferred (WASH regimen)
- The thrombosis will ulcerate and spontaneously drain over days
- Residual skin tags are common and may complicate hygiene
Excision is generally avoided in: pediatric patients, pregnant women, immunocompromised patients (unless symptoms are severe). — Rosen's Emergency Medicine, p. 1346
Surgical Management Summary
| Classification | Management |
|---|---|
| Thrombosed external hemorrhoid (≤72 h) | Excision in ED/office |
| Non-thrombosed swollen external | WASH regimen |
| 2nd/3rd degree internal | Banding, sclerotherapy, elective hemorrhoidectomy |
| 4th degree thrombosed/gangrenous | Emergent hemorrhoidectomy |
Disposition & Red Flags
Refer urgently if:
- Irreducible prolapse (Grade IV internal)
- Gangrenous tissue (black/necrotic) → emergent hemorrhoidectomy
- Uncontrolled bleeding
- Immunocompromised patient with significant thrombosis
Recent evidence update: A 2026 meta-analysis (PMID 40576944) comparing operative vs. non-operative treatment of thrombosed external hemorrhoids found surgical excision provides faster pain relief and lower recurrence, supporting the ≤72-hour excision recommendation above.
Sources: Rosen's Emergency Medicine (9e), p. 1344–1346 | Sleisenger & Fordtran's GI and Liver Disease | Textbook of Family Medicine (9e)
This is a shared conversation. Sign in to Orris to start your own chat.