Bph from surgery standard book
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer from Bailey & Love's Short Practice of Surgery (28th edition) - the standard surgery textbook. Here is the full write-up:
Benign Prostatic Hyperplasia (BPH)
Source: Bailey and Love's Short Practice of Surgery, 28th Edition (Chapter 84) & Sabiston Textbook of Surgery
Aetiology
- Occurs in men over 50 years; by age 60, 50% have histological BPH
- Most common cause of bladder outflow obstruction (BOO) in men >70 years
- Hormonal theory: declining testosterone with relatively preserved oestrogen levels promotes growth; intermediate peptide growth factors also play a role
- Metabolic syndrome and hereditary factors are also implicated
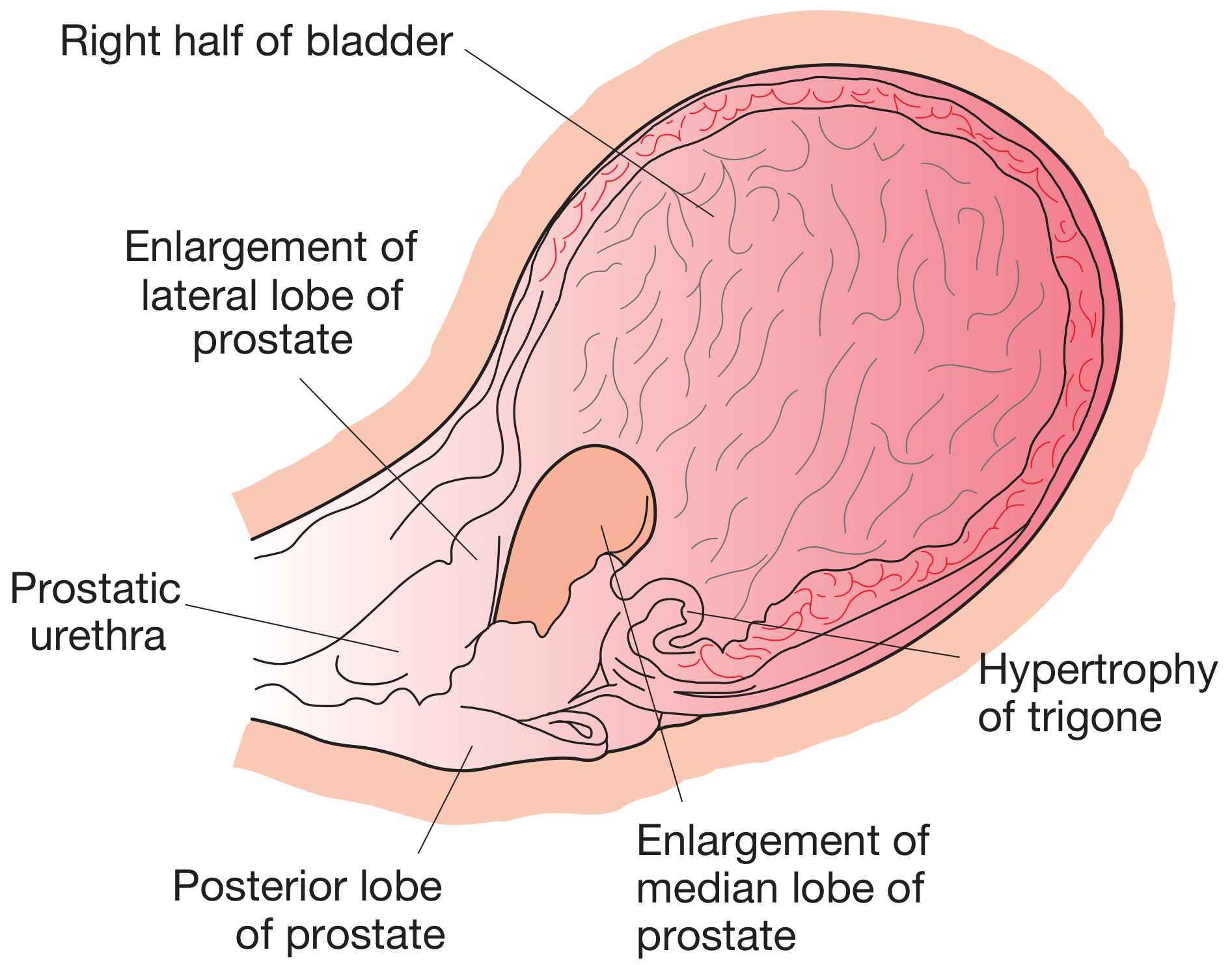
Pathology
BPH affects both glandular epithelium and connective tissue stroma. It typically affects the submucous glands of the transitional (periurethral) zone, forming nodular enlargements. This overgrowth compresses the peripheral zone glands into a false capsule, creating the appearance of "lateral lobes."
When the central zone glands are involved, a middle lobe develops projecting up into the bladder within the internal sphincter.
Effects of BPH
On the Urethra
- Prostatic urethra is lengthened (sometimes doubled), but not narrowed anatomically
- Posterior curve may be so exaggerated that a curved catheter is needed
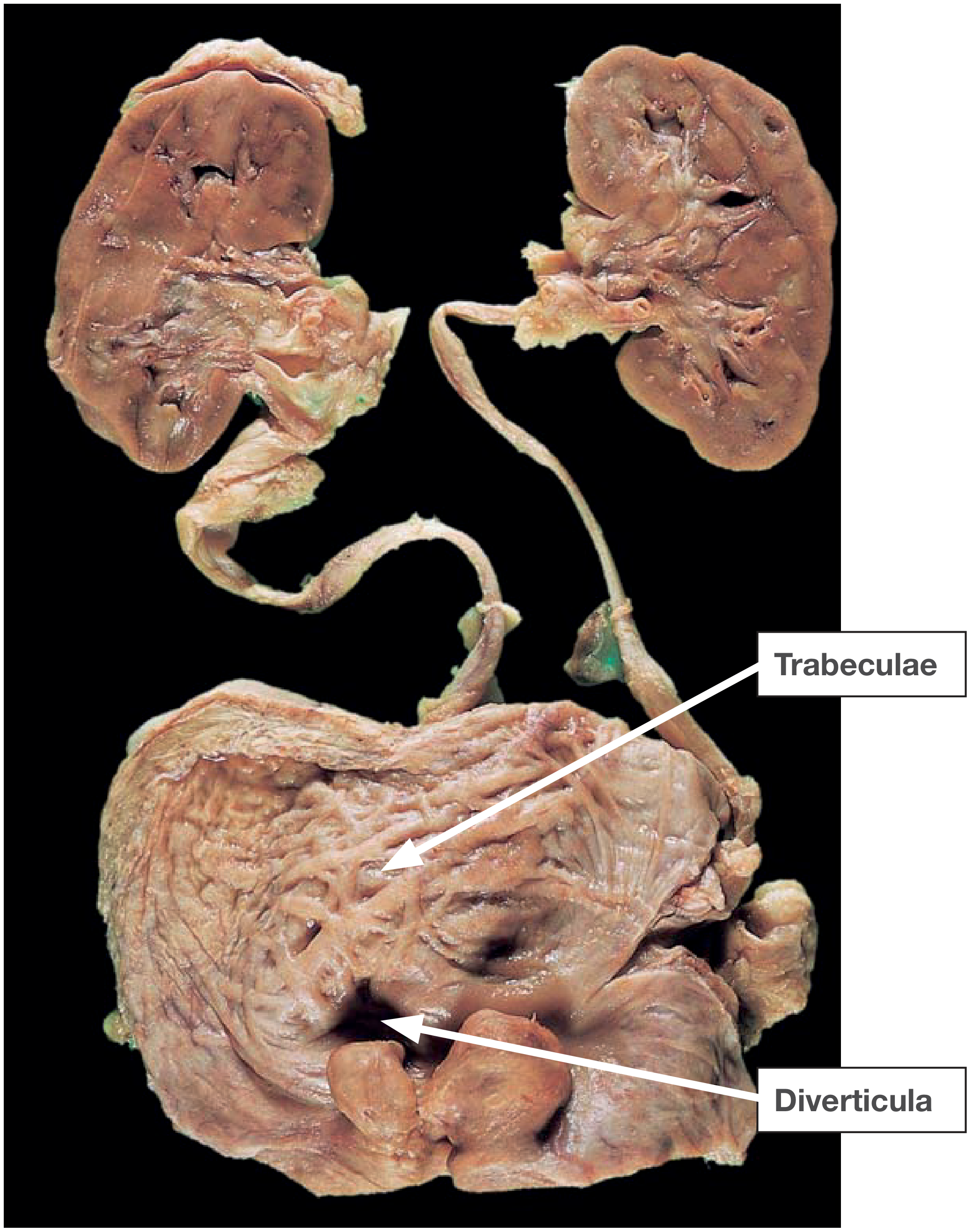
On the Bladder
- If BOO results, bladder musculature hypertrophies - appears trabeculated
- Increased blood flow - veins at base of bladder may cause haematuria
Consequences of BPH (Summary Box 84.2)
| Scenario |
|---|
| No symptoms, no BOO |
| No symptoms, but urodynamic evidence of BOO |
| LUTS with no evidence of BOO |
| LUTS and BOO |
| Complications: acute/chronic retention, haematuria, UTI, stone formation |
Lower Urinary Tract Symptoms (LUTS)
Voiding (Obstructive) Symptoms
- Hesitancy (worse if bladder very full)
- Poor flow (unimproved by straining)
- Intermittent stream (stops and starts)
- Dribbling (including post-micturition)
- Sensation of poor bladder emptying
- Episodes of near retention
Storage (Irritative) Symptoms
- Frequency
- Nocturia
- Urgency
- Urge incontinence
Complications of BOO
- Acute retention - sometimes the first presentation
- Chronic retention - residual volume >250 mL leads to high-pressure chronic retention, bilateral hydronephrosis, upper tract infection, and renal impairment; presents with overflow incontinence, enuresis, renal insufficiency
- Urinary infection and calculi - from impaired bladder emptying
- Post-obstructive diuresis - after catheter release in uraemic chronic retention (loss of tubular reabsorption due to chronic back pressure)
Investigations
Urinary Flow Rates
| Peak Flow Rate | Interpretation |
|---|---|
| >15 mL/s (voided vol >200 mL) | Normal |
| 10-15 mL/s | Equivocal |
| <10 mL/s | Low (obstructed) |
Voiding Pressures (Urodynamics)
| Pressure | Interpretation |
|---|---|
| >80 cmH2O | High (obstructed) |
| 60-80 cmH2O | Equivocal |
| <60 cmH2O | Normal |
Other Investigations
- Urine: dipstick (glucose, leucocyte esterase, blood), MSU for culture; cytology if CIS suspected
- Blood: serum creatinine, electrolytes, haemoglobin; PSA in appropriate patients (life expectancy >10 years)
- Imaging: Ultrasound for post-void residual; upper tract imaging (USS/CT urography) if haematuria or infection present
- Cystourethroscopy: done immediately before prostatectomy to exclude urethral stricture, bladder carcinoma, non-opaque vesical calculus
- Pressure-flow urodynamics: for suspected neuropathy, dominant irritative symptoms, borderline flow rates, young men (<50) or elderly (>80)
- IPSS (International Prostate Symptom Score): validated questionnaire used to quantify symptom severity
Management
Strong Indications for Surgery (Prostatectomy)
- Acute retention in fit men (accounts for ~25% of prostatectomies)
- Chronic retention with renal impairment - residual urine ≥200 mL + hydronephrosis/uraemia (accounts for ~15%)
- Complications of BOO - stones, infection, diverticulum formation
- Recurrent haematuria from a very vascular prostate
Treatment Options (Summary Box 84.4)
1. Conservative (Watchful Waiting)
- Fluid manipulation (avoid fluid bingeing and late-night intake)
- Reduce caffeine and alcohol intake
- Suitable for mild symptoms
2. Medical (Drug) Therapy
| Drug Class | Drugs | Mechanism | Side Effects |
|---|---|---|---|
| Alpha-1 blockers | Tamsulosin 0.4 mg OD, Alfuzosin 10 mg OD, Doxazosin 1-8 mg, Terazosin 1-10 mg, Silodosin 4-8 mg | Relax smooth muscle of bladder neck and prostate | Postural hypotension, retrograde ejaculation, rhinitis |
| 5α-reductase inhibitors | Finasteride, Dutasteride | Block testosterone → DHT conversion; reduce prostate volume by ~25-30%; reduce PSA by ~50% | Impotence, decreased libido |
| Combination therapy | Alpha-blocker + 5α-RI | Better outcomes for glands >35 g | - |
| PDE5 inhibitors | Tadalafil | Used for BPH-LUTS with or without ED | - |
3. Surgical/Interventional Therapy
| Procedure | Notes |
|---|---|
| TURP (Transurethral Resection of Prostate) | Gold standard; diathermy loop removes prostatic tissue transurethrally |
| HoLEP (Holmium Laser Enucleation) | Preferred for large glands; lower re-operation rate |
| Open/Robotic Simple Prostatectomy | For very large glands (>80-100 g) |
| Retropubic prostatectomy (Millin's) | Open approach |
| Transvesical prostatectomy | Through the bladder |
| PAE (Prostate Artery Embolisation) | Minimally invasive; growing evidence |
| Rezum (Water Vapour Treatment) | Minimally invasive |
| Urolift (Prostatic Urethral Lift) | Minimally invasive; good for men wishing to preserve ejaculatory function |
| Aquablation (Water Jet) | Minimally invasive |
TURP - Key Facts
- Resectoscope inserted transurethrally; electric current via diathermy loop resects tissue
- Success rate: 90% for urodynamically proven BOO; only 65% for mild symptoms or weak detrusor
- Mortality: <0.5%
- Retrograde ejaculation: 75-80%
- Erectile dysfunction: 5-10%
- Incontinence: ~1%
- Severe sepsis: ~6%
- Severe haematuria requiring transfusion: ~3%
- Re-operation rate: ~15% after 8-10 years
- TURP syndrome: dilutional hyponatraemia from absorption of hypotonic irrigating fluid - now largely avoided with bipolar/saline-based systems
Chronic Retention - Special Considerations
- Uraemic patients must have urgent catheterisation before surgery - wait at least 6 weeks for renal function to recover before prostatectomy
- Risk of post-obstructive diuresis after catheter placement - requires careful IV fluid replacement (0.45% saline or D5W based on urine output)
- Haematuria commonly follows catheterisation due to bladder/upper tract decompression - usually settles within days
Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 84 | Sabiston Textbook of Surgery, Chapter 121
Achalasia cardia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the material needed for a comprehensive answer. Let me compile the complete response:
Achalasia Cardia
Source: Bailey and Love's Short Practice of Surgery, 28th Edition (Chapter 66) + Sleisenger & Fordtran's GI and Liver Disease
Definition and Aetiology
The term achalasia originates from the Greek "khalasis" meaning "failure to relax." It is an uncommon primary oesophageal motility disorder with a prevalence of 1.8-12.6 per 100,000 persons per year.
Pathophysiology:
- Loss of inhibitory ganglion cells in the myenteric (Auerbach's) plexus of the oesophagus
- Postulated mechanism: virus-induced autoimmune destruction (evidence points to latent HSV-1 infection in genetically susceptible individuals with specific HLA alleles)
- Histology shows reduced ganglion cells with variable chronic inflammatory infiltrate (predominantly cytotoxic T cells)
- Key neurotransmitter deficit: loss of inhibitory neurons (NO and VIP) that mediate LOS relaxation and propagated peristalsis
- The excitatory cholinergic pathway is partially preserved, which explains why botulinum toxin has some effect
Result: Mismatch between excitatory and inhibitory activity → failure of LOS relaxation + absent peristalsis → progressive oesophageal dilatation → oesophagus empties only by hydrostatic pressure (incomplete) → food retention and fermentation
Secondary causes (pseudo-achalasia):
- Chagas disease - Trypanosoma cruzi destroys the myenteric plexus (South America)
- Cancer of the gastric cardia - must always be excluded
- Allgrove syndrome - rare genetic triad of familial adrenal insufficiency, alacrima, and achalasia
Chicago Classification (HRM Types)
Achalasia is classified by High-Resolution Manometry (HRM) using the Chicago Classification 4.0 based on the Integrated Relaxation Pressure (IRP) and oesophageal body pressurisation pattern:
| Type | Manometry Pattern | Clinical Features | Response to Treatment |
|---|---|---|---|
| Type I (Classic) | Elevated IRP + aperistalsis + no pressurisation | Dilated oesophagus, minimal contractions | Moderate response |
| Type II | Elevated IRP + pan-oesophageal pressurisation (>20% swallows) | Best prognosis | Best response to all treatments |
| Type III (Spastic) | Elevated IRP + premature/spastic contractions (>20% swallows) | Chest pain prominent | Poorest response; needs extended myotomy |
- Degree of ganglion cell loss parallels disease duration: likely progression from EGJ outflow obstruction → Type II → Type I → end-stage achalasia (megaoesophagus)
- Type III has unique pathogenesis - myenteric inflammation + altered function, without destruction
Clinical Features
Most commonly diagnosed between 30-60 years of age.
Symptoms
- Dysphagia (to both solids AND liquids - hallmark distinguishing from mechanical obstruction) - gradual onset, often present for years
- Regurgitation - nonbilious, nonacid, mixed with saliva; food from hours/days previously
- Retrosternal chest pain / odynophagia - common early, especially in type III; may improve spontaneously
- Heartburn - paradoxically common; actually due to fermentation of retained food (not true acid reflux)
- Halitosis - from fermentation of food residues
- Weight loss - variable; patients often adapt diet to maintain weight
- Aspiration pneumonia / respiratory symptoms - up to 10% with advanced disease
Eckardt Score (Clinical Severity Scoring)
| Score | Weight Loss (kg) | Dysphagia | Retrosternal Pain | Regurgitation |
|---|---|---|---|---|
| 0 | None | None | None | None |
| 1 | <5 | Occasionally | Occasionally | Occasionally |
| 2 | 5-10 | Daily | Daily | Daily |
| 3 | >10 | Each meal | Each meal | Each meal |
Total score 0-3 = remission; >3 = treatment failure. Maximum score = 12.
Diagnosis
1. Endoscopy (OGD)
- Frothy saliva pooling in oesophagus
- Food residue in oesophagus
- Oesophagus dilated or tortuous
- OGJ appears tight/spastic but usually allows scope passage with gentle pressure
- 30-40% of endoscopies are normal - does not exclude achalasia
- Critical to exclude pseudo-achalasia (carcinoma of gastric cardia)
2. Barium Contrast Study (Barium Swallow)
Classic findings:
- Dilatation of oesophageal body
- Abnormal/absent peristaltic contractions
- "Bird's beak" / "Rat's tail" appearance - smooth tapering at the distal oesophagus/OGJ
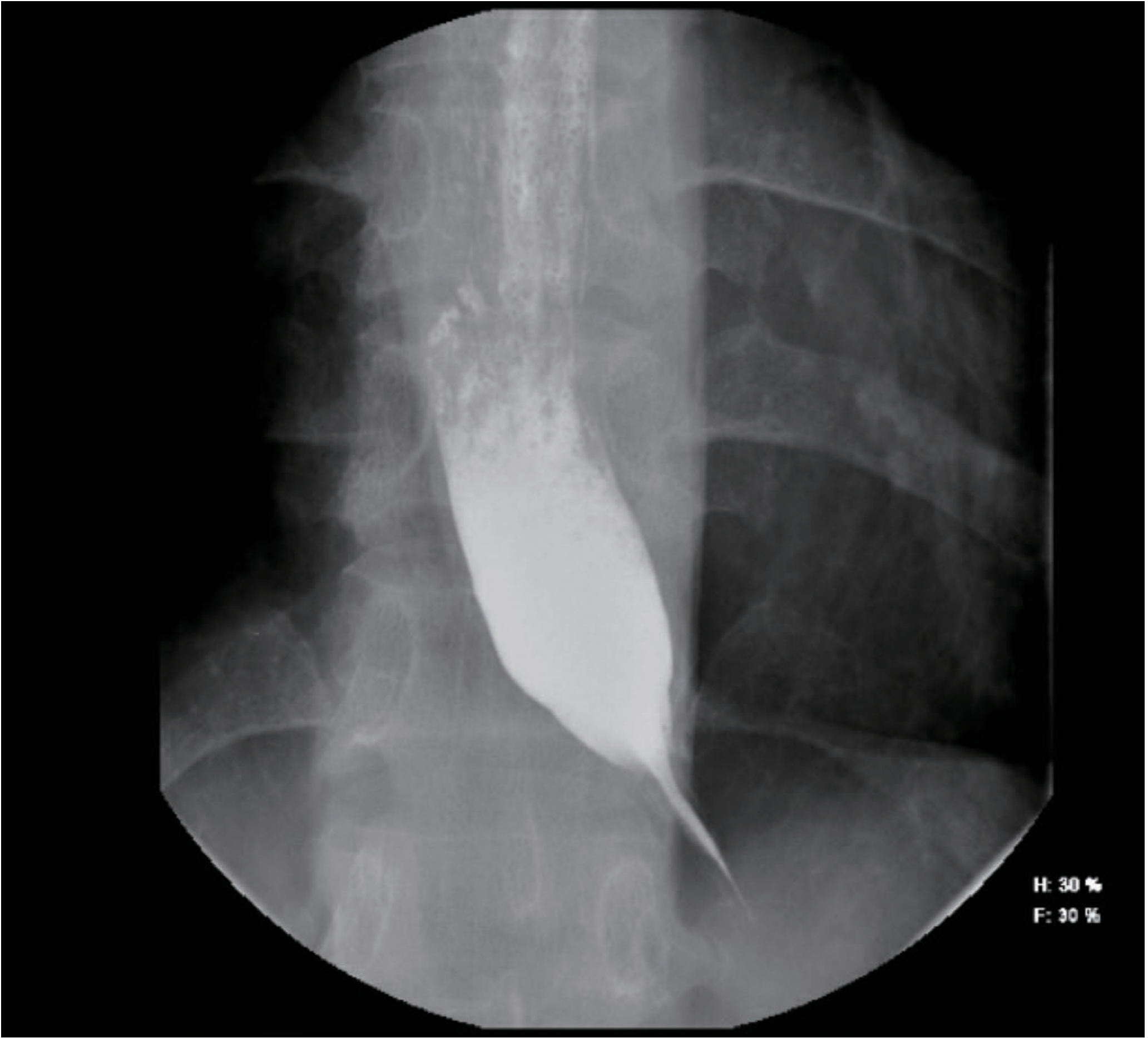
- Timed barium oesophagogram - quantifies contrast column height at fixed time intervals to assess disease severity
- Progressive dilatation leads to sigmoid-shaped / megaoesophagus (end-stage)
- Note: In normal individuals, no air-fluid level is seen in the stomach in achalasia on erect plain X-ray (no air passes through the LOS)
3. High-Resolution Manometry (HRM) - Gold Standard for Definitive Diagnosis
- Elevated Integrated Relaxation Pressure (IRP) across OGJ
- Aperistalsis in smooth muscle oesophagus
- Classifies into Type I, II, III
- Mandatory before any intervention
Complications
- Aspiration pneumonia - from retained food
- Oesophageal carcinoma - chronic retention oesophagitis/fermentation predisposes (squamous cell carcinoma; ~10-33x increased risk)
- Megaoesophagus / sigmoid oesophagus - end-stage with grossly dilated, tortuous oesophagus
- Malnutrition and weight loss
Treatment
Treatment is palliative - there is no therapy to reverse neuronal degeneration. All therapies target LOS reduction.
1. Medical Therapy (Limited Role)
- Calcium channel blockers (nifedipine), nitrates, PDE5 inhibitors - reduce LOS pressure
- Significant side effects (headache, oedema, hypotension)
- Reserved for patients unfit for endoscopic or surgical treatment
2. Botulinum Toxin Injection
- Inhibits presynaptic ACh release, paralyses LOS cholinergic excitatory neurons
- Symptom relief: ~70% at 3 months → ~40% at 1 year
- Effect is temporary - repeated injections required
- Repeated injections may cause scarring, making subsequent treatments more difficult
- Not first-line in patients who are good surgical candidates
- Useful when: diagnosis is in doubt, elderly or high-comorbidity patients
3. Pneumatic Dilatation (PD)
- Non-compliant balloon (30-40 mm) inserted over guidewire to disrupt LOS muscle fibres
- Graded serial dilatation: 30 mm → 35 mm → 40 mm
- Efficacy similar to surgical myotomy in selected patients
- Predictors of good response: age >45 years, female sex, undilated oesophagus, type II achalasia, response to first dilatation
- Complication: perforation (~1.9% average; <0.5% with 30-mm balloon; increases with larger balloons)
- Requires experienced endoscopist and surgical backup
4. Heller's Myotomy (Standard Surgical Treatment)
- Cutting the muscle of the lower oesophagus and gastric cardia (anterior myotomy)
- Extent: ≥6 cm proximally on oesophageal side + 2-3 cm distally into gastric cardia
- Standard approach: laparoscopic (transabdominal)
- Major complication: GORD in up to 40% of patients
- Therefore combined with partial fundoplication:
- Anterior Dor fundoplication or posterior Toupet fundoplication - reduces GORD incidence
- Nissen (360°) fundoplication is CONTRAINDICATED - increases outflow resistance against an aperistaltic oesophagus → postoperative dysphagia
- Laparoscopic myotomy is superior to single pneumatic dilatation in efficacy and durability
- Better outcomes in Type I and II achalasia; Type III needs longer extended proximal myotomy
5. POEM (Peroral Endoscopic Myotomy)
- Mucosa opened proximal to intended myotomy site
- Submucosal tunnel extended to ~2-3 cm into gastric cardia
- Circular ± longitudinal muscles cut with ESD instruments
- Myotomy: minimum 6 cm proximally + 2 cm into gastric cardia
- Mucosal entry site closed with endoclips
- Advantages:
- Equivalent efficacy to PD and Heller's myotomy in RCTs for dysphagia relief
- Can extend myotomy proximally - ideal for Type III achalasia (spastic component)
- Can treat distal oesophageal spasm and hypercontractile oesophagus
- Disadvantage: Higher rate of GORD (no antireflux procedure):
- Oesophagitis at 3 months post-POEM: up to 57%
- May require lifelong PPI or subsequent antireflux surgery
6. Oesophagectomy
- Reserved for end-stage achalasia with sigmoid/megaoesophagus not responding to other methods
- High operative risk vs. risk of aspiration complications must be balanced
- Option for surgically fit patients with grossly dilated oesophagus predisposing to aspiration pneumonia
Comparison of Treatment Options
| Treatment | Efficacy | Durability | GORD risk | Perforation/Leak risk | Notes |
|---|---|---|---|---|---|
| Medical therapy | Poor | - | Low | None | Last resort only |
| Botulinum toxin | 40% at 1 yr | Short | Low | Minimal | Temporary; elderly/unfit |
| Pneumatic dilatation | ~85% | Moderate | Low | ~1.9% | Graded; good for Type II |
| Heller's (lap) + Dor/Toupet | ~90% | Best | ~10-15% with partial fundoplication | Low | Gold standard surgical Rx |
| POEM | ~90% | Good | Up to 57% oesophagitis | Low mucosal injury | Best for Type III |
| Oesophagectomy | Definitive | Definitive | N/A | Highest | End-stage only |
Follow-up
- Treatment success assessed by Eckardt score (target ≤3)
- Counsel on post-treatment diet - oesophageal body motility remains defective
- Surveillance endoscopy for oesophageal carcinoma risk (long-standing achalasia)
- Patients with POEM require monitoring for GORD and possible acid suppression therapy
Bailey and Love's Short Practice of Surgery, 28th Edition, Chapter 66 | Sleisenger & Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.