Amoebiasis
Reading File
Finding Sources
Searching PubMed
"amoebiasis" OR "Entamoeba histolytica"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information. Let me compile the full response.
Amoebiasis
Definition
The WHO defines amoebiasis as the condition of harbouring the protozoan parasite Entamoeba histolytica with or without clinical manifestations. Symptomatic disease occurs in fewer than 10% of infected individuals. - Park's Textbook of Preventive and Social Medicine, p. 283
Epidemiology
-
Worldwide distribution; major health problem in China, South East and West Asia, Latin America (especially Mexico), the Indian subcontinent, Africa, and parts of Central and South America
-
Globally, ~50 million people carry E. histolytica; approximately 1 in 10 infected individuals develop invasive disease; ~50,000 deaths per year estimated
-
Prevalence in stool samples in high-endemic zones averages 10%; incidence of amoebic liver abscesses can reach 21 per 100,000 population
-
India: approximately 15% of the population is affected (ranging 3.6-47.4% in different areas)
-
More prevalent in lower socioeconomic groups due to poor sanitation
-
Bailey and Love's Short Practice of Surgery 28th Ed., p. 88; Park's, p. 283
Aetiology and Agent Factors
Organism: Entamoeba histolytica - exists in two forms:
| Form | Features |
|---|---|
| Trophozoite (vegetative) | Active form; dwells in colon; short-lived outside the body; not important in transmission |
| Cyst | Infective form; excreted in stool; survives days-weeks in faeces, water, sewage, soil; not killed by chlorine at routine water purification concentrations; killed by drying, heat (55°C), or freezing |
- E. histolytica can be differentiated into at least 18 zymodemes; 7 are pathogenic, 11 are non-pathogenic
- Man is the only reservoir of infection
- Healthy carriers can discharge up to 1.5 × 10⁷ cysts daily
- Period of communicability: as long as cysts are excreted (potentially years if untreated)
Mode of Transmission
- Faecal-oral route (primary) - contaminated water or food; raw vegetables from sewage-irrigated fields; direct hand-to-mouth via contaminated fingers
- Sexual transmission - oral-rectal contact, especially in men who have sex with men
- Vectors - flies, cockroaches, and rodents can carry cysts and contaminate food
Incubation period: approximately 2-4 weeks (or longer)
Pathogenesis
Intestinal pathway:
- Ingested cysts hatch in the small bowel releasing trophozoites, which are carried to the colon
- Trophozoites invade the submucosa producing characteristic "flask-shaped" (bottleneck) ulcers - these have considerably undermined edges and a yellow necrotic floor, with blood and pus
- Typical sites: caecum and ascending colon most commonly; then rectum and sigmoid
Hepatic pathway:
-
Trophozoites enter the portal circulation and are trapped in the interlobular veins of the liver
-
They cause focal infarction and liquefactive necrosis via proteolytic enzymes
-
Areas of necrosis coalesce to form an abscess cavity
-
Right lobe involved in 80% of cases, left lobe 10%, remainder are multiple - the right lobe is more often affected because blood from the superior mesenteric vein takes a straighter course through the portal vein into the larger lobe
-
Abscesses most common on the high diaphragmatic surface of the right lobe, potentially causing pulmonary symptoms
-
Abscess cavity contains chocolate-coloured, odourless "anchovy sauce"-like fluid (necrotic liver tissue + blood)
-
"Amoebic hepatitis" refers to the microscopic picture before macroscopic abscess forms
-
Bailey and Love's, p. 88
Clinical Features
Intestinal Amoebiasis
- Ranges from mild abdominal discomfort and diarrhoea to acute fulminating dysentery (bloody mucoid diarrhoea)
- Can clinically mimic ulcerative colitis
- Complications: haemorrhage, stricture, perforation, pericolitis with adhesions causing intestinal obstruction
Amoebic Liver Abscess
Typical patient: young adult male, insidious onset of:
- Non-specific: abdominal pain, anorexia, fever, night sweats, malaise, weight loss
- More specific: right upper abdominal pain, right shoulder tip pain, hiccoughs, non-productive cough
- Past history of bloody diarrhoea or travel to endemic area raises suspicion
On examination: toxic, anaemic patient; upper abdominal rigidity; tender hepatomegaly; bulging tender intercostal spaces; skin oedema; pleural effusion; basal pneumonitis (late finding); occasional jaundice or ascites
Emergency presentation may occur if abscess ruptures into the peritoneal, pleural, or pericardial cavity.
Amoeboma
- A chronic granulomatous lesion in the large bowel, most commonly the caecum
- Occurs in long-standing infection treated incompletely (intermittent/self-medication)
- Appears as a mass in the right iliac fossa with generalised ill health, pyrexia, and blood-stained mucoid diarrhoea
- Easily mistaken for carcinoma - always biopsy
Histological Appearance
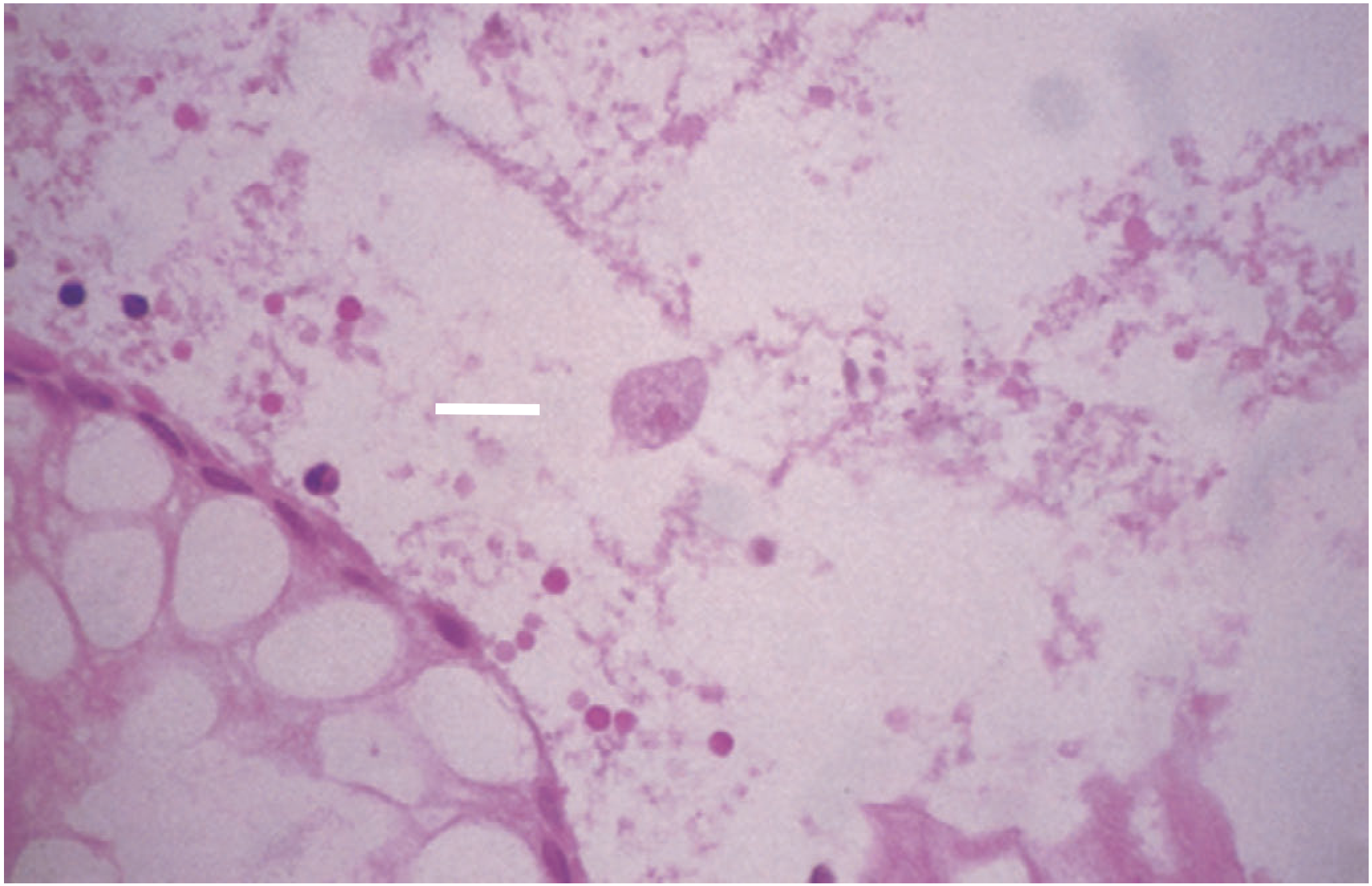
Amoeba in a rectal biopsy (arrow). Note the large trophozoite with ingested red cells amid background necrotic tissue.
Diagnosis
Laboratory
- Stool microscopy: Demonstration of trophozoites containing ingested red cells is diagnostic - must be performed on fresh, warm specimens (cooling destroys motility); mucus from rectal swabs is ideal
- Absence of pus cells in stool helps distinguish from shigellosis
- Endoscopic biopsy or stool examination for amoebae (note: presence of parasite alone doesn't confirm pathogenicity)
Serology
- Complement fixation, indirect haemagglutination (IHA), indirect immunofluorescence, counter-immunoelectrophoresis (CIE), ELISA
- IHA is the most sensitive serological test for acute amoebic liver abscess in non-endemic regions
- In endemic areas, persistent antibodies in healthy population limit serological utility
- Antigen detection or PCR combined with serology improves specificity
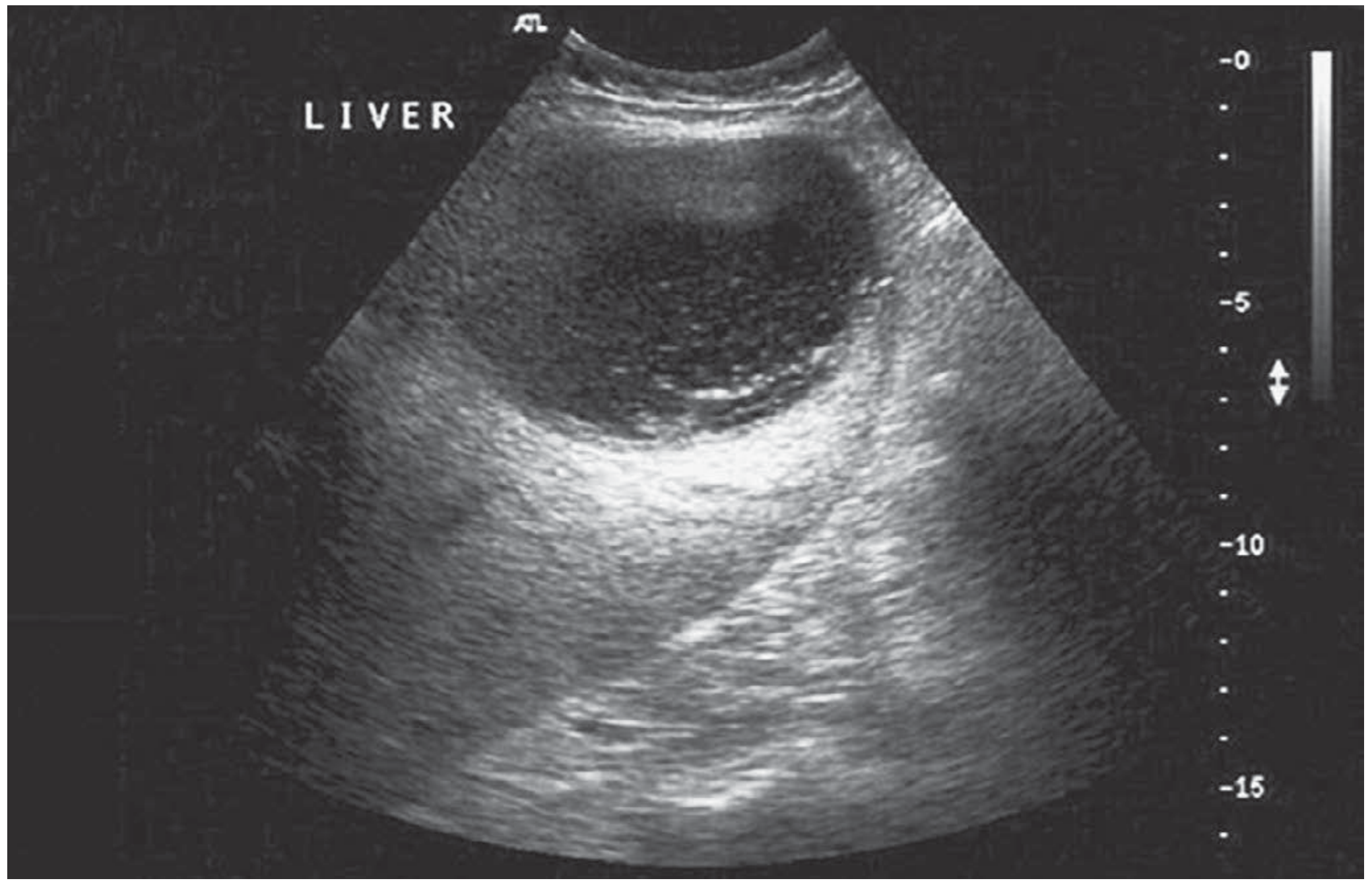
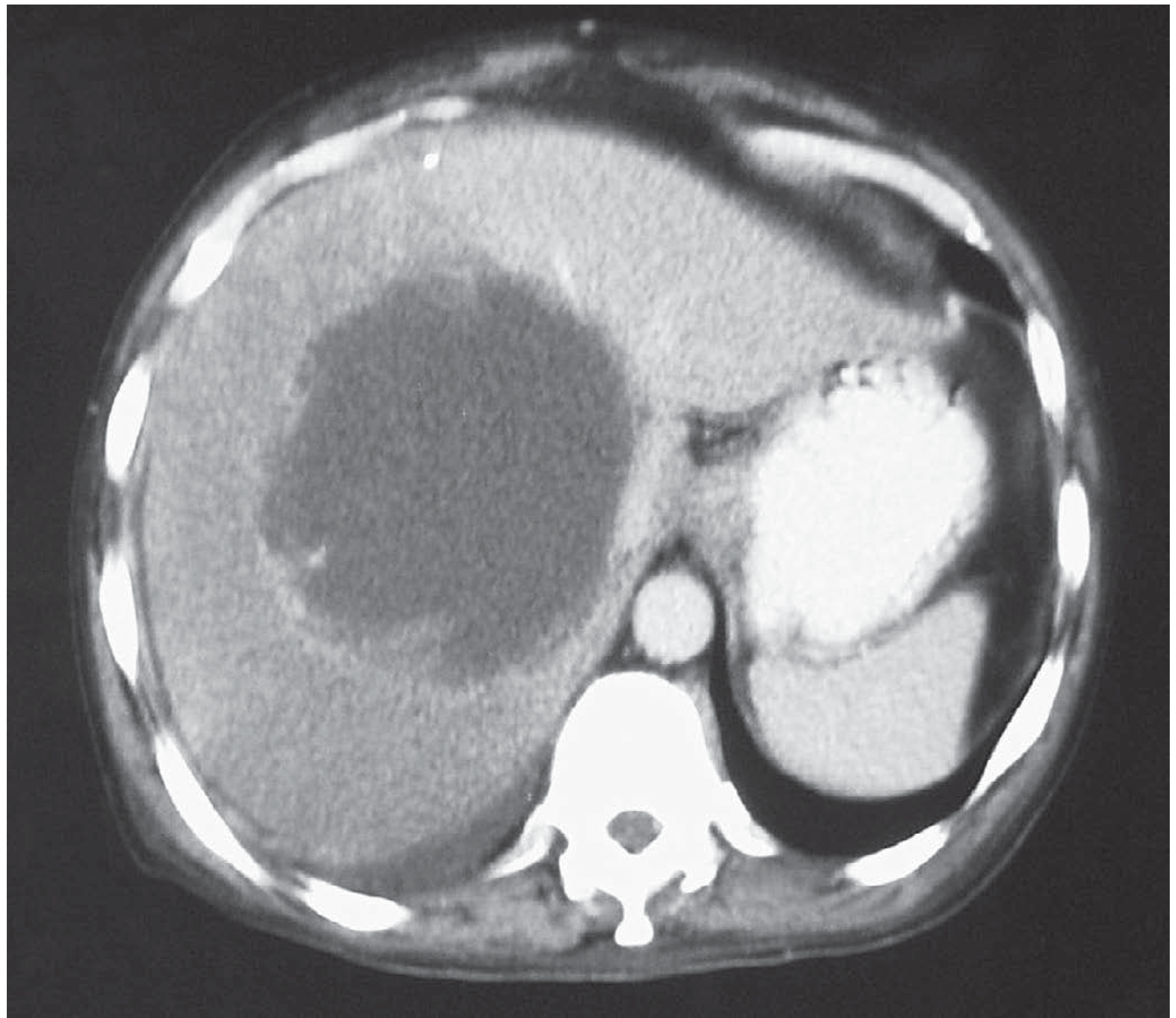
Imaging
Ultrasonography - first-line imaging: abscess appears as hypoechoic/anechoic lesion with ill-defined borders; used for aspiration (diagnostic and therapeutic):
CT scan - confirms diagnosis, shows raised right hemidiaphragm, pleural effusion, pneumonitis, and any complications.
Colonoscopy: reveals discrete exudate-covered ulcers with normal mucosa in between; biopsy mandatory if amoeboma suspected to exclude carcinoma.
Treatment
Medical (First-line)
| Drug | Role | Dose |
|---|---|---|
| Metronidazole | Tissue amoebicide (acute phase) | 30 mg/kg/day in 3 divided doses after meals × 8-10 days |
| Tinidazole | Tissue amoebicide (alternative to metronidazole) | - |
| Diloxanide furoate | Luminal amoebicide (used after metronidazole/tinidazole to eradicate intestinal cysts) | 10 days course |
Note: Diloxanide furoate is not effective against hepatic disease - it targets luminal/intestinal amoebae only.
Aspiration and Drainage
- Aspiration is carried out when imminent rupture is expected, especially left lobe abscesses
- Pigtail catheter drainage if no response to IV metronidazole within 48-72 hours
- Low threshold for draining left lobe abscesses (propensity to rupture into peritoneal, pleural, or pericardial cavity)
- Diagnostic aspiration: limited value except to confirm typical "anchovy sauce" appearance and sterility (unless secondarily infected)
Surgery (Reserved for Complications)
-
Rupture into pleural, peritoneal, or pericardial cavity: resuscitation, drainage, lavage + vigorous medical treatment
-
Acute toxic megacolon or severe haemorrhage: subtotal colectomy with terminal ileostomy and closure of rectal stump
-
Amoeboma: first confirm cancer excluded by imaging and biopsy; these masses can resolve with vigorous medical treatment (re-colonoscopy in 3-4 weeks)
-
Bailey and Love's, p. 89-90
Prevention and Control
Primary prevention:
- Sanitation: safe disposal of human excreta; hand washing after defecation and before eating
- Water supply: filtration and boiling are more effective than chemical disinfection (cysts survive routine chlorination); sand filters effectively remove cysts
- Food hygiene: aqueous acetic acid (5-10%) or full-strength vinegar can disinfect uncooked vegetables and fruits; thorough washing with detergents removes cysts; food handlers should be periodically examined and treated
- Health education
Secondary prevention (early diagnosis and treatment):
-
Symptomatic cases: metronidazole orally; response within 48 hours confirms suspected diagnosis
-
Asymptomatic infections in endemic areas: generally not treated (consensus)
-
Park's, p. 284
Key Differentiating Points
| Feature | Amoebiasis | Ulcerative Colitis |
|---|---|---|
| Microscopy | Amoebae (trophozoites) in stool/biopsy | No organism |
| Serology | Often positive (IHA) | Negative |
| Ulcer type | Flask-shaped, discrete, skip areas | Continuous, shallow |
| Response | Rapid response to metronidazole | No response to metronidazole |
| Risk | Endemic area travel, poor sanitation | Often no such history |
Important: Always exclude amoebic infection before starting steroids in a patient suspected of having ulcerative colitis - steroids in unrecognized amoebiasis can precipitate fulminant colitis.
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.