Explain gout
Reading File
Finding Sources
Searching PubMed
gout pathophysiology management
Reading File
Reading File
Searching PubMed
gout urate lowering therapy
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have a full picture from multiple authoritative textbooks. Here is the comprehensive explanation:
Gout
Gout is a potentially destructive inflammatory arthritis caused by the deposition of monosodium urate (MSU) crystals in joints and soft tissues, occurring in the setting of chronic hyperuricemia (elevated serum uric acid).
Epidemiology
- Affects approximately 4% of adults in the United States; ~5% of adult males and ~3% of adult females.
- Much more common in men (95% of cases), typically presenting in the 4th to 6th decades of life. In women, onset is usually postmenopausal.
- Asymptomatic hyperuricemia is far more common (~19% of individuals in the USA/UK), but only 1 in 8 patients with urate levels of 7-8 mg/dL develop clinical gout over 14 years.
- Risk increases significantly when urate exceeds 9 mg/dL.
Source: Grainger & Allison's Diagnostic Radiology; Rosen's Emergency Medicine
Pathophysiology
Uric Acid Metabolism
Uric acid is the end product of purine catabolism in humans. Purines are produced via two interlinked pathways:
- De novo pathway - purine nucleotides synthesized from non-purine precursors
- Salvage pathway - purine nucleotides recycled from free purine bases
Uric acid is filtered by the glomerulus and nearly completely reabsorbed in the proximal tubule, with only a small fraction secreted distally and excreted in urine.
Causes of Hyperuricemia
| Category | Examples |
|---|---|
| Reduced excretion (most common, ~90%) | Idiopathic; thiazide diuretics; chronic renal disease; cyclosporine |
| Overproduction | Rapid tumor cell lysis (tumor lysis syndrome); HGPRT deficiency (Lesch-Nyhan syndrome); high-purine diet |
- Primary gout (90% of cases): reduced renal excretion of unknown cause
- Secondary gout: medications or underlying disease
Lesch-Nyhan syndrome - complete absence of HGPRT causes profound hyperuricemia plus severe neurologic manifestations (not just gout).
Source: Robbins & Kumar Basic Pathology
Crystal-Induced Inflammation (The Gout Flare)
Hyperuricemia alone is necessary but not sufficient for gout - the plasma urate threshold is >6.8 mg/dL. Only ~10% of hyperuricemic individuals develop gout. Additional factors include duration of hyperuricemia and individual susceptibility.
When urate crystallizes in a joint:
- Resident macrophages in the synovium phagocytose MSU crystals
- This activates the NLRP3 inflammasome (a cytosolic sensor)
- The inflammasome activates caspase-1, producing active IL-1β
- IL-1β drives neutrophil recruitment into the joint
- Neutrophils release cytokines, free radicals, and proteases
- Crystals damage phagolysosomes, causing lysosomal enzyme leakage
- Result: acute, intensely painful arthritis - typically self-limited, resolving in days to weeks
Source: Robbins & Kumar Basic Pathology
Clinical Stages
1. Asymptomatic Hyperuricemia
Elevated uric acid for 20-30 years before symptomatic gout typically appears. No intervention is generally required at this stage.
2. Acute Intermittent Gout (Gout Flare)
Classic presentation:
- Sudden-onset severe joint pain, erythema, swelling, and warmth
- Peak symptoms within 1-2 days, self-limited resolution within a week
- Podagra - acute attack in the 1st metatarsophalangeal joint (in 50% of attacks) - the classic site
Other common sites: knee, ankle, midfoot, tarsal joints, wrist, hand.
Up to 20% of patients have polyarticular involvement. The attack can mimic cellulitis. Systemic fever may be present (which should raise concern for septic arthritis).

3. Intercritical Gout
Asymptomatic periods between attacks. Attacks become more frequent and involve more joints if left untreated.
4. Chronic Tophaceous Gout
Develops when joints are no longer pain-free between attacks:
- Tophi form - gritty, chalk-like nodules of MSU crystal aggregates surrounded by inflammatory tissue
- Found in subcutaneous tissue, bursae, synovial membranes, periarticular tissues
- Cause progressive cartilage destruction and joint dysfunction
- Small joints of hands and feet most commonly affected; large joints (ankle, knee) also involved
Source: Grainger & Allison's Diagnostic Radiology; Rosen's Emergency Medicine
Risk Factors
| Risk Factor | Notes |
|---|---|
| Male sex, older age | Estrogen is uricosuric; postmenopausal women lose this protection |
| Obesity | Increases uric acid production |
| Hypertension & cardiovascular disease | Associated comorbidities |
| Diabetes mellitus | Metabolic syndrome overlap |
| Renal insufficiency | Reduced urate excretion |
| Thiazide diuretics, cyclosporine | Drug-induced hyperuricemia |
| Purine-rich diet | Meats, shellfish, anchovies, legumes, beer |
Diagnosis
Arthrocentesis (Gold Standard)
Synovial fluid analysis is definitive, especially for a first episode or when septic arthritis is on the differential:
- MSU crystals appear as needle-shaped, negatively birefringent crystals under polarized light microscopy (yellow when parallel to the compensator axis)
Serum Uric Acid
- Not reliable during an acute attack - levels can be normal
- Some patients have elevated uric acid without ever developing gout
- Useful for monitoring chronic management
Imaging
Plain X-ray:
- In acute gout: only soft-tissue swelling visible
- In chronic gout: asymmetric, sclerotic "punched-out" periarticular erosions outside the joint capsule (characteristic overhanging edge)
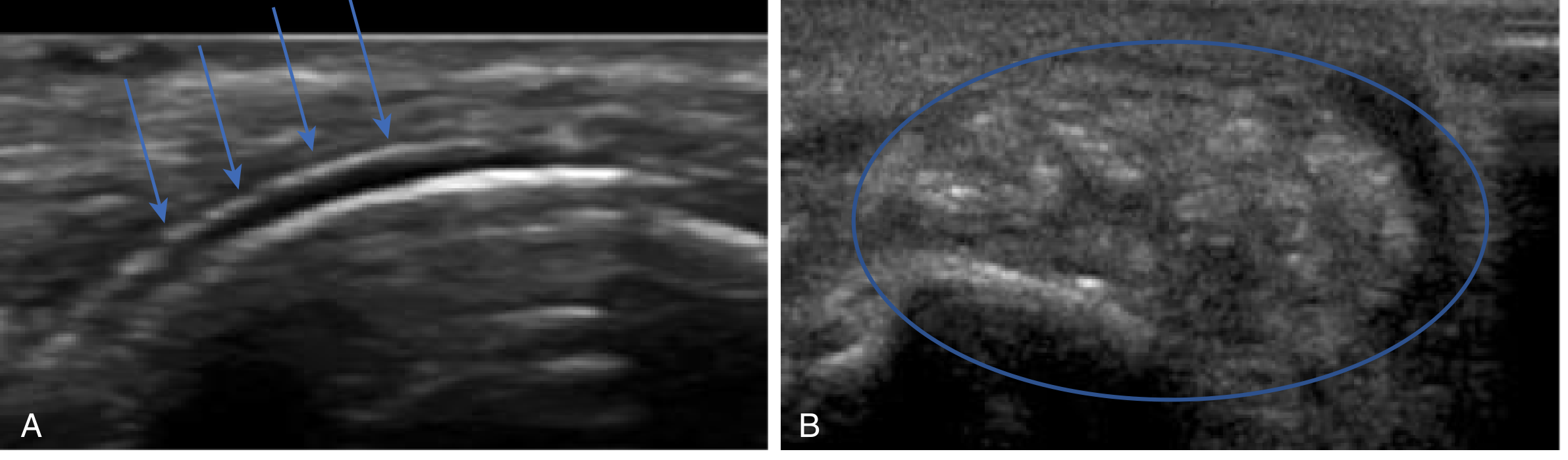
Ultrasound:
- Acute: hyperechoic foci in effusion, synovium, or on cartilage surface
- "Double contour sign" - hyperechoic line over cartilage surface (crystals overlying the bone)
- Tophi appear as "wet clumps of sugar" - heterogeneous center with hypoechoic rim
Renal function should be assessed, given the association with renal insufficiency and nephrotoxicity of many gout medications.
Management
Acute Flare Treatment
All three options (NSAIDs, colchicine, corticosteroids) are effective. There is no strong evidence favoring one over another.
| Drug | Mechanism | Notes |
|---|---|---|
| NSAIDs (indomethacin, naproxen, ibuprofen) | COX inhibition, anti-inflammatory | First-line; avoid in PUD, GI bleeding, renal insufficiency |
| Colchicine | Inhibits microtubule formation - blunts crystal-triggered inflammation | Effective; contraindicated in renal/hepatic failure; narrow therapeutic window; GI side effects common |
| Corticosteroids (oral prednisone 40 mg/day x 5-7 days, or intra-articular) | Anti-inflammatory | Useful when NSAIDs/colchicine contraindicated; intra-articular most effective for single joint; avoid oral NSAID + oral steroid combination (GI risk) |
- Topical ice and joint rest are also helpful adjuncts.
- Do not start urate-lowering therapy during an acute flare, but continue chronic urate-lowering drugs already in use.
Long-Term Urate-Lowering Therapy (ULT)
Target serum uric acid: <6 mg/dL in symptomatic patients.
| Drug | Class | Notes |
|---|---|---|
| Allopurinol | Xanthine oxidase inhibitor (purine analog) | First-line ULT; start at 100-200 mg/day; increase in 50-100 mg increments; dose-adjust for renal function |
| Febuxostat | Non-purine xanthine oxidase inhibitor | Use in allopurinol-allergic patients; 40-80 mg/day; no renal dose adjustment; CARES trial showed higher CV/all-cause mortality vs allopurinol in high-CV-risk patients |
| Probenecid | Uricosuric | Blocks renal tubular urate reabsorption; less commonly used |
| Pegloticase | Recombinant pegylated uricase | Converts urate to allantoin (more soluble); FDA approved 2010 for refractory gout; risk of anti-drug antibodies causing infusion reactions and loss of efficacy |
Important drug interaction: Both allopurinol and febuxostat inhibit xanthine oxidase, the enzyme that metabolizes azathioprine. Concurrent use causes azathioprine toxicity - dose reduce azathioprine by ~25% and monitor CBC closely, or switch azathioprine to mycophenolate.
Anti-inflammatory Prophylaxis
Low-dose colchicine or NSAIDs are used during initiation of ULT to prevent flares triggered by urate mobilization. A 2025 meta-analysis (Stamp et al., PMID 39711080) found increased flare risk after stopping anti-inflammatory prophylaxis, supporting gradual discontinuation.
Lifestyle Modifications
- Reduce dietary purines (red meat, organ meat, shellfish, beer)
- Reduce alcohol (especially beer; fructose-containing beverages also raise urate)
- Maintain hydration
- Achieve and maintain healthy weight
- Switch diuretics if clinically possible
Key Associations
- Lesch-Nyhan syndrome - X-linked complete HGPRT deficiency; severe gout + neurologic disease (intellectual disability, self-mutilation, spasticity)
- Tumor lysis syndrome - massive purine release from dying cancer cells after chemotherapy - can cause acute severe gout and acute kidney injury
- Renal urate nephropathy - urate crystals can precipitate in renal tubules, causing obstructive uropathy
- Cardiovascular disease - gout is independently associated with hypertension, heart failure, and CAD; a 2024 meta-analysis (Lee & Song, PMID 39636389) confirmed ULT reduces all-cause and CVD-specific mortality in gout
Sources: Robbins & Kumar Basic Pathology; Rosen's Emergency Medicine; Grainger & Allison's Diagnostic Radiology; Comprehensive Clinical Nephrology, 7th Ed.; Firestein & Kelley's Textbook of Rheumatology; Lippincott Biochemistry, 8th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.