MI
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
"myocardial infarction"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
I now have all the essential information needed for a comprehensive MI review. Let me compile the full response.
Myocardial Infarction (MI) - Comprehensive Review
Definition
MI (commonly called a "heart attack") is the death of cardiac muscle due to prolonged ischemia, most often caused by atherosclerotic coronary artery disease (CAD). In the United States, roughly 800,000 MIs occur each year - nearly one every 40 seconds - causing approximately 400,000 deaths annually.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 511
Epidemiology & Risk Factors
- 10% of MIs occur in people under 40 years; 45% occur under 65 years
- Male sex increases relative risk through middle age
- Postmenopausal women lose estrogen protection, with rising CAD risk; IHD is the most common cause of death in older females
- Postmenopausal hormonal replacement therapy has not been shown to be protective and may be detrimental (pro-thrombotic effect)
- Classic risk factors: hypertension, dyslipidemia, diabetes, smoking, obesity, family history
Classification
Type 1 MI
Caused by atherosclerotic plaque rupture leading to thrombotic coronary occlusion and infarction. Subdivided into:
- STEMI - ST-segment elevation on ECG + elevated cardiac biomarkers
- NSTEMI - Same biomarker elevation but without ST-elevation
Type 2 MI
Caused by supply-demand mismatch ("demand ischemia") - e.g., severe tachycardia, hypotension, anemia, vasospasm. Treatment targets reducing cardiac oxygen demand rather than revascularization.
Unstable angina = ischemic symptoms without biomarker elevation. STEMI + NSTEMI + unstable angina form the Acute Coronary Syndrome (ACS) spectrum.
- Sabiston Textbook of Surgery, p. 2928
Pathogenesis
The sequence underlying most MIs:
- Plaque disruption - An atheromatous plaque is eroded or suddenly ruptured by endothelial injury, intraplaque hemorrhage, or mechanical forces, exposing subendothelial collagen and necrotic plaque contents
- Platelet activation - Platelets adhere, aggregate, and release thromboxane A2, ADP, and serotonin - causing further platelet aggregation and vasospasm
- Coagulation cascade - Tissue factor activates the coagulation cascade, adding to the thrombus
- Complete occlusion - Within minutes, the thrombus can completely occlude the coronary lumen
When angiography is performed within 4 hours of MI onset, coronary thrombosis is demonstrated in ~90% of cases. By 12-24 hours, evidence of thrombosis is seen in only ~60%, even without intervention - indicating some spontaneous thrombolysis occurs.
Atypical causes (~10% of cases):
-
Vasospasm (cocaine, ephedrine, Prinzmetal angina)
-
Embolism (from LA thrombus in AF, endocarditis vegetations, prosthetic material, paradoxical embolism via PFO)
-
Vasculitis
-
Hematologic abnormalities (e.g., sickle cell disease, hypercoagulable states)
-
Amyloid deposition in vascular walls
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 511-512
Coronary Artery Territories
| Artery | Frequency | Infarct Location |
|---|---|---|
| LAD | 40-50% | Anterior LV wall near apex, anterior ventricular septum, apex |
| RCA | 30-40% | Inferior/posterior LV wall, posterior ventricular septum, ± RV free wall |
| LCx | 15-20% | Lateral LV wall (except apex) |
- Right ventricular infarction complicates 15-30% of RCA occlusions
- Isolated RV infarction: only 1-3% of cases
Morphologic Evolution (Table 12.5 from Robbins)
| Time | Gross Appearance | Light Microscopy | EM |
|---|---|---|---|
| 0-0.5 hr | None | None | Myofibril relaxation, glycogen loss, mitochondrial swelling |
| 0.5-4 hr | None | Usually none; wavy fibers at border | Sarcolemmal disruption; mitochondrial amorphous densities |
| 4-12 hr | Dark mottling (occasional) | Early coagulative necrosis; edema; hemorrhage | - |
| 12-24 hr | Dark mottling | Ongoing coagulative necrosis; nuclear pyknosis; myocyte hypereosinophilia; early neutrophil infiltrate | - |
| 1-3 days | Mottling with yellow-tan center | Full coagulative necrosis, loss of nuclei and striations; brisk neutrophilic infiltrate | - |
| 3-7 days | Hyperemic border; central yellow-tan softening | Disintegrating dead myofibers; dying neutrophils; early macrophage phagocytosis; early granulation tissue at border | - |
| 7-10 days | Maximally yellow-tan and soft, depressed red-tan margins | Well-developed phagocytosis; granulation tissue at margins | - |
| 10-14 days | Red-gray depressed borders | Established granulation tissue with new vessels and collagen | - |
| 2-8 weeks | Gray-white scar forming from border inward | Increasing collagen, decreasing cellularity | - |
| >2 months | Scarring complete | Dense collagenous scar | - |
Key staining note: Triphenyl tetrazolium chloride (TTC) stain - intact myocardium stains brick-red (preserved LDH activity); infarcted areas appear as unstained pale zones (LDH leaked through damaged membranes).
ECG Changes in MI (Ganong's Physiology)
Three underlying electrical changes explain ECG findings:
| Defect in Infarcted Cells | Current Flow | ECG Change (leads over infarct) |
|---|---|---|
| Rapid repolarization (accelerated K+ channel opening) | Out of infarct | ST-segment elevation |
| Decreased resting membrane potential (K+ loss) | Into infarct during diastole | TQ depression - recorded as ST elevation |
| Delayed depolarization | Out of infarct | ST-segment elevation |
-
Acute phase: ST-segment elevation in leads over the infarct; reciprocal ST depression in opposite leads
-
Days to weeks later: ST abnormalities subside; dead muscle becomes electrically silent
-
Chronic changes: New Q waves appear; loss of R-wave progression in anterior leads
-
Non-Q-wave infarcts: less severe but higher rate of subsequent reinfarction
-
Ganong's Review of Medical Physiology, p. 534
ECG Localization
| Lead Changes | Territory | Artery |
|---|---|---|
| V1-V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA |
| I, aVL, V5-V6 | Lateral | LCx |
| V1-V2 (reciprocal changes) | Posterior | RCA/LCx |
| ST elevation in V4R | Right ventricle | RCA |
Diagnosis
Biomarkers
Cardiac troponins (cTnI and cTnT) are the gold standard:
- Present at very low concentrations in normal serum
- High-sensitivity (hs) assays: detection threshold ~1-2 ng/L; upper 99th percentile ~10-30 ng/L (varies by age, sex, assay)
- Rise detectable within 3-6 hours of infarction onset
- Elevations are not exclusive to MI - also seen in myocarditis, pericarditis, pulmonary embolism, renal failure, sepsis, critical illness, and after intense exercise
- Serial troponins with rising/falling pattern are key to diagnosing AMI vs. chronic elevation
Older markers (now rarely used): CK-MB, myoglobin, AST, LDH - all diagnostically inferior to troponin.
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 313
Diagnostic Triad
- Clinical symptoms (chest pain, diaphoresis, radiation to arm/jaw, dyspnea)
- ECG changes
- Rise and/or fall of cardiac biomarkers (troponin)
Management
Immediate Goals
- Restore perfusion as fast as possible ("time is muscle")
- Limit infarct size
- Prevent and treat complications
STEMI
- Primary PCI (percutaneous coronary intervention): preferred reperfusion strategy - goal door-to-balloon time <90 min
- Thrombolysis: if timely PCI unavailable
NSTEMI/UA
- Antiplatelet therapy, anticoagulation
- Intervention can be delayed up to 72 hours in some cases (risk-stratify with TIMI/GRACE score)
Drug Therapy
| Drug | Rationale |
|---|---|
| Aspirin | Antiplatelet; given immediately |
| P2Y12 inhibitor (clopidogrel, ticagrelor, prasugrel) | Dual antiplatelet therapy |
| Beta-blockers | Reduce heart rate/oxygen demand; cardioprotective - avoid if hypotension, bradycardia, or cardiogenic shock |
| Nitroglycerin (sublingual or IV) | Chest pain relief, reduces preload/afterload - avoid in right-sided MI (risk of catastrophic preload reduction) |
| IV opioids (morphine) | Pain control if nitroglycerin insufficient |
| ACE inhibitors/ARBs | Reduce remodeling, especially with reduced EF |
| Statins | Plaque stabilization and lipid control |
| Anticoagulation (heparin, LMWH) | Prevent thrombus propagation |
Critical distinction: In a suspected right-sided MI (inferior STEMI + right-sided leads), nitroglycerin can precipitate fatal hypotension by reducing preload to a preload-dependent right ventricle. Always check right-sided ECG (V4R) in inferior MI.
- Sabiston Textbook of Surgery, pp. 2934-2936
Complications (~75% of patients experience at least one)
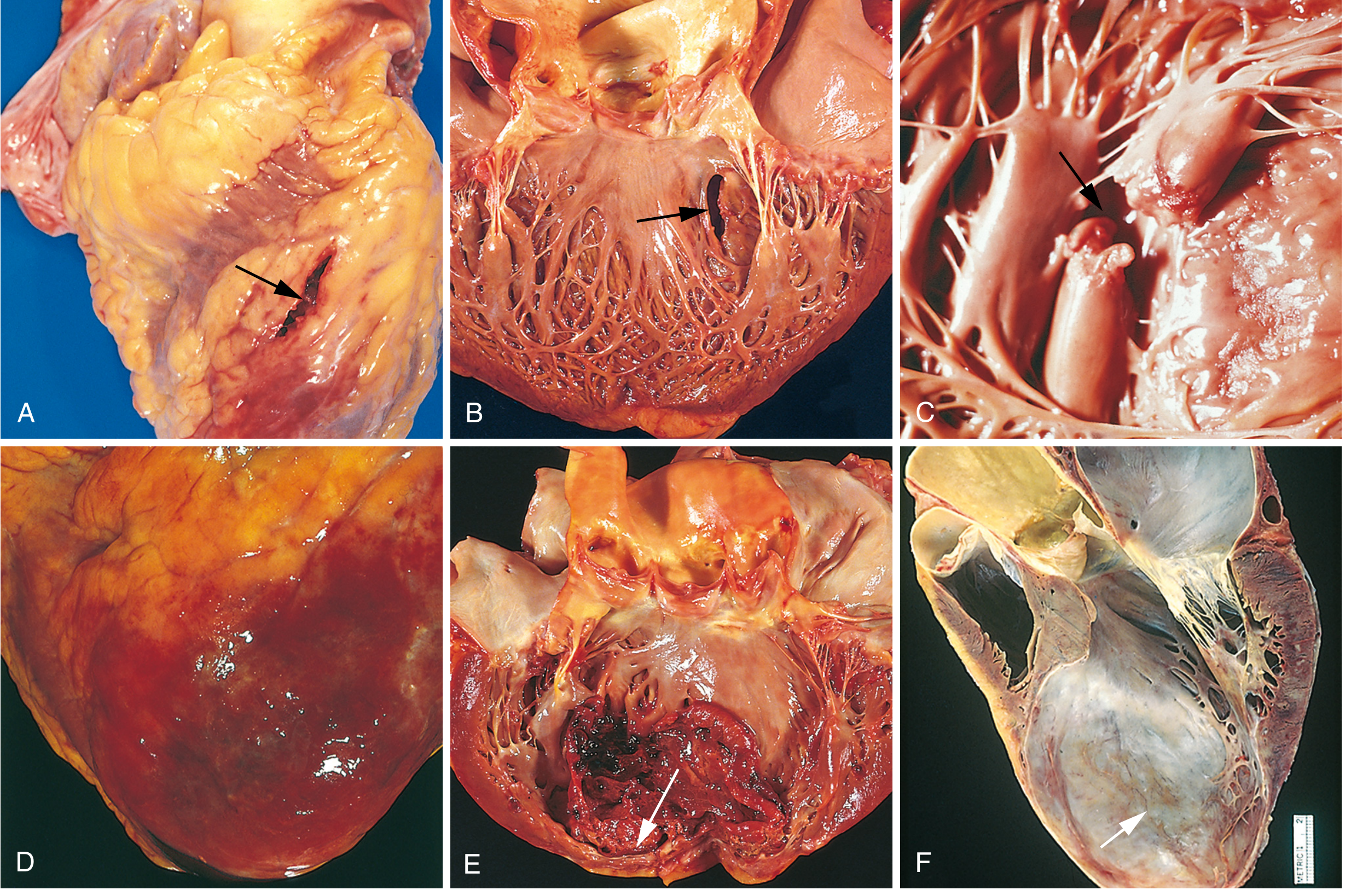
Fig. 12.17 - Complications of MI (Robbins, Cotran & Kumar)
1. Contractile Dysfunction
- LV failure proportional to volume of damage
- Cardiogenic shock: ~10% of transmural MIs; typically when ≥40% of the LV is damaged; high mortality
2. Arrhythmias
- Most common cause of early out-of-hospital death
- Ventricular fibrillation is the most dangerous
- A defibrillator must be immediately available for all MI patients
- AF, heart block (especially in inferior MI with AV node involvement) also common
3. Papillary Muscle Dysfunction/Rupture
- Papillary muscles often ischemic - causes mitral regurgitation
- Papillary muscle rupture (day 3-7): catastrophic acute MR - medical emergency
4. Myocardial Rupture (1-3% of MIs, frequently fatal)
Occurs most commonly 3-7 days after infarction (when myolysis peaks before sufficient scar forms):
- Free wall rupture → hemopericardium → cardiac tamponade (most common)
- Ventricular septal rupture → VSD with left-to-right shunt
- Papillary muscle rupture → severe acute mitral regurgitation
5. Right Ventricular Infarction
- Usually from RCA occlusion extending into RV
- Results in right-sided heart failure: JVD, hypotension, clear lungs (no pulmonary edema)
- Treatment: IV fluids to maintain preload; avoid preload-reducing agents (nitrates, diuretics)
6. Infarct Expansion and Ventricular Aneurysm
- Infarct expansion: thinning and dilation of infarcted zone (days-weeks)
- True aneurysm: late complication; dyskinetic wall segment; risk of mural thrombus and systemic embolism; anticoagulation recommended
- Risk of VT from re-entry around the aneurysm
7. Mural Thrombus
- Forms on dyskinetic endocardium, especially anterior MI
- Risk of systemic arterial embolism (stroke, limb ischemia)
8. Pericarditis
- Early (1-3 days): fibrinous pericarditis over the infarcted zone
- Dressler syndrome (weeks later): immune-mediated; pleuropericarditis, fever
9. Sudden Cardiac Death (SCD)
-
325,000 deaths/year in the US
-
Mechanism: ventricular fibrillation or asystole
-
One-third of out-of-hospital STEMI patients die within 1 hour of onset before reaching care
-
ICD implantation markedly improves prognosis in at-risk survivors
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 516-518
Post-MI Management (Long-term)
- Dual antiplatelet therapy (duration depends on stent type)
- Statin (high-intensity)
- Beta-blocker (especially if reduced EF)
- ACE inhibitor/ARB (if EF ≤40%)
- Cardiac rehabilitation
- Risk factor modification (smoking cessation, BP control, glucose control, weight loss)
- ICD implantation if EF ≤35% persists after 3 months of optimal therapy
Key Summary Points
| Feature | STEMI | NSTEMI | Type 2 MI |
|---|---|---|---|
| Cause | Plaque rupture + complete occlusion | Plaque rupture + partial occlusion | Supply-demand mismatch |
| ECG | ST elevation | ST depression / T-wave changes / normal | Variable |
| Troponin | Elevated | Elevated | Elevated |
| Treatment | Emergent PCI / thrombolysis | Antiplatelet + PCI within 72 hr | Treat underlying cause |
| In-hospital mortality | ~9% | ~6% | Variable |
The overall in-hospital death rate for MI is less than 7%. Out-of-hospital STEMI mortality is far worse - one-third of patients die before reaching the hospital, usually from arrhythmia within 1 hour of onset.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Ganong's Review of Medical Physiology (26th ed.); Sabiston Textbook of Surgery; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.