Lap cholecystectomy with down syndrome adult patient with aesthetic consideration
laparoscopic cholecystectomy "Down syndrome"
"Down syndrome" anesthesia surgical considerations adult
PMID: 34165727
PMID: 36610856
Laparoscopic Cholecystectomy in an Adult with Down Syndrome - Anesthetic & Surgical Considerations
1. Why This Patient is a Special Population
2. Preoperative Evaluation
A. Cardiovascular Screen
- Congenital heart disease (CHD) occurs in ~40% of patients: most commonly endocardial cushion defect (AV canal), VSD, and ASD. Even in adults, many may have uncorrected or repaired lesions.
- Pulmonary hypertension is a common sequela of left-to-right shunts and must be specifically sought. It is a relative contraindication to laparoscopic surgery because pneumoperitoneum raises PaCO2 and further increases pulmonary vascular resistance.
- Obtain ECG and echocardiography if not done recently. Patients with significant CHD warrant cardiology clearance. - Morgan & Mikhail's Clinical Anesthesiology 7e, Sabiston Textbook of Surgery
- Adults with both Down syndrome and CHD undergoing noncardiac surgery have a systematically higher risk profile and should be evaluated for pulmonary artery pressures [PMID 36610856].
B. Airway Assessment
- Anticipate a difficult airway as the default:
- Macroglossia and relative macroglossia
- High-arched palate, midface hypoplasia, micrognathia
- Short neck
- Subglottic stenosis (may require a smaller ETT than predicted by age/weight)
- Airway malacia, tracheal bronchus (congenital lower airway anomalies in ~71% vs ~32% of controls)
- Dysphonia/vocal fold paralysis in patients who had prior cardiac surgery (left recurrent laryngeal nerve injury)
- Plan for video laryngoscopy or fiberoptic intubation as primary airway management, not a backup. - Miller's Anesthesia 10e
C. Atlantoaxial Instability (AAI) - CRITICAL
- Generalized ligamentous laxity from collagen defect causes atlantoaxial and atlantooccipital instability in up to 15-20% of DS patients.
- Symptoms to screen for: neck pain, torticollis, gait changes, change in bowel/bladder function, upper extremity weakness.
- If no prior cervical spine imaging or if symptomatic: obtain lateral flexion/extension cervical spine X-rays before surgery.
- If AAI is confirmed with neurological symptoms: neurosurgery consult.
- Intraoperative implication: Avoid aggressive neck flexion during laryngoscopy; use in-line stabilization; avoid steep Trendelenburg and reverse Trendelenburg head positions that stress the cervical spine. - Miller's Anesthesia 10e, Bradley and Daroff's Neurology
D. Obstructive Sleep Apnea (OSA)
- OSA is extremely common in adults with DS due to hypotonia, midfacial hypoplasia, macroglossia, obesity, and narrow nasopharynx.
- Preoperative CPAP/BiPAP use should be documented and the device brought to hospital.
- High OSA severity increases postoperative respiratory monitoring requirements - ICU may be warranted after major abdominal surgery. - Miller's Anesthesia 10e, Harrison's Principles of Internal Medicine 22e
E. Additional Comorbidities
- Hypothyroidism: very common in adults with DS; check TSH. Undertreated hypothyroidism amplifies sensitivity to anesthetics and prolongs emergence.
- Seizure disorder: document and continue anti-epileptics perioperatively.
- Early-onset Alzheimer's dementia (by age 40-50 in many): increases risk of postoperative delirium and cognitive dysfunction; limits use of patient-controlled analgesia.
- Gastrointestinal: higher incidence of GERD - consider aspiration prophylaxis (H2 blocker or PPI, metoclopramide).
- Obesity: common in adults; affects pneumoperitoneum tolerance, positioning, and ventilation.
3. Anesthetic Management
Induction
- Use RSI or modified RSI if GERD present - DS adults have higher aspiration risk.
- Pre-oxygenate well given OSA and reduced FRC from obesity.
- Have video laryngoscope (e.g., GlideScope) as the primary intubation device.
- Use a smaller ETT size than expected (e.g., 6.0-6.5 mm cuffed in adults with suspected subglottic narrowing).
- Maintain in-line cervical spine stabilization throughout laryngoscopy if AAI risk.
- Avoid air bubbles in IV lines if intracardiac shunts are present (paradoxical air embolism).
Maintenance
- Pneumoperitoneum with CO2 at 12-14 mmHg - minimize insufflation pressure given potential pulmonary hypertension risk; lower pressures may need to be used if hemodynamic instability.
- Monitor end-tidal CO2 closely (DS adults may not exhale CO2 as efficiently, especially with OSA).
- Steep reverse Trendelenburg positioning (standard for lap chole) - be mindful of cervical spine and hemodynamic effects.
- Use short-acting agents where possible (remifentanil, desflurane/sevoflurane) for quicker emergence and reduced postoperative sedation.
- Muscle relaxation is required; use quantitative neuromuscular monitoring and reverse fully (sugammadex preferred over neostigmine in patients with pulmonary hypertension or high OSA risk).
Postoperative
- Plan for extended recovery monitoring - at least 24 hours of SpO2 and respiratory monitoring.
- Patients with severe OSA: consider step-down unit or ICU after any major surgery or if opioid requirement is high.
- Multimodal analgesia to minimize opioids: ketorolac, acetaminophen, local infiltration of port sites.
- Restart CPAP/BiPAP as soon as tolerated postoperatively.
- Screen for delirium in those with cognitive impairment using validated tools (CAM or similar). - Miller's Anesthesia 10e [PMID 34165727]
4. Surgical Technique - Laparoscopic Cholecystectomy
Port Placement
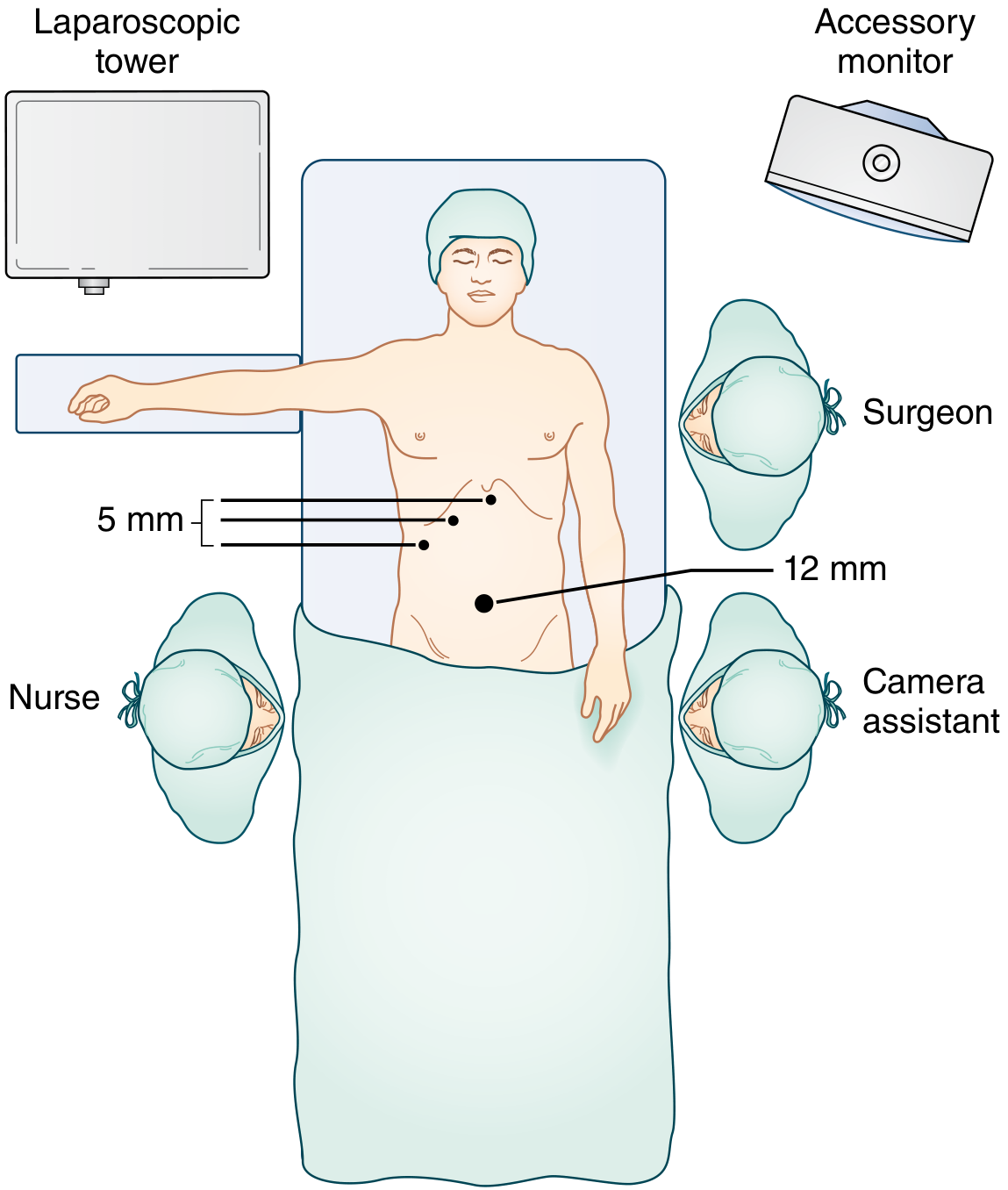
- 12-mm port at/near umbilicus for camera and specimen extraction.
- 5-mm port subxiphoid (instrument access/liver retraction).
- 5-mm port right midclavicular line (grasp infundibulum, retract inferolaterally).
- 5-mm port right anterior axillary line (elevate gallbladder fundus cephalad).
- Patient supine, secured for steep reverse Trendelenburg; one arm tucked for potential cholangiogram.
- Orogastric tube placed to decompress stomach (especially important in DS adults with macroglossia and higher GERD risk).
Critical View of Safety (CVS)
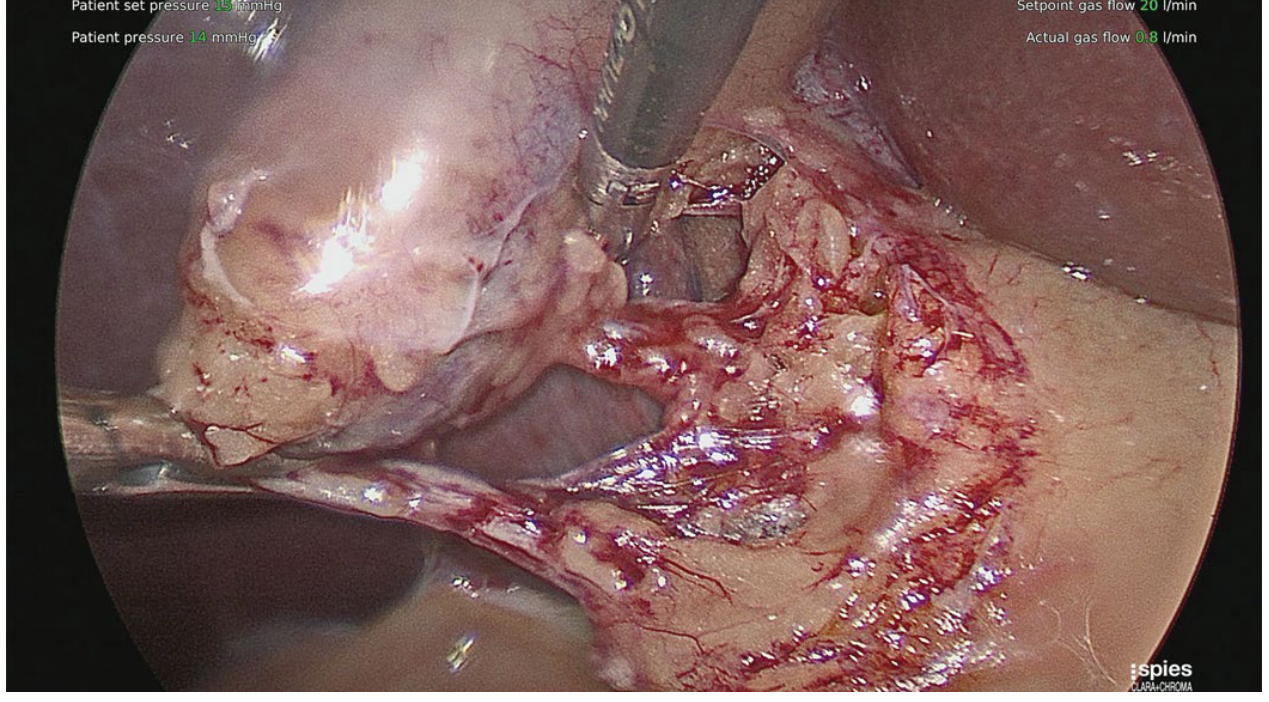
- The hepatocystic triangle must be completely cleared of fat and fibrous tissue.
- The lower one-third of the gallbladder must be dissected free from the liver cystic plate.
- Only two structures should be seen entering the gallbladder - the cystic duct and cystic artery.
Clipping and Division
- Place two clips proximally and one distally on cystic duct; two clips on cystic artery.
- Transect between clips.
- Dissect gallbladder off liver bed with electrocautery; achieve meticulous hemostasis.
- Remove specimen via umbilical port in a retrieval bag. Inspect for any spilled stones and retrieve them (prevent late perihepatic abscesses).
Intraoperative Cholangiography (IOC)
- Routine IOC is not universally required.
- Selective indications: gallstone pancreatitis, unclear or anomalous biliary anatomy, suspected choledocholithiasis, difficult dissection.
- Down syndrome patients may have GI anatomic variants (e.g., prior Duodenal stenosis repair, Hirschsprung's remnants); review imaging carefully preoperatively. - Sabiston Textbook of Surgery
Fluorescent Cholangiography (ICG)
- Near-infrared fluorescent cholangiography using indocyanine green (ICG) is an increasingly used adjunct to enhance real-time biliary visualization and reduce bile duct injury risk - particularly valuable when anatomy is unclear.
5. Key Down Syndrome - Specific Surgical Points
| Concern | Implication |
|---|---|
| Macroglossia + short neck | Airway priority; use smaller ETT, video laryngoscopy |
| Atlantoaxial instability | Cervical spine X-rays preop; in-line stabilization during intubation and positioning |
| CHD / Pulmonary hypertension | Echo preop; minimize pneumoperitoneum pressure; avoid hypoxia/hypercarbia |
| OSA + obesity | Extended recovery monitoring; CPAP postop; low-opioid analgesia |
| Hypothyroidism | Check TSH; delayed emergence if undertreated |
| Cognitive impairment / dementia | Delirium risk; family/carer involvement in perioperative communication |
| GERD | RSI induction; NG/OG tube decompression intraop |
| Cooperation / consent | Assess decision-making capacity; involve guardian if needed; pre-admission familiarization visit may reduce anxiety |
6. Published Evidence
- Perioperative care of adults with Down syndrome (Malinzak, Can J Anaesth 2021) - Comprehensive narrative review of anesthetic management for adults with DS including preop assessment, intraop management, and postop care.
- Anesthetic considerations for adults with Down syndrome + CHD undergoing noncardiac surgery (Aboud et al., J Cardiothorac Vasc Anesth 2023) - Systematic approach for the subgroup with concurrent CHD.
- Lap repair of Morgagni hernia + cholecystectomy in a 40-year-old with Down's syndrome (De Paolis et al., Minerva Chir 2007) - Direct case report of combined laparoscopic abdominal surgery in a DS adult, supporting feasibility and safety with appropriate preparation.
Create a pre-anesthesia checklist (PDF) for DS adult cholecystectomy
ls -la /home/daytona/workspace/ 2>/dev/null || echo "workspace not found"
mkdir -p /home/daytona/workspace/ds-cholecystectomy-checklist
~/ds-cholecystectomy-checklist/generate_checklist.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.units import mm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_RIGHT
from reportlab.platypus import Flowable
import os
OUTPUT = "/home/daytona/workspace/ds-cholecystectomy-checklist/DS_Adult_Cholecystectomy_PreAnesthesia_Checklist.pdf"
# ─── Colour Palette ─────────────────────────────────────────────────────────
TEAL = colors.HexColor("#1A6B72") # main header bg
TEAL_LIGHT = colors.HexColor("#E8F4F5") # alt row tint
ORANGE = colors.HexColor("#E8640A") # alert/critical accent
ORANGE_LITE = colors.HexColor("#FFF3EC") # alert bg
GREY_DARK = colors.HexColor("#2C2C2C")
GREY_MID = colors.HexColor("#5A5A5A")
GREY_LIGHT = colors.HexColor("#F4F4F4")
WHITE = colors.white
DIVIDER = colors.HexColor("#B0D4D7")
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=14*mm, rightMargin=14*mm,
topMargin=12*mm, bottomMargin=12*mm,
)
W = A4[0] - 28*mm # usable page width
styles = getSampleStyleSheet()
# ─── Custom Styles ───────────────────────────────────────────────────────────
def S(name, **kw):
return ParagraphStyle(name, **kw)
TITLE_STYLE = S("DocTitle",
fontSize=17, textColor=WHITE, fontName="Helvetica-Bold",
leading=22, spaceAfter=1, alignment=TA_CENTER)
SUBTITLE_STYLE = S("DocSubtitle",
fontSize=10, textColor=colors.HexColor("#B2E0E4"),
fontName="Helvetica", leading=13, alignment=TA_CENTER)
SECTION_HDR = S("SectionHdr",
fontSize=9.5, textColor=WHITE, fontName="Helvetica-Bold",
leading=12, alignment=TA_LEFT, leftIndent=4)
ITEM_STYLE = S("Item",
fontSize=8.5, textColor=GREY_DARK, fontName="Helvetica",
leading=12, leftIndent=4, spaceAfter=0)
ITEM_BOLD = S("ItemBold",
fontSize=8.5, textColor=GREY_DARK, fontName="Helvetica-Bold",
leading=12, leftIndent=4, spaceAfter=0)
ALERT_STYLE = S("Alert",
fontSize=8, textColor=colors.HexColor("#7A2500"),
fontName="Helvetica-Bold", leading=11, leftIndent=4)
FOOTER_STYLE = S("Footer",
fontSize=7, textColor=GREY_MID, fontName="Helvetica",
leading=9, alignment=TA_CENTER)
NOTE_STYLE = S("Note",
fontSize=7.8, textColor=GREY_MID, fontName="Helvetica-Oblique",
leading=10, leftIndent=4)
PATIENT_LABEL = S("PatientLabel",
fontSize=8, textColor=GREY_MID, fontName="Helvetica",
leading=10)
PATIENT_FIELD = S("PatientField",
fontSize=8.5, textColor=GREY_DARK, fontName="Helvetica-Bold",
leading=11)
# ─── Helper: checkbox row ────────────────────────────────────────────────────
def cb(text, indent=0, bold=False, note=None):
"""Returns a row for the checklist table: [checkbox, text, result field]"""
sty = ITEM_BOLD if bold else ITEM_STYLE
main = Paragraph(text, sty)
rows = [[
Paragraph("☐", S("cb", fontSize=10, fontName="Helvetica",
leading=12, textColor=TEAL)),
main,
Paragraph("", ITEM_STYLE)
]]
if note:
rows.append([
Paragraph("", ITEM_STYLE),
Paragraph(note, NOTE_STYLE),
Paragraph("", ITEM_STYLE)
])
return rows
def cb_result(text, result_label="Result:", bold=False, note=None):
sty = ITEM_BOLD if bold else ITEM_STYLE
rows = [[
Paragraph("☐", S("cb2", fontSize=10, fontName="Helvetica",
leading=12, textColor=TEAL)),
Paragraph(text, sty),
Paragraph(result_label + " ______________________", NOTE_STYLE)
]]
if note:
rows.append([
Paragraph("", ITEM_STYLE),
Paragraph(note, NOTE_STYLE),
Paragraph("", ITEM_STYLE)
])
return rows
def section_table(items_rows, col_widths=None):
"""Build a bordered checklist table from rows."""
if col_widths is None:
col_widths = [6*mm, W*0.62, W*0.31]
all_rows = []
for r in items_rows:
all_rows.extend(r)
t = Table(all_rows, colWidths=col_widths, repeatRows=0)
n = len(all_rows)
style_cmds = [
("VALIGN", (0, 0), (-1, -1), "TOP"),
("LEFTPADDING", (0, 0), (-1, -1), 3),
("RIGHTPADDING", (0, 0), (-1, -1), 3),
("TOPPADDING", (0, 0), (-1, -1), 3),
("BOTTOMPADDING",(0, 0), (-1, -1), 3),
("ROWBACKGROUNDS", (0, 0), (-1, -1), [WHITE, GREY_LIGHT]),
("BOX", (0, 0), (-1, -1), 0.4, DIVIDER),
("LINEBELOW", (0, 0), (-1, -2), 0.25, DIVIDER),
]
t.setStyle(TableStyle(style_cmds))
return t
def section_header(title, color=TEAL):
data = [[Paragraph(title, SECTION_HDR)]]
t = Table(data, colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), color),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
]))
return t
def alert_box(text):
data = [[Paragraph("⚠ " + text, ALERT_STYLE)]]
t = Table(data, colWidths=[W])
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), ORANGE_LITE),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING",(0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("BOX", (0,0), (-1,-1), 0.8, ORANGE),
]))
return t
# ═══════════════════════════════════════════════════════════════════════════
# DOCUMENT BUILD
# ═══════════════════════════════════════════════════════════════════════════
story = []
# ─── HEADER BANNER ──────────────────────────────────────────────────────────
header_data = [[
Paragraph("PRE-ANESTHESIA ASSESSMENT CHECKLIST", TITLE_STYLE),
]]
header_sub = [[
Paragraph(
"Down Syndrome Adult · Laparoscopic Cholecystectomy · Anesthesiologist Copy",
SUBTITLE_STYLE)
]]
banner = Table(
[
[Paragraph("PRE-ANESTHESIA ASSESSMENT CHECKLIST", TITLE_STYLE)],
[Paragraph("Down Syndrome (Trisomy 21) Adult Patient · Laparoscopic Cholecystectomy", SUBTITLE_STYLE)],
[Paragraph("Anesthesiologist Use Only · Complete 24–48 h Before Scheduled Surgery", SUBTITLE_STYLE)],
],
colWidths=[W]
)
banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), TEAL),
("TOPPADDING", (0,0), (-1,-1), 8),
("BOTTOMPADDING", (0,0), (-1,-1), 8),
("LEFTPADDING", (0,0), (-1,-1), 10),
("ROUNDEDCORNERS", [4]),
]))
story.append(banner)
story.append(Spacer(1, 4*mm))
# ─── PATIENT INFO BAR ───────────────────────────────────────────────────────
pi_data = [[
Paragraph("Patient Name:", PATIENT_LABEL),
Paragraph("_______________________________", PATIENT_FIELD),
Paragraph("DOB:", PATIENT_LABEL),
Paragraph("____________", PATIENT_FIELD),
Paragraph("MRN:", PATIENT_LABEL),
Paragraph("____________", PATIENT_FIELD),
],[
Paragraph("Date of Assessment:", PATIENT_LABEL),
Paragraph("____________", PATIENT_FIELD),
Paragraph("Surgeon:", PATIENT_LABEL),
Paragraph("_______________________________", PATIENT_FIELD),
Paragraph("ASA Class:", PATIENT_LABEL),
Paragraph("____", PATIENT_FIELD),
]]
pi_table = Table(pi_data, colWidths=[30*mm, 45*mm, 18*mm, 28*mm, 18*mm, 28*mm])
pi_table.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "BOTTOM"),
("LEFTPADDING", (0,0), (-1,-1), 2),
("RIGHTPADDING",(0,0), (-1,-1), 2),
("TOPPADDING", (0,0), (-1,-1), 2),
("BOTTOMPADDING",(0,0),(-1,-1), 3),
("LINEBELOW", (0,0), (-1,-1), 0.4, DIVIDER),
("BACKGROUND", (0,0), (-1,-1), GREY_LIGHT),
("BOX", (0,0), (-1,-1), 0.4, DIVIDER),
]))
story.append(pi_table)
story.append(Spacer(1, 4*mm))
# ─── ALERT: DS-SPECIFIC REMINDER ────────────────────────────────────────────
story.append(KeepTogether([
alert_box(
"DS-SPECIFIC ALERT: This patient has Trisomy 21. "
"Anticipate difficult airway (default), screen for atlantoaxial instability, "
"congenital heart disease, pulmonary hypertension, OSA, and hypothyroidism "
"BEFORE proceeding. Do NOT skip cervical spine assessment."
),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 1 — CARDIOVASCULAR
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("1. CARDIOVASCULAR ASSESSMENT"),
section_table([
cb_result("Congenital heart disease (CHD) present?",
result_label="Type:", bold=True,
note="CHD present in ~40% DS adults (AV canal, VSD, ASD most common). If unknown → ECHO mandatory."),
cb("ECG obtained and reviewed",
note="Look for: arrhythmia, RVH (pulmonary HTN), conduction defects"),
cb("Echocardiogram reviewed (within 12 months or ordered if absent)",
bold=True,
note="Assess LVEF, RV pressures, PASP, valve function, residual shunts"),
cb_result("Pulmonary artery systolic pressure (PASP)?",
result_label="PASP: ___ mmHg",
note="PASP >40 mmHg = significant pulmonary HTN → Cardiology consult mandatory; "
"lower pneumoperitoneum pressure ≤10 mmHg intraop; avoid hypoxia/hypercarbia"),
cb("Cardiology consult obtained (if CHD or PASP >40 mmHg or unrepaired defect)"),
cb_result("Current cardiac medications",
result_label="Meds:", bold=False,
note="Continue most cardiac meds morning of surgery. Hold ACEi/ARB if instructed."),
cb("Air bubble protocol ordered (if intracardiac shunt present)",
note="All IV lines must be meticulously de-aired; use inline filter"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 2 — AIRWAY (DIFFICULT AIRWAY DEFAULT)
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("2. AIRWAY ASSESSMENT — TREAT AS DIFFICULT AIRWAY UNTIL PROVEN OTHERWISE", color=ORANGE),
section_table([
cb("Mallampati class recorded", bold=True),
cb_result("Mouth opening (inter-incisor distance)",
result_label="mm: ____"),
cb("Macroglossia present? ☐ Yes ☐ No", bold=True),
cb("High-arched palate / midface hypoplasia documented"),
cb_result("Neck circumference / short neck noted",
result_label="Neck circ: ___ cm"),
cb("Subglottic stenosis history or prior intubation difficulty?",
bold=True,
note="Use ETT ≥1 size smaller than predicted by weight/age. Start with 6.0 cuffed in adults."),
cb("Prior anesthesia records reviewed for intubation details",
note="Request previous records; DS patients often have multiple prior GAs"),
cb("Video laryngoscope (GlideScope/C-MAC) confirmed available and checked",
bold=True),
cb("Fiberoptic scope available if anticipated Grade III–IV view"),
cb("Difficult airway cart at bedside before induction"),
cb("ENT/Surgical airway backup arranged for anticipated severe difficulty"),
cb_result("Planned primary airway technique",
result_label="Plan:"),
cb_result("Planned backup (Plan B) airway technique",
result_label="Plan B:"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 3 — CERVICAL SPINE / ATLANTOAXIAL INSTABILITY
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("3. CERVICAL SPINE & ATLANTOAXIAL INSTABILITY (AAI)", color=colors.HexColor("#8B1A1A")),
alert_box(
"AAI occurs in up to 15–20% of DS patients. Unrecognised AAI + aggressive neck "
"flexion during laryngoscopy can cause irreversible tetraplegia."
),
section_table([
cb("Screened for AAI symptoms: neck pain, torticollis, gait change, "
"upper limb weakness, bowel/bladder change",
bold=True),
cb("Lateral flexion-extension cervical X-rays obtained (if symptomatic OR no prior imaging)",
bold=True,
note="Order if: no prior imaging documented, OR any new neurological symptom"),
cb_result("Atlantodens interval (ADI) on X-ray",
result_label="ADI: ___ mm (Normal <5 mm adults)",
note="ADI >5 mm in adults → high-risk; neurosurgery consult before proceeding"),
cb("Neurosurgery consult completed if ADI >5 mm or symptomatic AAI"),
cb("IN-LINE cervical stabilization technique confirmed with assistant for intubation",
bold=True),
cb("Positioning plan for reverse Trendelenburg documented; gentle head movement only"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 4 — RESPIRATORY / OSA
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("4. RESPIRATORY & OBSTRUCTIVE SLEEP APNEA (OSA)"),
section_table([
cb("STOP-BANG score completed", bold=True),
cb_result("Known OSA? ☐ Yes ☐ No CPAP/BiPAP user? ☐ Yes ☐ No",
result_label="CPAP pressure: ___ cmH₂O"),
cb("CPAP/BiPAP device brought to hospital for postop use",
note="Restart CPAP immediately postop when patient is awake and cooperative"),
cb("SpO₂ baseline documented (room air at rest)",
result_label="SpO₂: ___%"),
cb("Chest X-ray reviewed (if respiratory symptoms or new findings)"),
cb_result("Spirometry / PFTs reviewed (if severe OSA, obesity, or known lung disease)",
result_label="FEV1/FVC: ____"),
cb("Postoperative monitoring level agreed: ☐ PACU standard ☐ Step-down ☐ ICU",
bold=True,
note="ICU advised if: PASP >40 mmHg, severe OSA, BMI >40, or significant CHD"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 5 — ENDOCRINE & METABOLIC
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("5. ENDOCRINE & METABOLIC"),
section_table([
cb_result("TSH / thyroid function reviewed",
result_label="TSH: ___ mIU/L",
bold=True,
note="Hypothyroidism common in DS adults → increases anesthetic sensitivity, "
"delays emergence, lowers MAC requirement. Treat before elective surgery."),
cb("Levothyroxine continued morning of surgery (with sip of water)"),
cb_result("Fasting blood glucose on day of surgery",
result_label="BGL: ___ mmol/L"),
cb("Diabetes medications reviewed and adjusted per fasting protocol"),
cb_result("Electrolytes: Na / K / Cr",
result_label="Na:__ K:__ Cr:__ μmol/L"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 6 — NEUROLOGICAL / COGNITIVE
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("6. NEUROLOGICAL & COGNITIVE"),
section_table([
cb("Baseline cognitive function documented (mild / moderate / severe ID)",
bold=True),
cb("Dementia / Alzheimer's disease present? ☐ Yes ☐ No",
note="Early-onset Alzheimer's in DS adults from age ~40. "
"Increases postoperative delirium risk significantly."),
cb("Seizure disorder present? ☐ Yes ☐ No",
note="Document current antiepileptic drugs; continue perioperatively"),
cb_result("Antiepileptic drugs",
result_label="AED:"),
cb("Delirium screening tool agreed (CAM or equivalent) for postop monitoring"),
cb("Guardian / carer identified and informed of consent process",
bold=True),
cb("Pre-admission familiarisation visit offered (reduces procedural anxiety in DS)"),
cb("PCA suitability assessed: ☐ Suitable ☐ Not suitable (cognitive impairment)",
note="If PCA not suitable → nurse-controlled or multimodal analgesia protocol"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 7 — GI / ASPIRATION RISK
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("7. GASTROINTESTINAL & ASPIRATION RISK"),
section_table([
cb("GERD present? ☐ Yes ☐ No Current PPI/H2 blocker? ☐ Yes ☐ No",
bold=True),
cb("Aspiration prophylaxis prescribed (e.g., ranitidine 150 mg OR omeprazole 40 mg night before + morning of surgery)"),
cb("NPO status confirmed: solids ≥6 h, clear fluids ≥2 h",
bold=True),
cb("Rapid sequence induction (RSI) planned if GERD / full stomach / obesity",
bold=True,
note="RSI with succinylcholine or high-dose rocuronium + cricoid pressure"),
cb("Orogastric tube insertion planned for intraoperative gastric decompression"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 8 — ANAESTHETIC PLAN
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("8. ANAESTHETIC PLAN DOCUMENTED"),
section_table([
cb("Induction agent selected (Propofol / Ketamine / Sevoflurane inhalation)",
bold=True),
cb("Neuromuscular blocker selected ☐ Succinylcholine ☐ Rocuronium"),
cb("Reversal agent confirmed available: ☐ Sugammadex (preferred) ☐ Neostigmine",
note="Sugammadex preferred — avoids muscarinic effects; safer in pulmonary HTN"),
cb("Maintenance agent: ☐ Sevoflurane ☐ Desflurane ☐ TIVA",
note="Short-acting agents preferred for quicker emergence"),
cb("Quantitative neuromuscular monitoring (TOF) confirmed",
bold=True),
cb("Pneumoperitoneum pressure target documented: ≤12–14 mmHg standard / ≤10 mmHg if pulm HTN",
bold=True),
cb("End-tidal CO₂ monitoring confirmed — titrate ventilation to EtCO₂ 35–40 mmHg"),
cb("Multimodal analgesia plan: Paracetamol + Ketorolac + Port-site local anesthetic",
note="Minimise opioids given OSA risk"),
cb("Antiemetic prophylaxis: ondansetron ± dexamethasone"),
cb("VTE prophylaxis: LMWH + sequential compression devices"),
cb("Antibiotic prophylaxis given (within 60 min of incision)"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 9 — LABS & INVESTIGATIONS SUMMARY
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("9. REQUIRED INVESTIGATIONS — TICK WHEN REVIEWED"),
section_table(
col_widths=[6*mm, W*0.50, W*0.43],
items_rows=[
cb_result("FBC / CBC", result_label="Hb:___ Plt:___"),
cb_result("Coagulation (PT/INR/APTT)", result_label="INR:___ APTT:___"),
cb_result("U&E / CMP", result_label="Na:__ K:__ Cr:__"),
cb_result("LFTs / liver function", result_label="ALT:__ ALP:__ Bili:__"),
cb_result("TSH", result_label="___ mIU/L"),
cb_result("Blood glucose", result_label="___ mmol/L"),
cb_result("ECG", result_label="Interpretation:"),
cb_result("Echocardiogram", result_label="LVEF:___ PASP:___"),
cb_result("Cervical spine X-ray (if indicated)", result_label="ADI:___ mm"),
cb_result("Chest X-ray (if indicated)", result_label="Findings:"),
cb_result("Abdominal USS / CT report reviewed", result_label="Bile duct diam:___"),
cb_result("Group & Screen / Blood type", result_label="Group:___"),
]),
Spacer(1, 3*mm),
]))
# ════════════════════════════════════════════════════════════════════
# SECTION 10 — FINAL SIGN-OFF
# ════════════════════════════════════════════════════════════════════
story.append(KeepTogether([
section_header("10. FINAL CLEARANCE & SIGN-OFF"),
section_table([
cb("Patient / guardian informed consent obtained and documented",
bold=True),
cb("All critical issues identified above have been addressed or escalated"),
cb("Surgical team briefed on DS-specific risks"),
cb("OT team alerted: difficult airway equipment, cervical in-line stabilisation protocol"),
cb("ICU / HDU bed reserved (if indicated)"),
cb("CPAP device at bedside for postoperative use"),
]),
]))
story.append(Spacer(1, 4*mm))
# ─── Sign-off bar ────────────────────────────────────────────────────────────
signoff_data = [[
Paragraph("Assessed by:", PATIENT_LABEL),
Paragraph("_____________________________", PATIENT_FIELD),
Paragraph("Designation:", PATIENT_LABEL),
Paragraph("___________________", PATIENT_FIELD),
Paragraph("Date / Time:", PATIENT_LABEL),
Paragraph("___________________", PATIENT_FIELD),
]]
so_table = Table(signoff_data, colWidths=[24*mm, 48*mm, 24*mm, 36*mm, 22*mm, 33*mm])
so_table.setStyle(TableStyle([
("VALIGN", (0,0), (-1,-1), "BOTTOM"),
("LEFTPADDING", (0,0), (-1,-1), 2),
("RIGHTPADDING", (0,0), (-1,-1), 2),
("TOPPADDING", (0,0), (-1,-1), 3),
("BOTTOMPADDING",(0,0), (-1,-1), 4),
("BACKGROUND", (0,0), (-1,-1), TEAL_LIGHT),
("BOX", (0,0), (-1,-1), 0.5, TEAL),
]))
story.append(so_table)
story.append(Spacer(1, 4*mm))
# ─── FOOTER ─────────────────────────────────────────────────────────────────
story.append(HRFlowable(width=W, thickness=0.5, color=DIVIDER))
story.append(Spacer(1, 1.5*mm))
story.append(Paragraph(
"References: Miller's Anesthesia 10e · Morgan & Mikhail's Clinical Anesthesiology 7e · "
"Sabiston Textbook of Surgery · Malinzak EB, Can J Anaesth 2021 (PMID 34165727) · "
"Aboud MA et al., J Cardiothorac Vasc Anesth 2023 (PMID 36610856) | "
"This checklist is a clinical aid and does not replace individual clinical judgment.",
FOOTER_STYLE
))
# ─── BUILD ──────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF created: {OUTPUT}")
cd /home/daytona/workspace/ds-cholecystectomy-checklist && python generate_check…
~/ds-cholecystectomy-checklist/generate_checklist.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/ds-cholecystectomy-checklist/generate_checklist.py'
cd /home/daytona/workspace/ds-cholecystectomy-checklist && python generate_check…
ls -lh /home/daytona/workspace/ds-cholecystectomy-checklist/
DS Adult Cholecystectomy PreAnesthesia Checklist
PDF Document · PDF
What's included in the checklist
| Section | Key Content |
|---|---|
| Patient Info Bar | Name, DOB, MRN, Surgeon, ASA class, Date |
| DS Alert Banner | Highlighted warning box at the top reminding of the 5 non-negotiable DS-specific risks |
| 1. Cardiovascular | CHD screen, ECG, ECHO, PASP, air-bubble protocol, cardiology consult trigger |
| 2. Airway | Default difficult airway approach, macroglossia, subglottic stenosis, ETT sizing, video laryngoscope + fiberoptic confirmed, Plan A & B documented |
| 3. Cervical Spine / AAI | Symptom screen, flexion-extension X-ray indication, ADI measurement field, in-line stabilisation plan - highlighted in dark red |
| 4. Respiratory / OSA | STOP-BANG, CPAP details, baseline SpO₂, postop monitoring level decision |
| 5. Endocrine / Metabolic | TSH with action note for hypothyroidism, glucose, electrolytes |
| 6. Neurological / Cognitive | Cognitive baseline, Alzheimer's/dementia, seizures/AEDs, guardian consent, PCA suitability |
| 7. GI / Aspiration | GERD, RSI indication, NPO confirmation, OG tube plan |
| 8. Anaesthetic Plan | Induction agent, NMB, reversal (sugammadex preferred), pneumoperitoneum pressure target, multimodal analgesia, VTE, antibiotics |
| 9. Investigations Summary | All required labs with write-in result fields |
| 10. Sign-off | Final clearance, team briefing, ICU reservation, countersignature line |
Search for DS-specific anesthesia complications literature and case reports
"Down syndrome"[MeSH Terms] AND anesthesia AND complications
"Down syndrome"[MeSH Terms] AND airway AND intubation
"Down syndrome" AND "atlantoaxial" AND anesthesia
"Down syndrome" AND "pulmonary hypertension" AND surgery
Down syndrome anesthesia complications case reports perioperative adverse events adults
PMID: 35156260
PMID: 30207016
PMID: 30262364
PMID: 36716257
PMID: 39503133
"Down syndrome" AND bradycardia AND anesthesia
PMID: 20736433
PMID: 40376277
PMID: 26749540
PMID: 17315425
PMID: 15835829
https://ndss.org/resources/surgery-down-syndrome
"Down syndrome" AND "postoperative" AND (delirium OR cognitive OR respiratory)
PMID: 34165727
DS-Specific Anesthesia Complications: Literature Review
1. Induction Bradycardia - The Most Quantified Complication
Incidence Data
-
In a large cohort study of DS patients having non-cardiac procedures, the complication rate for severe bradycardia was 3.6%, airway obstruction 1.8%, post-intubation stridor 1.8%, and bronchospasm 0.4%. Difficult intubation occurred in 0.5%. (Borland et al., cited in Steward review)
-
A landmark retrospective cohort of 209 DS children vs 268 controls undergoing sevoflurane induction showed DS was an independent risk factor for bradycardia on multivariate analysis - even when controlling for CHD and ASA class. The association held whether or not the patient had known heart disease.
- [Kraemer FW et al., Anesth Analg 2010, PMID 20736433]
-
The NDSS reports that up to 50% of DS patients may exhibit bradycardia during induction - some deteriorating to asystole. The risk is highest in children but remains significant across all ages including adults. (ndss.org/resources/surgery-down-syndrome)
Mechanism - NEW 2024 Evidence
- 58% of DS children (54/93) became bradycardic within 300 seconds of sevoflurane induction, vs 22% of typically developing controls (22/102).
- Bradycardia and hypotension were statistically associated with sympathetic nervous system failure - an inability to mount the normal compensatory sympathetic response to the vasodilatory effects of sevoflurane.
- Sympathetic failure was identified as a modifiable target - suggesting that pre-treatment with sympathomimetics (atropine, ephedrine, glycopyrrolate) before induction may be preventive.
- [Sinton JW et al., J Pediatr Res 2024, PMID 40376277]
Autonomic Dysfunction as the Unifying Framework
- [Sinton JW et al., Paediatr Anaesth 2022, PMID 35156260]
2. Atlantoaxial & Atlantooccipital Instability - Catastrophic but Preventable
Systematic Review: 16 Cases of Iatrogenic Tetraplegia
- Injuries occurred during: intubation for non-ENT surgery (9 cases), ENT surgery (3 cases), sedation for neuroimaging (1), physical restraint (1), and intraoperative head positioning (2).
- Preoperative screening was reported in only 4 of 16 cases.
- No cases resolved spontaneously. Two patients progressed to brain death, 12 required surgical stabilization (7 improved, 1 died later).
- Diagnosis was delayed by a median of 30 days after symptom onset (range 11.5-912.5 days).
- No intraoperative precautions were reported in any of the 16 index procedures.
- [Husnudinov RE et al., Int J Pediatr Otorhinolaryngol 2018 - Systematic Review, Tier 1 - PMID 30262364]
The Screening Dilemma
-
Bertolizio et al., 2018: "The Eternal Gamble" - a combined case report + review in Paediatric Anaesthesia that directly confronts the clinical dilemma: up to 30% of Trisomy 21 patients have atlanto-axial or atlanto-occipital instability radiologically, but only 1-2% are symptomatic. Dynamic cervical X-rays are the most common screening tool but "no conclusive recommendations have been forthcoming." Many anesthesiologists proceed without pre-op imaging. The review proposes practical recommendations for clinical practice.
- [Bertolizio G et al., Paediatr Anaesth 2018, PMID 30207016]
-
Harley & Collins, 1994: The foundational case series on neurologic sequelae from AAI during ENT surgery - still heavily cited. Documented permanent cord injury after routine ENT procedures.
- [Harley EH, Collins MD, Arch Otolaryngol 1994, PMID 8297573]
3. Airway Complications
Tracheal Stenosis - Under-recognised
- Resistance was felt while advancing the ETT past the vocal cords.
- On a second GA 2 years later, pre-operative 3D CT tracheal mapping was used to define the stenosis and plan airway management without advancing the tube over the narrowing.
- The case highlights that tracheal bronchus, airway malacia, and subglottic/tracheal stenosis are under-appreciated lower airway anomalies in DS (prevalence ~71% vs ~32% in controls in one cohort study).
- [Ujita T et al., Anesth Prog 2024, PMID 39503133]
Airway Size Data
- Shott's Laryngoscope 2000 study provides anatomical measurements showing DS patients have smaller subglottic diameters than age/weight-matched controls, guiding ETT sizing recommendations.
- [Shott SR, Laryngoscope 2000, PMID 10764002]
Prevalence of Airway Problems
- Hamilton et al. (2016) found a high prevalence of anatomical airway problems in children with DS: laryngomalacia, subglottic stenosis, tracheal bronchus, and lingual tonsil hypertrophy - all of which persist or worsen into adulthood in many patients.
- [Hamilton J et al., Int J Pediatr Otorhinolaryngol 2016, PMID 26810279]
Tracheal Morphology (2024 New Data)
- [Fockens MM et al., Laryngoscope 2024, PMID 38676421]
4. Cardiovascular Complications
Comprehensive 2023 Consensus (Circulation)
- CHD present in up to 50% of DS patients; the most common forms are complete atrioventricular canal (AVSD), VSD, and ASD.
- DS patients develop pulmonary arterial hypertension at higher rates and at lower ages than the general population, even without CHD - likely driven by upper airway obstruction, OSA, and altered pulmonary vascular reactivity.
- Eisenmenger syndrome (irreversible pulmonary HTN from long-standing shunt) has historically been common in DS and is a major driver of perioperative mortality.
- Adults with DS have significantly higher perioperative cardiac arrest rates and syncope than age-matched non-DS adults undergoing similar procedures.
- The review identifies disparities in cardiovascular care for DS patients - they are less often referred for timely cardiac evaluation.
- [Dimopoulos K et al., Circulation 2023, PMID 36716257]
Cardiovascular Disease Spectrum in DS Adults
- [Versacci P et al., Curr Opin Pediatr 2018, PMID 30015688]: Reviews the evolving cardiovascular disease burden in DS adults - emphasizing that repaired CHD, residual lesions, and late-onset pulmonary HTN create a complex cardiac profile requiring specialist input before non-cardiac surgery.
Pneumoperitoneum + Pulmonary Hypertension
- [Hofland J et al., Br J Anaesth 2001, PMID 11573602]
5. Opioid Sensitivity & Altered Pharmacodynamics
- Post-mortem studies show abnormal concentrations of endogenous opioids in the cortex of DS patients.
- Structural and functional alterations of mu, delta, and kappa receptors are hypothesized.
- Practical implication: DS patients may show unpredictable opioid responses - either enhanced sensitivity (risk of respiratory depression) or altered pain expression. Dose titration with careful monitoring is essential. PCA may not be suitable for those with significant cognitive impairment.
- [Mafrica F, Fodale V, J Opioid Manag 2006, PMID 17315425]
6. Postoperative Complications
Infectious & Respiratory
- The Malinzak 2021 review (PMID 34165727) documents that DS adults have higher rates of postoperative pneumonia, aspiration pneumonitis, and urinary tract infections than the general population, leading to longer hospital stays and increased infection-related mortality with age.
Cognitive/Delirium
- Early-onset Alzheimer's (affects most DS patients over 50) dramatically increases postoperative delirium risk.
- Standard CAM-ICU tools may be less sensitive in DS patients with baseline cognitive impairment - need to establish and document baseline cognitive function preoperatively.
DVT
- DS adults typically have low functional status and sedentary lifestyles → increased perioperative DVT risk. Sequential compression devices + LMWH are mandatory.
Difficult IV Access
- Obesity combined with xerodermia (dry, thickened skin characteristic of DS) can make IV cannulation extremely difficult, delaying drug delivery and causing procedural distress. Ultrasound-guided IV insertion should be available.
7. Comprehensive Review Articles to Know
| Evidence | Year | Key Contribution | PMID |
|---|---|---|---|
| Systematic Review (Tier 1) | 2018 | 16 cases iatrogenic tetraplegia; no spontaneous resolution | 30262364 |
| Scoping Review + Consensus (Circulation) | 2023 | Cardiovascular complications full spectrum, disparities in care | 36716257 |
| Narrative Review (adults) | 2021 | Perioperative care of DS adults; comorbidity progression with aging | 34165727 |
| Review (DS + CHD noncardiac) | 2023 | Systematic approach for DS + CHD undergoing noncardiac surgery | 36610856 |
| Review (ANS) | 2022 | Autonomic dysfunction as unifying mechanism for bradycardia, hypotonia, airway obstruction | 35156260 |
| Review + Case Report (AAI) | 2018 | The screening dilemma; 30% radiologic AAI, 1-2% symptomatic | 30207016 |
| Review (preop eval) | 2016 | Comprehensive DS-specific risk stratification framework | 26749540 |
| Cohort study (bradycardia) | 2010 | DS = independent risk factor for induction bradycardia with sevoflurane | 20736433 |
| Prospective (bradycardia mechanism) | 2024 | Sympathetic failure mechanism; 58% bradycardia incidence | 40376277 |
| Case Report (tracheal stenosis) | 2024 | Tracheal stenosis found at intubation; 3D CT planning for next GA | 39503133 |
| Review (opioids) | 2006 | Altered opioid receptor system in DS brain | 17315425 |
| Case Report (lap chole + DS) | 2007 | Lap chole + Morgagni hernia repair in 40-year-old DS man; successful | 17519846 |
Key Take-Aways for the Cholecystectomy Setting
-
Bradycardia is the most common DS-specific induction complication - occurs in 3.6-58% depending on the study and definition. Mechanism is sympathetic failure. Have atropine ready; consider prophylactic glycopyrrolate; favour TIVA if high cardiac risk.
-
AAI-related tetraplegia is rare but irreversible - 16 documented iatrogenic cases, 2 resulting in brain death. No precautions were documented in any of them. Systematic review supports treating every DS patient as potentially at risk, regardless of prior imaging.
-
Pulmonary hypertension + pneumoperitoneum is the most specific cholecystectomy risk in this population. Titrate insufflation pressure, monitor EtCO2 vigilantly, have a plan for acute RV failure.
-
Tracheal/subglottic stenosis may not be known preoperatively - resistance on tube advancement is the first sign. Always have a smaller ETT available (6.0 and 5.5 mm cuffed).
-
Opioid pharmacodynamics are altered - use multimodal analgesia, avoid opioid-dominant regimens, titrate carefully.
-
Postoperative period carries specific risks: OSA-related respiratory events, delirium in those with dementia, pneumonia/aspiration, DVT from sedentary baseline.